
Abstract
Objective:
Vertigo and dizziness are the common presenting concerns in emergency departments and outpatient clinics, accounts for approximately 15% to 20% of adults annually. We aimed to evaluate economic burden of vertigo on health-care system and work productivity in association between clinic characteristics of in- or outpatients.
Methods:
A total number of 2289 patients diagnosed with peripheric (noncentral) vertigo were evaluated retrospectively. The direct medical costs associated with vertigo classified as medication, consumable, imaging, and laboratory. In addition, the indirect costs were associated with lost working days. The overall economic impact of vertigo assessed via total expenditure for diagnosis and treatment.
Results:
The mean duration of hospitalization was 5.6 ± 4.3 days and working day lost was 9.47 ± 3.90 days. The overall impact on work productivity of disease was 15.35 ± 6.11 days. The overall mean direct cost including all expenditure items associated with vertigo care was $250.25 ± $1479.62 per patient. The overall cost associated with vertigo was found to be statistically increased in the male, aged ≥65 years, widow or divorced, and hospitalized patients.
Conclusions:
Our findings clearly indicate that a vertigo–dizziness management program based on patients’ risk factors may achieve to reduce hospitalizations and cost of hospital care as well.
Introduction
Vertigo is defined as a perceived illusion of motion of either the self or the environment in the absence of true physical movement. 1 Dizziness, which is one of the most common presenting concern in emergency departments (EDs) and outpatient clinics, affects approximately 15% to 20% of adults annually. 2 Vertigo comprises about a quarter of total dizziness complaints with a reported 12-month prevalence of 5%, according to the population-based studies. 3 Additionally, its prevalence increases with age and more frequent among female gender. 4
Since the vertigo and dizziness are major complaints lead individuals to present to the medical departments, it is increasingly recognized as a major health and economic burden worldwide. Seeking medical care due to the symptoms of vertigo associated with higher costs in recent studies. 5,6 Researches also suggested that vertigo has significant impact on work productivity, such that severe vertigo symptoms may lead patients to quit or change their jobs. 7
As vertigo more frequently occurs in elderly population, hospitalized patients increase gradually in aging populations. Thus, hospitalization costs increase substantially with increasing number of the hospitalized patients. 6,7 On the other hand, vertigo has significant health-care costs that includes charges of the medications, laboratory, and imaging tests. 5,7 Moreover, varied health-care costs between hospitalized and outpatients with dizziness also documented. 5 Thus, accurate disease management may contribute to allocate medical resources efficiently. Therefore, we aimed to evaluate economic burden of vertigo on health-care system and work productivity in association between inpatient admissions and hospitalization of the vertigo patients.
Materials and Methods
A total number of 2289 patients diagnosed with peripheric (noncentral) vertigo were evaluated retrospectively in present study. Outpatients whose symptoms did not improve with treatment were hospitalized. Data were collected from database of Ministry of Health Samsun Education and Research Hospital Turkish lira. The direct medical costs associated with vertigo classified as medication, consumable, imaging, and laboratory. In addition, the indirect costs were associated with lost working days in vertigo patients. The overall economic impact of vertigo assessed via total expenditure for diagnosis and treatment of patients with vertigo. Sociodemographic data such as age, gender, marital status as well as information including treatment duration and discharge data of hospitalized patients were recorded and evaluated. All costs calculated in Turkish lira initially and converted to the US dollars by using the exchange rate of April 24, 2019 (1TL = $5.85).
Statistical Analysis
All the data were analyzed with SPSS (Statistical Package for the Social Sciences) software for Windows (v21.0; IBM, Armonk, New York). Individual and aggregate data were summarized using descriptive statistics including mean, standart deviations, medians (min–max), frequency distributions, and percentages. Normality of data distribution was verified by Kolmogorov-Smirnov test. Comparison of the variables with normal distribution was made with Student t test and paired sample t test. The variables that were not normally distributed, the Mann-Whitney U and Kruskal-Wallis tests were conducted to compare between groups. Evaluation of categorical variables was performed by χ2 test. P values of <.05 were considered statistically significant.
Results
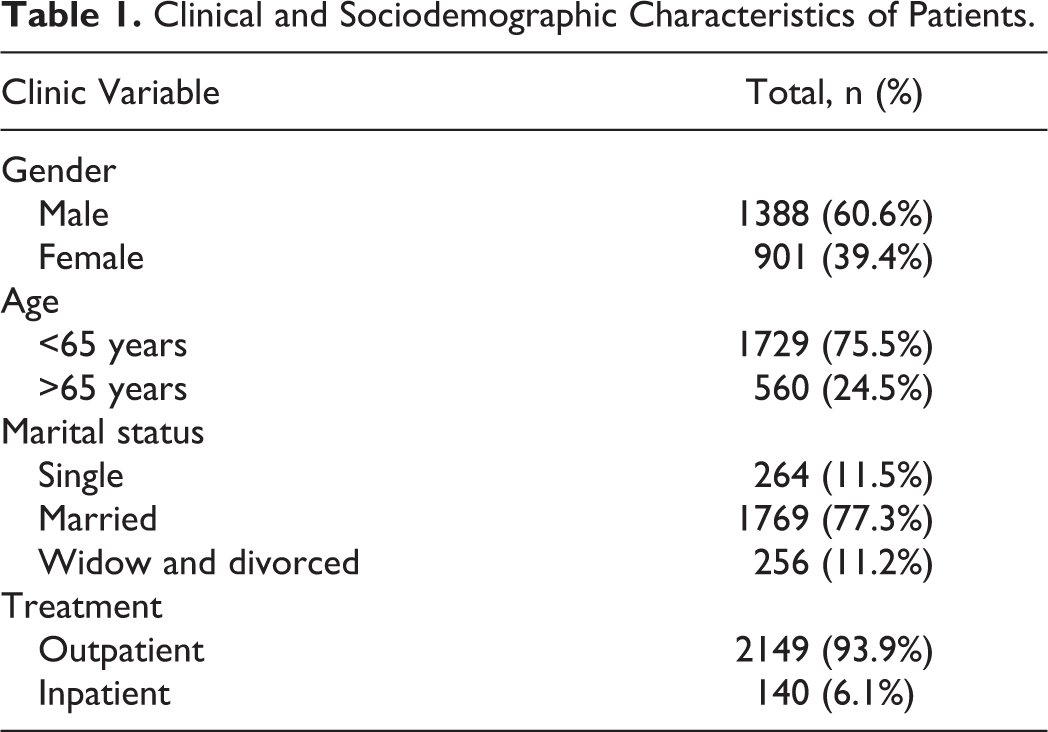
The 2289 patients included in this study were 901 (39.4%) male, 1388 (60.6%) female, and the mean age of total participants was 50.58 ± 17.90 years. Of the participants, 2149 (93.9%) were outpatients and 140 (6.1%) were inpatients. The mean duration of hospitalization was 5.6 ± 4.3 (range: 1-31) days. The mean working day lost was 9.47 ± 3.90 (range: 5-20) days after discharge from hospital. The overall impact on work productivity of disease was 15.35 ± 6.11 days. Patients were separated into 2 groups according to their ages: <65 years old and 65 or older; 75.5% (n = 1729) were aged below 65 and 24.5% (n = 560) were aged 65 and above. According to the sociodemographic characteristics of the patients, 77.3% (n = 1769) were married, 11.2% (n = 256) were widowed or divorced, and 11.5% (n = 264) were single (Table 1).
Clinical and Sociodemographic Characteristics of Patients.
The mean medication cost was determined as $87.36 ± $612.86, and the mean cost of consumable was $32.16 ± $367.24 for all patients. Additionally, the average laboratory cost of all patients was calculated as $33.68 ± $116.47, and the mean cost of imaging was $55.47 ± $145.22. Moreover, the total average cost of all medication and consumables was determined as $161.08 ± $131.19. The overall mean direct cost including all expenditure items associated with vertigo care was $250.25 ± $1479.62 per patient.
According to the evaluation of treatment costs in association between clinical and sociodemographic characteristics of the patients, the average costs of medication and consumables measured in the group with aged 65 or older were found to be statistically higher than in group with aged lower than 65 (P = .000 and .000, respectively). In addition, the average costs of medication and consumables in hospitalized patients were found to be significantly higher than outpatients (P = .000 and .000, respectively). There were no statistically significant gender differences found according to the average costs of medication and consumables (P > .05; Table 2).
Comparison of Medication and Consumable Costs According to the Patients Characteristics
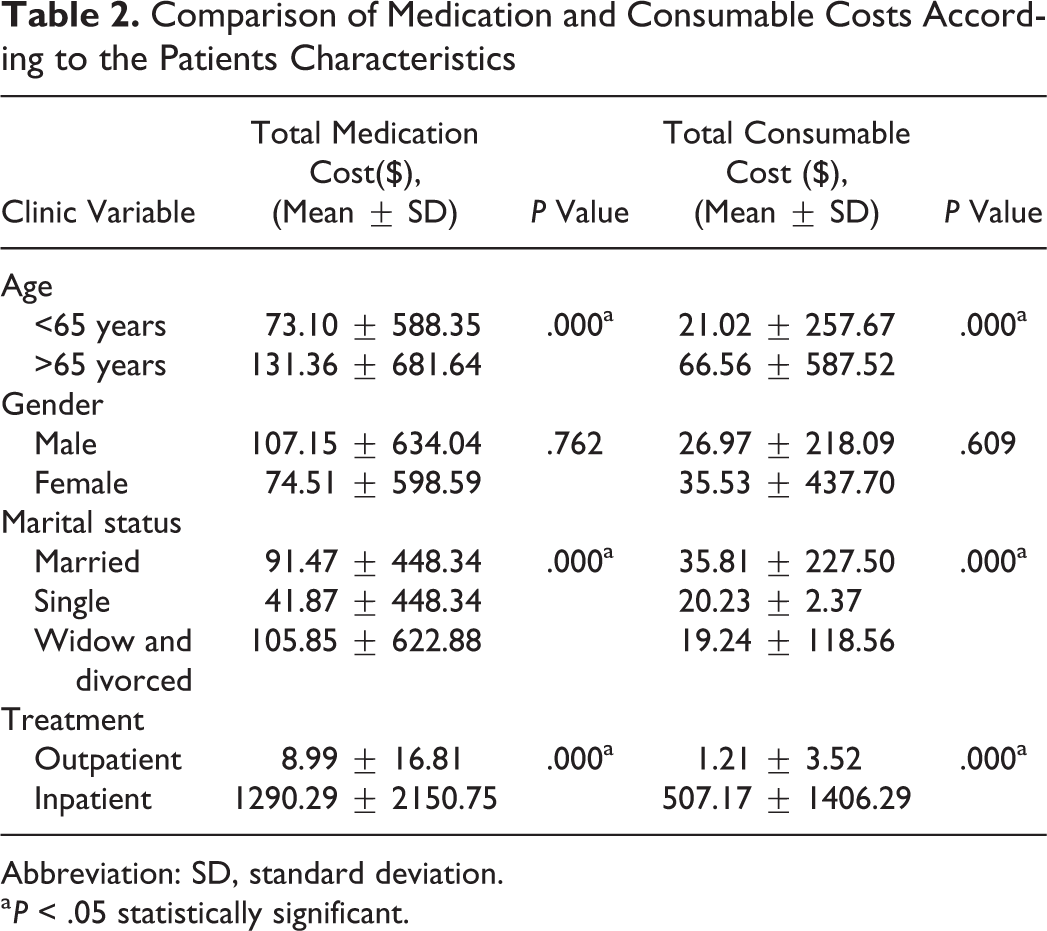
Abbreviation: SD, standard deviation.
a P < .05 statistically significant.
The mean laboratory expenditures were found to be statistically increased in the male, aged ≥65 years, widow or divorced, and hospitalized patients (P = .002, .000, .000, and .000, respectively). Similarly, the mean imaging costs determined in the male, aged ≥65 years, widow or divorced, and hospitalized patients were found to be statistically increased (P = .000, .000, .000, and .000, respectively; Table 3).
Comparison of Laboratory and Imaging Costs According to the Patients Characteristics.
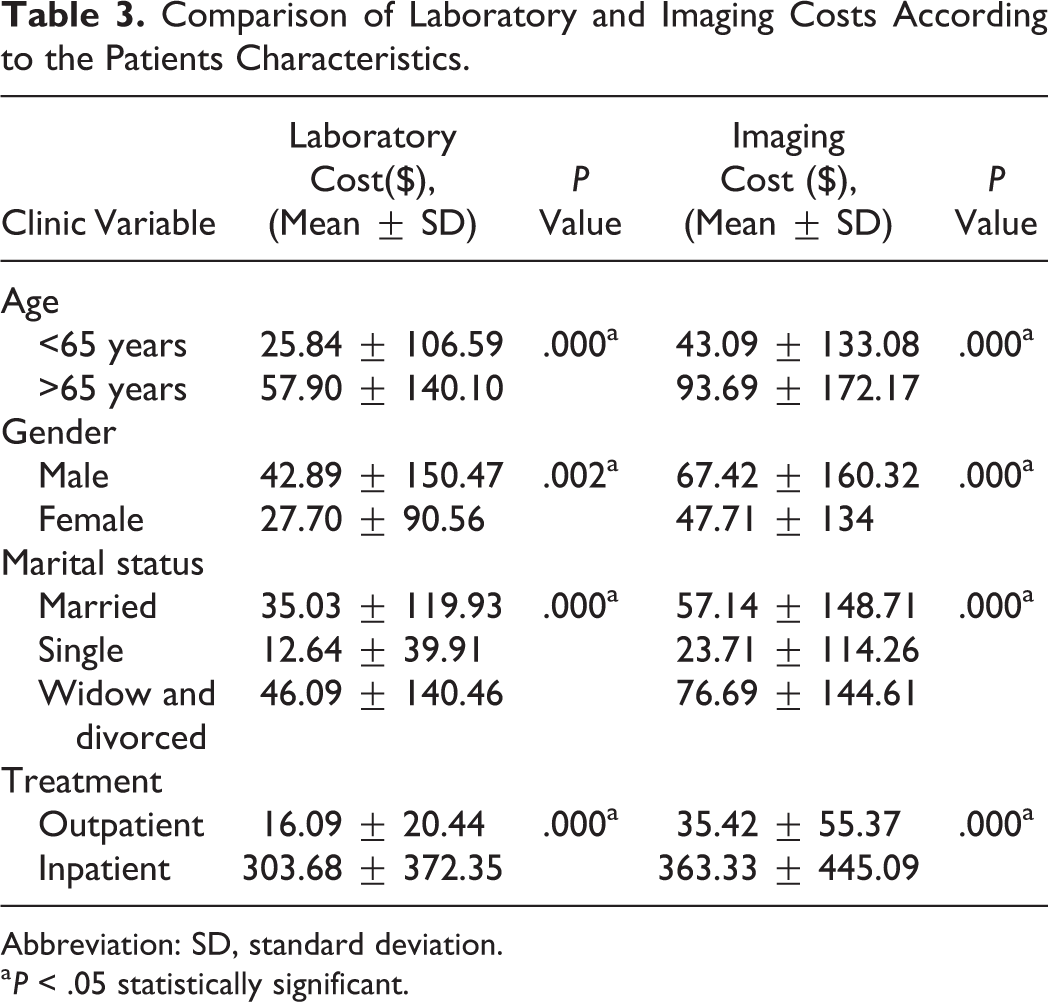
Abbreviation: SD, standard deviation.
a P < .05 statistically significant.
According to the evaluation of total treatment costs in association between clinical and sociodemographic characteristics of the patients, the average costs of total medication and consumables calculated in the aged ≥65 years and hospitalized patients were found to be statistically higher than aged <65 years and outpatients (P = .000 and .000, respectively). Moreover, the overall direct cost including all medication, consumables, laboratory, and imaging expenses associated with vertigo was detected to be statistically increased in the male, aged ≥65 years, widow or divorced, and hospitalized patients (P = .000, .000, .000, and .000, respectively; Cohen d = 0.156, 0.063, 0.001, and 0.833, respectively; Table 4). Furthermore, there were positive–moderate statistically significant correlation detected between total cost and age of patients (r = 0.381, P = .000).
Comparison of Overall Costs According to the Patients Characteristics.
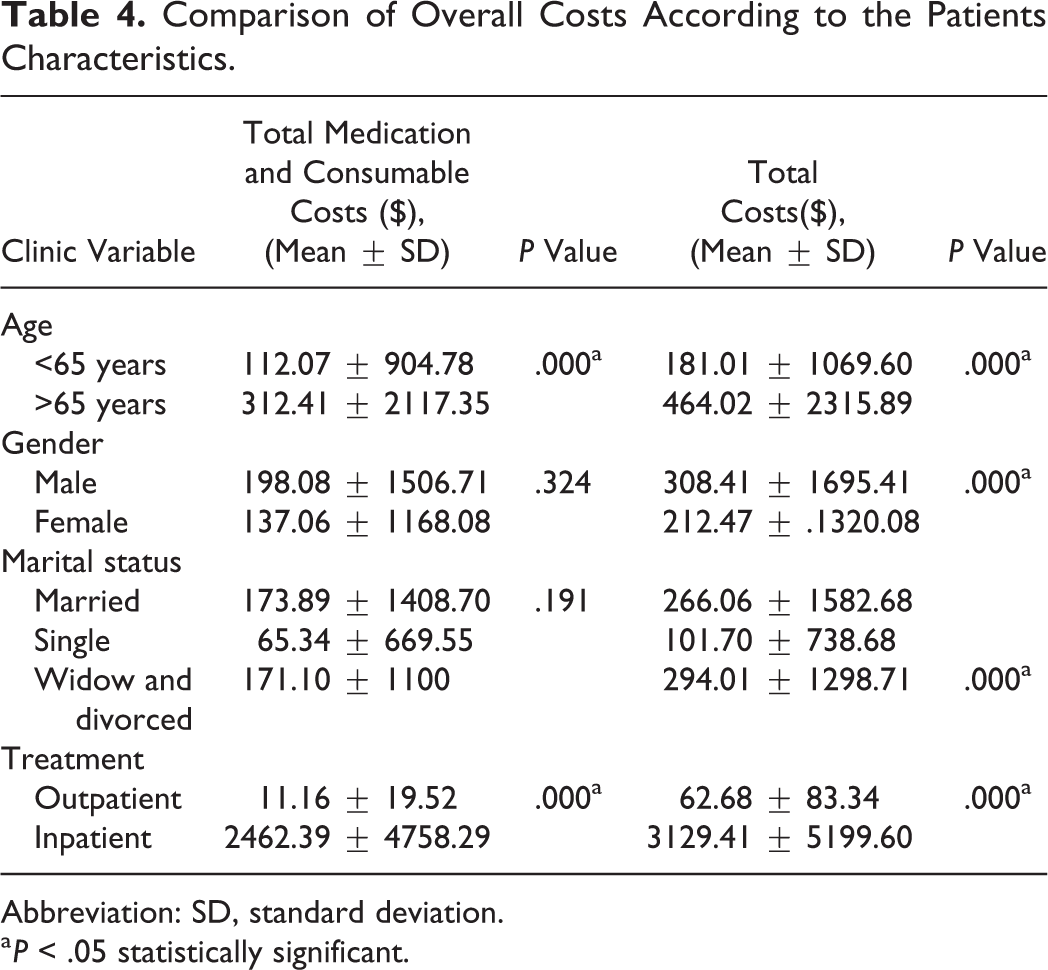
Abbreviation: SD, standard deviation.
a P < .05 statistically significant.
Discussion
Dizziness and vertigo are the common complaints in medicine, accounting for the 20% to 30% of the general population. 3 Therefore, these common symptoms have significant burden on health-care systems. The recognition of impact on its economic burden can only achieve with more researches that evaluating epidemiologic data, risk factors, and clinic characteristics of symptoms. 8 There are limited published data evaluating economic burden of vertigo. Reis et al documented increased ED visit rate among elderly population in a study conducted with 4347 patients with dizziness. 9 Benecke et al reported a reduction workload in 69.8% and lost of working days in 63.3% of vertigo patients in a study involved 4294 vertigo patients at 618 centers in 13 countries. Additionally, researchers reported that vertigo symptoms lead 4.6% of patients changed and 5.7% of patients quit their jobs. Moreover, they documented mean hospital stay of 2.7 days for 13 countries; in Ukraine, mean duration of hospital stay was 7.6 days, and in Russia, it was 5.3 days. 7 Similarly in our study, the mean duration of hospitalization was 5.6 ± 4.3 days and the mean working day lost was 9.47 ± 3.90 days after discharge from hospital. The overall impact on work productivity of vertigo was estimated to be 15.35 ± 6.11 days.
Data from National Hospital Ambulatory Medical Care (1995-2009) and Medical Expenditure Panel Survey (2003-2008) in United States revealed 3.9 million ED visits for dizziness or vertigo in 2011. The total annual cost of ED visit $3.9 billion. Additionally, 12% of the total cost was attributed to the imaging. Researchers concluded that dizziness and vertigo management is exceedingly costly. 5 Similarly, Becares-Martinez et al reported an imaging costs of €56 741 which of more than 90% was not even related to vertigo in 493 patients. 6 Similarly, Kerber et al reported a median of 3.6 tests (laboratory or imaging) at each ED visit for vertigo-dizziness between 1995 through 2004. Researchers also highlighted a gradually increased (169%) tests utilization in time. 10 In present study, we evaluated not only the total costs of disease burden but also evaluated expenditures of medication, consumable, imaging, and laboratory separately. Thus, the mean medication and consumable cost was $87.36 ± $612.86 and $32.16 ± $367.24, respectively. Additionally, the average laboratory cost of all patients was calculated as $33.68 ± $116.47, and the mean cost of imaging was $55.47 ± $145.22. Moreover, the overall direct cost including all expenditure items associated with vertigo care was $250.25 ± $1479.62 per patient.
To our knowledge, this study is the first overview of estimated total costs for vertigo in association between clinic characteristics of in- or outpatients. Le et al assessed the hospital cost of dizziness or dizziness-related diseases between 2009 and 2014 in Canadian patients. Researchers reported a mean age of 55.9 years, of the 12 186 patients with majority diagnosis of dizziness and benign paroxysmal vertigo; 59.3% were females, additionally researchers documented a total estimated hospital cost of $31 202 000 annually. Moreover, it was also stated that the mean total cost per patient was $450 ± $1333.68, but with inpatients only (n = 93) was $6978.94 ± $9991.16 in same study. 11 In addition, Benecke et al concluded that health-care utilization is increasing by disease severity and advanced age, according to the Registry to Evaluate the Burden of Disease in Vertigo (REVERT) data. 7 Lai et al also stated vertigo as a major health burden in particularly older women. 8 Supportively, the 2289 patients included in present study were 39.4% male, 60.6% female, and the mean age of total participants was 50.58 ± 17.90 years. Of the participants, 2149 (93.9%) were outpatients and 140 (6.1%) were inpatients. The mean laboratory and imaging costs were found to be statistically increased in the male, aged ≥65 years, widow or divorced, and hospitalized patients. Additionally, the average costs of total medication and consumables calculated in the aged ≥65 years and hospitalized patients were found to be statistically higher than aged <65 years and outpatients. Moreover, the overall direct cost including all medication, consumables, laboratory, and imaging expenses associated with vertigo was found to be statistically increased in the male, aged ≥65 years, widow or divorced, and hospitalized patients. Furthermore, there were positive–moderate statistically significant correlation detected between total cost and age of patients. It is well known that patients having dizziness and vertigo also manifest higher comorbidity with psychological disorders, which have significant impact on quality of life. 11 Impaired life quality in vertigo patients may influence on personal care and also work performance, consequently leading increased health-care utilization. This could be possible explanation of higher costs obtained from widow or divorced patients in our study.
On the other hand, it is possible to reduce costs of hospital care with effective management of diseases. Supportively, Statile et al achieve to reduce cost of dizziness/syncope management from $1784 to $1098 per patient by standardization of symptom evaluation. 12 Similarly, Bjorne and Agerberg performed a coordinated treatment of temporomandibular and cervical spine disorders in 24 patients with Meniere disease and documented an average sick leave decrease of 66.6 days after 3 years period of treatment. 13
In conclusion, our findings clearly indicate that a vertigo–dizziness management program based on patients’ risk factors may achieve to reduce hospitalizations and cost of hospital care as well. Moreover, the underestimation of vertigo symptoms may subsequently result with a greater economic burden due to the possible underlying disorders particularly in aging individuals.
Conclusion
In addition to the negative impact on the patient, vertigo has considerable impact on work productivity and health-care resource use. Our findings show the importance of determining the causes of hospitalization in vertigo patients economically. Determination of hospitalization and treatment methods of these patients may alleviate the economic burden. In this respect, further multicenter designed researches should be performed with larger study groups to alleviate economic burden of vertigo and utilize health-care resources efficiently.
Footnotes
Authors’ Note
Informed consent was obtained from all individual participants included in the study. Institutional review board protocol approval number: 95-2018; Institutional review board protocol approval number date: 5 July 2018.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.