
Abstract
Objective:
The aim of this study was to compare the functional and aesthetic outcomes of endonasal septoplasty (ES) and extracorporeal septal reconstruction (ESR) in anterocaudal septal deviation.
Methods:
In this study, patients (n = 46) who underwent nasal septoplasty surgery due to anterocaudal septal deviation during February 2015 to August 2017 were analyzed; 23 patients underwent ES and the others (n = 23) underwent ESR. The decision of whether to use the ES or ESR was randomized by random number table method. Nasal obstruction symptoms evaluation (NOSE) scores, total nasal resistance (TNR), aesthetic visual analog scale (VAS), nasal anatomical angles, and incidence of complications were used to assess the patients in 2 groups.
Results:
The NOSE scores, TNR, aesthetic VAS, tip deviation angle (TDA), nasolabial angle (NLA), nasofrontal angle (NFA) in the ESR group were significantly improved from preoperative to postoperative 1 year, whereas in the ES group, except aesthetic VAS, NLA, NFA, all other postoperative outcomes were improved from preoperative values. The objective and subjective postoperative results of ESR group were better than the ES group except TDA. The incidence of complications was not significantly different between the 2 groups.
Conclusion:
Our study have compared the nasal functional and aesthetic outcomes of 2 septoplasty techniques in a randomized controlled trial. The ESR technique is more effective than ES technique in correcting functional and aesthetic disorders caused by anterocaudal septal deviation.
Keywords
Introduction
Nasal septal deviation is one of the most common diseases in otorhinolaryngology. This disease always lead to symptoms such as nasal obstruction, headache, and epistaxis. 1,2 Anterocaudal septal deviation is a kind of severe septal deviation that can result in congenital, traumatic, or iatrogenic insults. This type of septal deviation has unique structure and synostosis that make restore far more challenging. Anterocaudal septal deviation tends to nasal valves stenosis and aesthetic deformity of the nose. It also increases the risk of nasal tip support mechanism damaged when septoplasty was underwent. 3 Correction of this septal deviation has 2 major goals. 4 First, nasal stenosis and obstruction must be relieved and the nasal airway must be improved. Second, repair must be done to keep the nasal tip support stable. Traditional and extracorporeal septoplasty are procedures commonly performed to correct anterocaudal septal deviation. Traditional septoplasty was first put forward by Ingals in 1882 and modified by Killian in 1904. 5 Nowadays, traditional septoplasty is performed by endoscopic approach called endonasal septoplasty (ES). 6 Extracorporeal septal reconstruction (ESR) was first put forward by King 7 in 1952 and notably by Gubisch. 8 The principle of ESR is to replant the nasal septum after removing it completely or mostly. It is an ideal method to correct specific severe nasal septum deviation. 9 To further investigate the aesthetic and functional outcomes of septoplasty involving ES and ESR, we compared the 2 surgical methods as follows .
Materials and Methods
The study was approved by the local ethics committee to the Qingdao Municipal Hospital Affiliated and was performed according to the World Medical Association Declaration of Helsinki. In all, 46 patients (ES in 23 patients and ESR in 23 patients) who underwent nasal septoplasty surgery due to anterocaudal septal deviation in otorhinolaryngology department of Qingdao Municipal Hospital between February 2015 and August 2017 were analyzed. They were randomized into 2 groups: ES and ESR. Random processing was carried out by random number table method. After random assignment, all patients received corresponding surgical treatment. All procedures in this study were abide by the standards of the institutional and national ethics committee and all the participants have obtained the written informed consent.
Inclusion Criteria
Patients were conformed to the diagnostic criteria of anterocaudal septal deviation. Conservative treatment was ineffective and the patients had indications of nasal septum deviation. Patients developed symptoms such as nasal obstruction, headache, and so on. Patients who gave consent for the study participation.
Exclusion Criteria
Patients with mild anterocaudal septal deviation. Patients with active nasal disease, chronic rhinosinusitis, allergic rhinitis. Patients with other underlying diseases cannot tolerate the surgery. Patients unable to cooperate with follow-up.
Surgical Techniques
Patient’s consent was obtained prior to undertake the surgical procedure. All operations were performed by the same senior surgeon. All the patients were primary cases.
In the ES technique, after general anesthesia was induced, epinephrine with 1% lidocaine was injected into the nasal septum mucosa. The deviation septum was exposed by using nasal speculum. The mucosa from the caudal septum to the level of the cartilage was incised by making a Killian or hemitransfixion incision. Then the surgeon scraped the caudal quadrangular cartilage (QC) and elevated a mucoperichondrial flap. After the incision line was marked, the QC was incised parallel to the dorsum from the keystone. A through-biting instrument was used to incise the bony septum. The septal cartilage and bone were removed by using Takahashi or bayonet forceps. The remaining bony spurs were removed carefully to avoid damaging the skull base or keystone support. The length of the L-strut was preserved at least 1.5 cm. Finally, the mucoperichondrial flaps were reset and the mucosal incision was closed. Figure 1 shows the ES technique procedure.
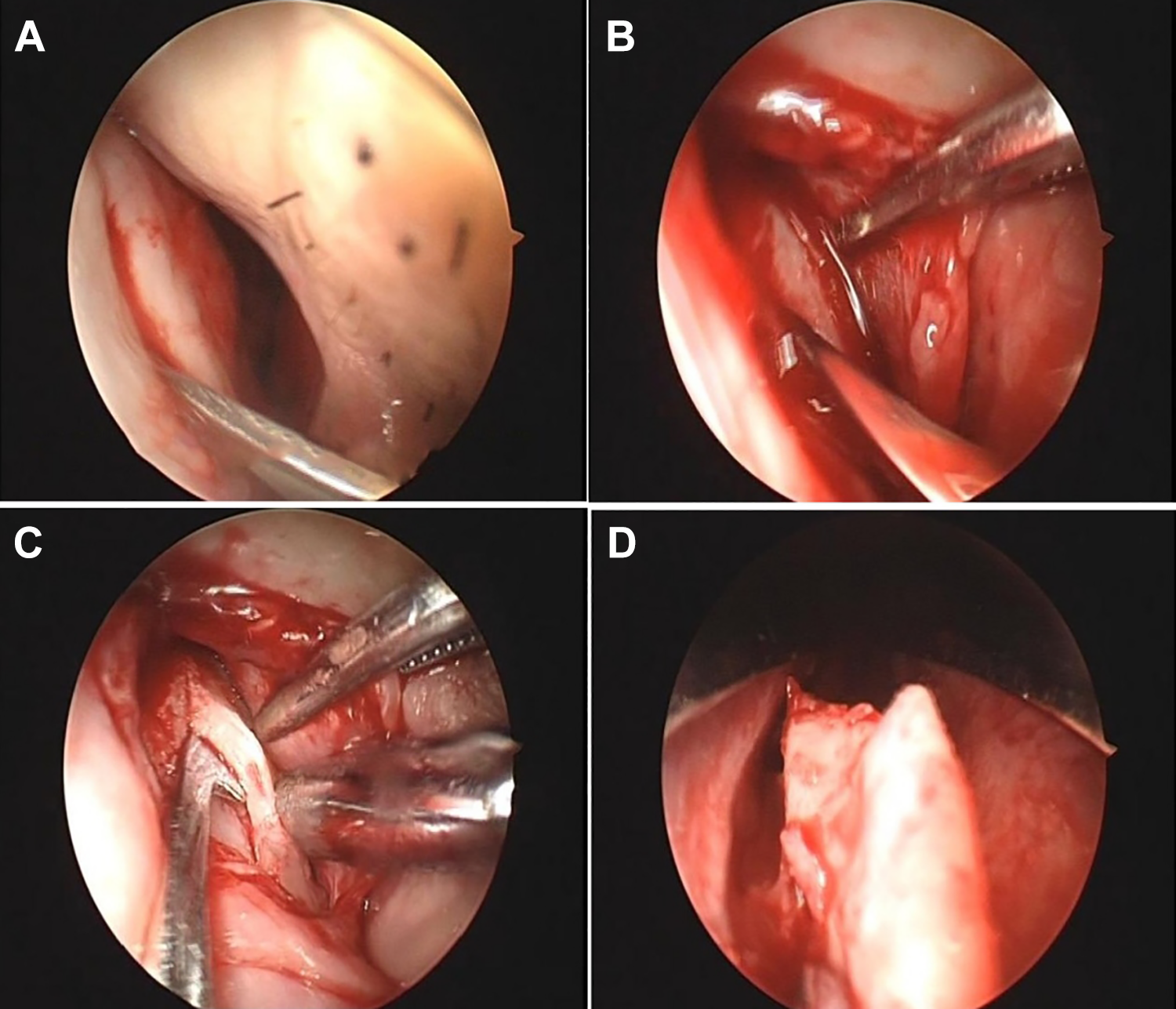
A, The mucosa from the caudal septum to the level of the cartilage is incised. B, The surgeon scraps the caudal quadrangular cartilage (QC) and elevates a mucoperichondrial flap. C, Transition around the posterior septal angle is performed and the same plane dissected on the opposite side. D, The incised septal cartilage and bone are removed.
In the ESR technique, patients were kept supine and received general anesthesia. An inverted “V” incision was incised at the 1/3 (middle and lower) of the columella. The incision was extend to the middle columellar area following the caudal edge of the lateral crus posteriorly moved up. The skin flap of nasal columella was separated and turned up to expose the dorsolateral cartilage, the superior lateral cartilage, and the nasal bone. Part of the deviant septal bones and cartilage flaps were removed to form a new “L” support. Then, the newly formed septal cartilage was sutured to the keystone and the tissue that around the anterior nasal spine with 4-0 polydioxanone (PDS) sutures to keep the caudal septum stable. After the new L-strut was shaped, the dorsal of the septal cartilage was sutured to the upper lateral cartilages with 4-0 PDS to provide additional stability. Then, the surgeon reconstructed the nasal tip and sutured the incision of nasal columella with 6-0 nonabsorbable sutures. Finally, the nose was placed with a thermoplastic splint and filled with vaseline yarn. Figure 2 shows the ESR technique procedure.
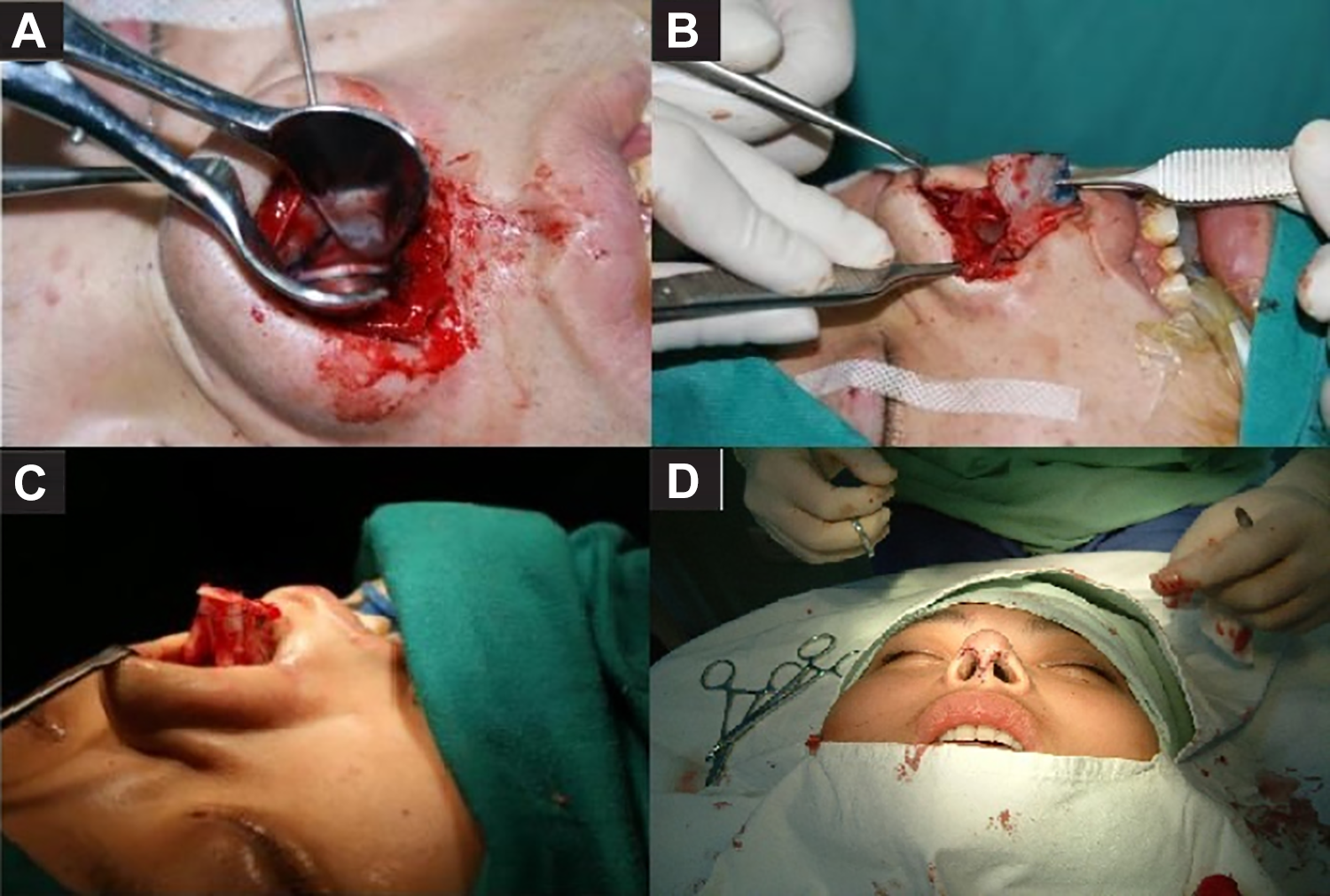
A, The skin flap of nasal columella is separated and turned up to expose the nasal septal cartilage B, Septal bones and cartilages are removed to form a new “L” support. C, The newly formed septal cartilage is sutured to the tissue that around the anterior nasal spine. D, The incision of nasal columella is sutured with 6-0 nonabsorbable sutures.
Outcome Data
The nasal obstruction symptoms evaluation (NOSE) Scale 10 was used to evaluate the subjective nasal obstruction symptoms in the preoperative and postoperative 1 year. The NOSE Scale included 5 items, 0 to 4 points were used for each item to indicate the severity. The scores were summed for an ultimate score. Higher scores meant serious nasal obstruction. According to the NOSE Scale results, the patients were categorized as mild (1-5), moderate (6-10), severe (11-15), or extreme (16-20).
Active anterior rhinomanometry (AAR) was an objective method to measure the nasal obstruction in the preoperative and postoperative 1 year. According to the standard guidance of AAR, 11 the average values of the total nasal resistance (TNR) were measured byrhinomanometer (NR6, GM Instruments Ltd., Scotland, United Kingdom) with a standard pressure of 150 Pa. All the patients remained seated. The oxymetazoline nasal drops was used to decongest the nasal mucosa and then the rhinomanometer was fixed to the patient’s face. The TNR value was obtained as the evaluation data.
A visual analog scale (VAS) was used for the subjective aesthetic analysis in the preoperative and postoperative 1 year by asking the patients how much they liked the appearance of their nose. Aesthetic analysis is a comprehensive analysis of the nasal dorsum, nasal tip, nasal nostril, nasal columella, alar, and alar base.
Three important nasal anatomical angles measured from the standard frontal and lateral photographs of the patients were used to assess objective nasal aesthetics in the preoperative and postoperative 1 year. The photographs were taken by a digital SLR camera (Nikon D3500, Nikon, Japan). Patients stood 1.5 m away from the camera to take the frontal and lateral view photographs. Angles measurement was taken by using a ruler and a protractor. Tip deviation angle (TDA) was measured from the frontal photographs. This angle was consisted of nasion–labral lines and nasion–tip lines. Lateral photographs were used to measure the nasolabial angles (NLAs) and nasofrontal angles (NFAs).
Postoperative complications included persistent nasal obstruction, septal perforation, septal abscess, septal hematoma, saddling deformity, nasal hemorrhage, infection, asymmetric nostrils, and so on. The incidence of postoperative complications was used to compare the risk of surgery techniques.
Statistical Analysis
Statistical analyses were done using computer software (SPSS version 22.0, SPSS Inc, Chicago, Illinois). The preoperative and postoperative NOSE scores, TNR, aesthetic VAS, TDA, NLA, and NFA in both ES and ESR groups were obtained and compared by using a Wilcoxon signed-rank test. This test was also used to determine whether the changes in these outcomes were significantly different between ES and ESR patients. The incidence of postoperative complications was expressed by percentage. A chi-square test was used to determine whether the changes in incidence of postoperative complications were significantly different between ES and ESR patients. Differences were regarded statistically significant when the P value was <.05.
Results
The mean ages of the ES and ESR groups were 34.5 years (range 21-43 years) and 36.5 years (range 23-42 years), respectively. There were 16 males and 7 females in the ES group. The ESR group included 18 males and 5 females. History of nasal trauma was present in 14 (60.9%) patients in the ES group and 12 (52.2%) patients in the ESR group. Nasal surgery history was present in 4 (17.4%) patients in the ES group and 6 (26.1%) patients in the ESR group. The follow-up of these patients was 12 to 24 months. The mean follow-up period was 17 months in the ES group and 19 months in the ESR group. There was no significant difference in gender, age, nasal trauma, nasal surgery, and follow-up period between the 2 groups (Table 1).
Characteristics of the Patients.a
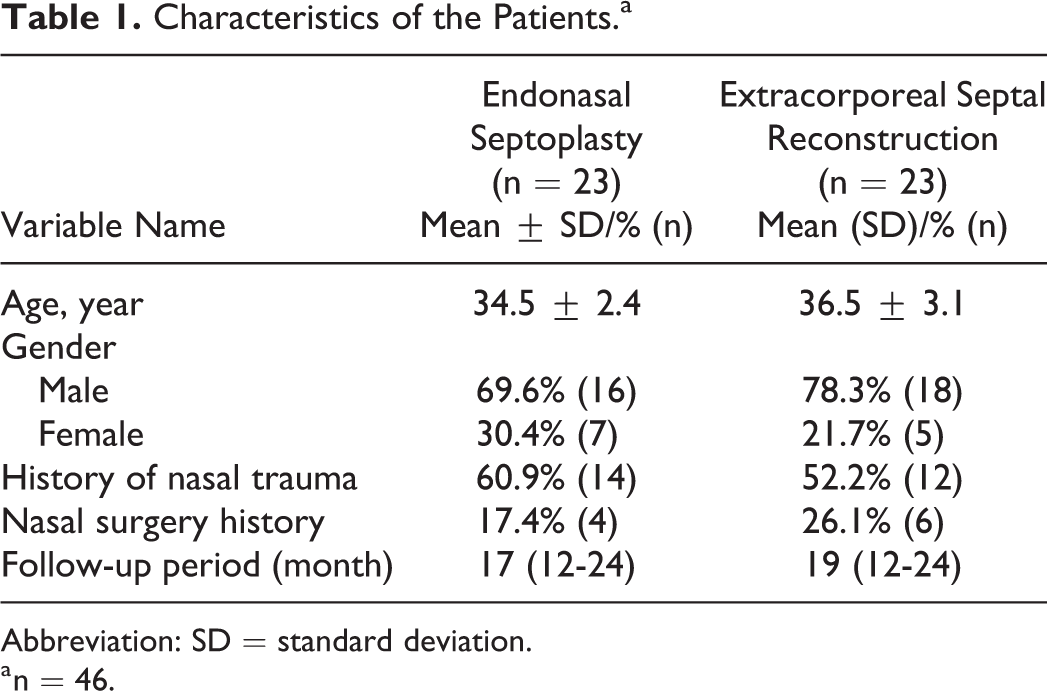
Abbreviation: SD = standard deviation.
a n = 46.
According to the preoperative NOSE scores, there were 12 patients with severe degree nasal obstruction and 11 patients with extreme degree nasal obstruction in the ESR group. Fifteen patients with severe degree nasal obstruction and 8 patients with extreme degree nasal obstruction were in the ES group. There were no significant differences in preoperative NOSE scores between the ES group and ESR group (Z = −0.444, P = .657). The NOSE scores in the ES group were decreased from preoperative (14.69 ± 2.49) to postoperative 1 year (8.22 ± 1.73; Z = 5.644, P < .001). There was also a significant decrease in NOSE scores from preoperative (15.04 ± 2.74) to postoperative 1 year (6.61 ± 1.44) in the ESR group (Z = 5.832, P < .001). The postoperative 1-year NOSE scores in the ESR group had a greater decrease compared to the ES group (Z = 2.988, P = .003). There were 5 patients with mild degree nasal obstruction and 18 patients with moderate degree nasal obstruction in the ESR group after surgery. In the ES group, 20 patients had moderate degree nasal obstruction and 3 patients still had severe degree nasal obstruction after surgery (Table 2).
Comparison of the NOSE Scores Obtained From Preoperative and Postoperative 1-Year Measurements Between the ES and ESR Groups.
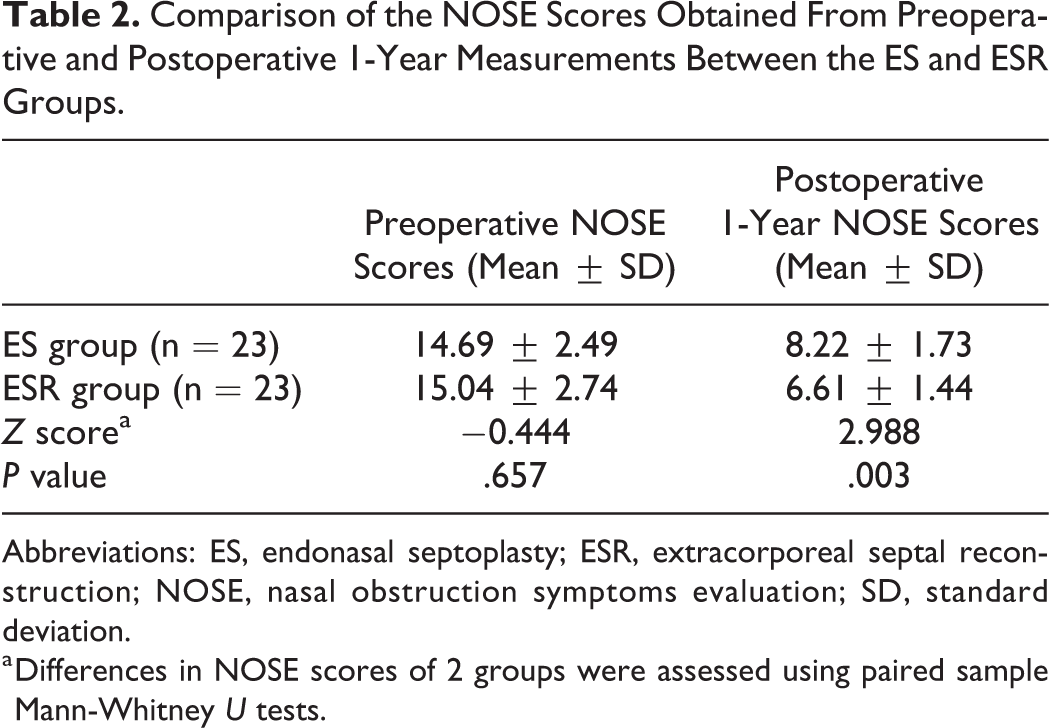
Abbreviations: ES, endonasal septoplasty; ESR, extracorporeal septal reconstruction; NOSE, nasal obstruction symptoms evaluation; SD, standard deviation.
a Differences in NOSE scores of 2 groups were assessed using paired sample Mann-Whitney U tests.
There was no significant difference in preoperative TNR between the ES group and ESR group (Z = −0.683, P = .495). Total nasal resistance in 2 groups were decreased from preoperative to postoperative 1 year (both P values were less than .05). The postoperative 1-year TNR in the ESR group had a greater decrease compared to the ES group (Z = 2.357, P = .018; Table 3).
Comparison of the TNR Obtained From Preoperative and Postoperative 1-Year AAR Measurements Between the ES and ESR Groups.
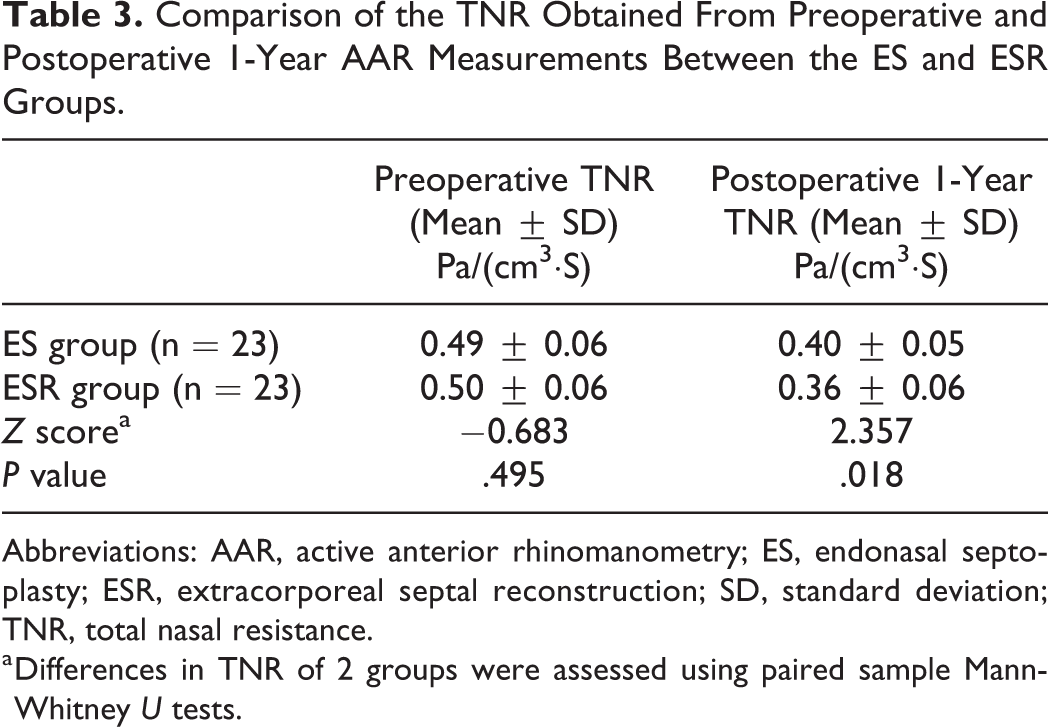
Abbreviations: AAR, active anterior rhinomanometry; ES, endonasal septoplasty; ESR, extracorporeal septal reconstruction; SD, standard deviation; TNR, total nasal resistance.
a Differences in TNR of 2 groups were assessed using paired sample Mann-Whitney U tests.
There was no significant difference in preoperative VAS values of aesthetic outcomes between the ES group and ESR group (Z = 0.676, P = .499). The postoperative VAS values(6.91 ± 0.73)of aesthetic outcomes in the ESR group were increased compared to the preoperative values(3.65 ± 1.11; Z = −5.752, P < .001). In ES group, there was no significant difference in VAS values of aesthetic outcomes between preoperative (3.82 ± 1.03) and postoperative (4 ± 0.95; Z = −.450, P = .653). Improvement of the aesthetic outcomes was higher in the ESR group (Z = −5.760, P < .001; Table 4).
Comparison of the Aesthetic VAS Obtained From Preoperative and Postoperative 1-Year Measurements Between the ES and ESR Groups.
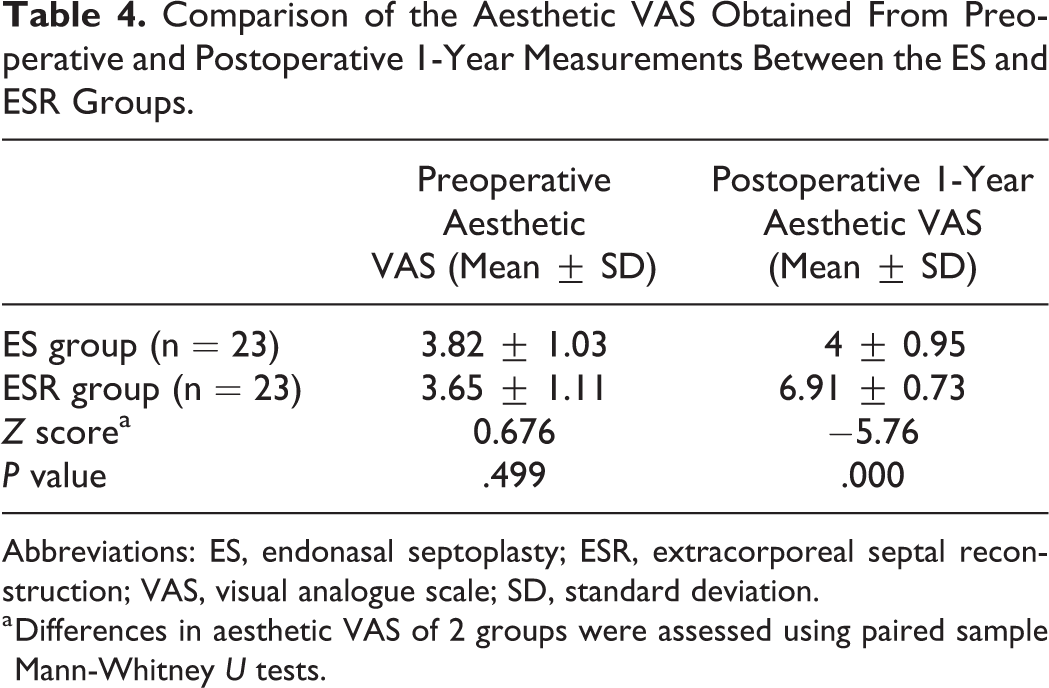
Abbreviations: ES, endonasal septoplasty; ESR, extracorporeal septal reconstruction; VAS, visual analogue scale; SD, standard deviation.
a Differences in aesthetic VAS of 2 groups were assessed using paired sample Mann-Whitney U tests.
The postoperative 1-year TDA (1.35 ± 0.48), NLA (90.53 ± 4.61), and NFA (128.84 ± 5.83) in the ESR group changed significantly compared to the preoperative (2.92 ± 1.09; 85.2 ± 5.24; 139.25 ± 3.99; both P values were less than .05), whereas in the ES group, only postoperative 1-year TDA (1.48 ± 0.8) was significantly different from preoperative (3.15 ± 1.27; Z = 4.882, P < .001). The postoperative 1-year NLA (82.6 ± 5.84) and NFA (140.17 ± 4.61) in the ES group had no obvious changes compared to the preoperative (83.59 ± 5.72; 138.84 ± 4.54; both P values were large than .05). There was no difference between the 2 groups in the preoperative values of these 3 angles (TDA P = .597; NLA P = .368; NFA P = .725). The postoperative 1-year NLA and NFA were different between the 2 groups, but there was no difference in DTA (P = .741; Table 5).
Comparison of the Nasal Anatomical Angles Obtained From Preoperative and Postoperative 1-Year Photograph Measurements Between the ES and ESR Groups.
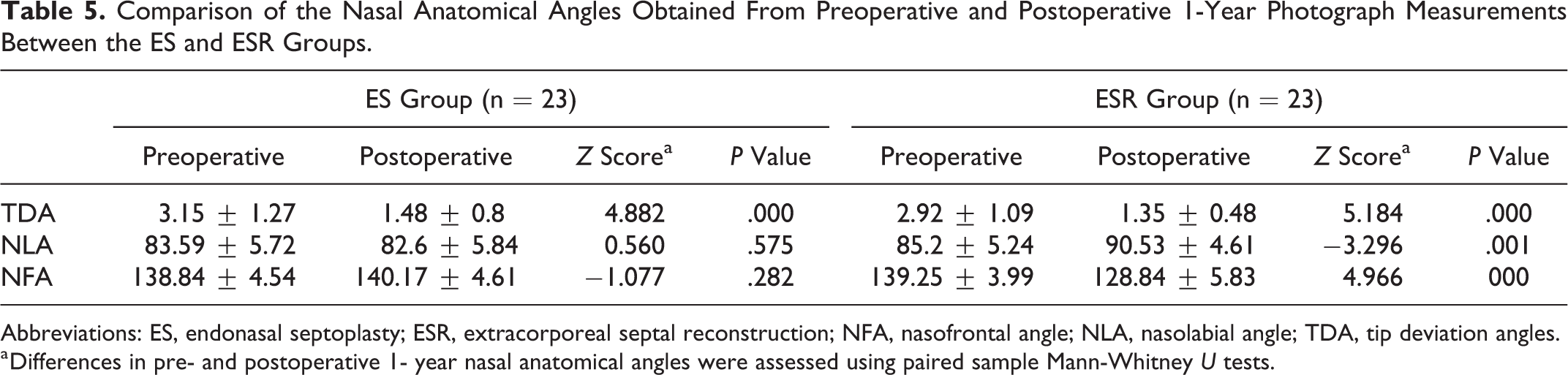
Abbreviations: ES, endonasal septoplasty; ESR, extracorporeal septal reconstruction; NFA, nasofrontal angle; NLA, nasolabial angle; TDA, tip deviation angles.
a Differences in pre- and postoperative 1- year nasal anatomical angles were assessed using paired sample Mann-Whitney U tests.
The incidence of complications was not significantly different between the 2 groups (c2 = 0.224, P = .636). There were 2 patients with nasal hemorrhage in the ESR group and 1 patient in the ES group; 1 patient in the ES group had postoperative septal perforation and 1 patient had septal hematoma after the ESR operation. No postoperative infection, septal abscess, asymmetric nostrils, saddling deformity was detected in 2 groups. No patient had persistent postoperative nasal obstruction that required revision operation (Table 6).
Comparison of Postoperative Complications Between the ES and ESR Groups.
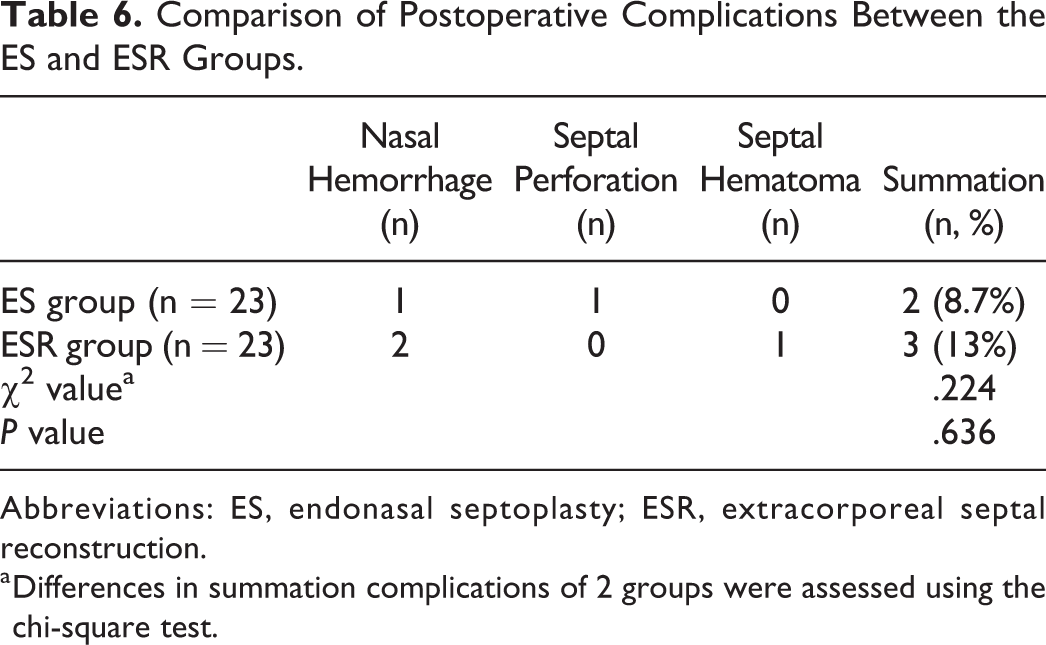
Abbreviations: ES, endonasal septoplasty; ESR, extracorporeal septal reconstruction.
a Differences in summation complications of 2 groups were assessed using the chi-square test.
Discussion
Anterocaudal septal deviation is one of the most common reasons that lead to nasal aesthetic or functional disorders. The nasal valve, nasal patency, major tip support mechanisms, and nasal aesthetic landmarks can be adversely affected by the anterocaudal septal anatomic abnormalities. 1,3 The corrections of anterocaudal septal deviation are difficult and complicated to perform. It demands proficient surgical skills to be successful. Several operations have been considered useful to correct anterocaudal septal deviation such as swinging door technique, translocation technique, spreader or batten grafts, stabilization of tongue-in-groove, septal cartilage morselization, ES, and ESR. 12,13 Endonasal septoplasty technique is a common method to correct the nasal septal deviation by removing part of the nasal septal cartilage and perpendicular plate of the ethmoid bone. Although ES technique has been confirmed to have some benefits in the patients who have anterocaudal septal deviation, 14 it is not enough to correct severe caudal septal deviation and nasal cavity stenosis with those repositioning and suturing methods. If the septum is radical dysmorphia, even the caudal aspect is reset to the midline will not enough to treat the nasal obstruction. As removal of the septal cartilage without rebuild the septal strut will result in instability of nasal tip support. Using ES technique in the anterocaudal area can be risky.
With the development of nasal endoscopic surgery, otolaryngologists have gradually improved their surgical knowledge to find an operative method that can correct the deviation of nasal septum and avoid the collapse of the nasal dorsum as much as possible. Now the most commonly used method is ESR. Extracorporeal septal reconstruction is a modified septoplasty that correct the severe nasal septum deviation by an external approach. 15 In ESR technique, the cartilages of nasal septum are completely removed and replaced by a reproductive and straighter septum.
It can be more effective in treating nasal obstruction and external nose deformity in patients of severe anterocaudal septal deviation. 16 In ESR technique, narrow internal nasal valve angle is corrected by rectifying the severe anterocaudal septal deviation while also placing the spreader grafts to further improve the nasal valve patency. 17 It is quite remarkable that the ESR technique avoids the cartilage memory (the elastic cartilage tends to return to the original position) from winding. 18 There are many current studies that demonstrate the ESR outcomes in long-term success with decrease from severe preoperative to lighter postoperative symptoms. About the influence of ESR technique on the nasal obstruction, Marangi et al 19 compared the NOSE scores and acoustic rhinomanometry after ES technique and ESR technique with 50 patients. The authors reported that rhinomanometric scores in the ES group were higher than in the ESR group at 3 months postoperatively and this difference disappeared at 6 months postoperatively. This study demonstrated that ESR could significantly improve postoperative nasal patency. About the evaluation of the aesthetic outcomes in ESR technique, Baser et al 20 described the postoperative aesthetic outcomes in ESR technique with 35 patients. This study reported that 32 (91.43%) patients showed significant improvement of aesthetic satisfaction and only 3 (8.5%) patients showed there is no improvement. Extracorporeal septal reconstruction technique can also improve other nasal functions. Patients with septal deviation are frequently accompanied with hyposmia due to obstruction of nasal air flow. Türk et al 21 described that ESR could improve olfactory threshold, discrimination, and identification function in patients with severe nasal septal deviation. The patients with anosmia or hyposmia had significant improvement after operation. Extracorporeal septal reconstruction technique is beneficial to olfactory recovery and this effect may owing to increased sense of nasal airflow and anatomic improvement of the internal nasal valve operative area. However, septoplasty may cause the olfactory function damage due to injury in the epithelium of the olfactory region. Recent studies have reformed traditional ESR technique to improve the operative efficiency and reduce the incidence of complications. Jang et al 22 reported that PDS foil can be used for ESR technique to support or stabilize the reconstructed septal cartilage. Rezaeian et al 23 have created the criss-cross and transcutaneous transosseous cerclage suture to reduce the incidence of complications after ESR technique. These modified suture methods could overcome the vital and technically demanding of the ESR technique. According to the outcomes of our study, anterocaudal septal deviation can be corrected effectively by either ES or ESR. The NOSE scores and TNR of the patients in our study were improved after ES or ESR. The improvements of these 2 outcomes in the ESR group were better than the ESR group. Therefore, both objective and subjective examination results show that ESR is more beneficial to improve nasal obstruction. Moreover, the postoperative 1-year TNR in ESR group had a greater decrease compared to ES group. The nasal aesthetic was evaluated by VAS and nasal anatomical angles. Extracorporeal septal reconstruction technique could improve the aesthetic VAS, TDA, NLA, and NFA value. But ES technique could only promote the TDA of the patients. It means ES technique could correct the external nasal deviation but could not improve the collapse of nasal tip. In our study, there were no patients complained about a worse nasal obstruction or severe decline of the nasal aesthetic satisfaction after the surgery in either group. Extracorporeal septal reconstruction seems to be more advantageous in the treatment of severe anterocaudal septal deviation compared to ES. The improvement of nasal obstruction and nasal aesthetic in ESR was better than ES. This difference may be due to implantation of the reconstructed nasal septum which can enlarge the nasal valves region and improve the shape of nasal dorsum, nasal tip, nasal nostril, and nasal columella. Because of the limitation of ES technique, the outcomes of the nasal obstruction were significantly less improved and it was not effective in improving the nasal aesthetic satisfaction. About the surgical complications, Dąbrowska-Bień et al 24 conducted a study about the complications of nasal septoplasty in a large group of 5639 patients. There were 193 patients with different types of complications (3.42%) in the whole study. Nasal hemorrhage was the most frequent complication (3.3%). Other postoperative complications included hyposmia (>1 week <6months; 3.1%), infection (prolonged healing; 3.1%), septal perforation (2.3%), adhesions (0.8%), tooth/upper lip anesthesia (0.1%), and ocular complications (0.08%). In our study, nasal hemorrhage was observed in 3 patients (2 patients was in the ESR group and 1 patient was in the ES group). One patient in the ES group had postoperative septal perforation. And 1 patient had septal hematoma after the ESR operation. No patient required revision operation to treat the complications. The above results of this study were in concordance with most previous researches, but this is the first time to research the surgical methods for severe anterocaudal septal deviation. We can conclude that ESR should be chosen over the ES technique in patients with anterocaudal septal deviation.
Limitations
This study has some limitations. First, fewer cases is the shortcoming of this study. We tried to overcome this limitation by performing standard surgical techniques. Moreover, lacking of acoustic rhinometry is another limitation of this study. Finally, 3 patients had nasal hemorrhage, 1 patient had septal perforation, and 1 patient had septal hematoma. After treatment, these patients recovered from postoperative complications.
Conclusion
This comprehensive study compared the aspects of the patients who underwent 2 common different surgical techniques for treatment of anterocaudal septal deviation. Extracorporeal septal reconstruction technique is more effective than ES technique in correcting functional and aesthetic disorders caused by anterocaudal septal deviation. Moreover, the most important thing is that surgeons should acquire more knowledge about septoplasty surgical technique to provide the best possible outcome by reestablishing the structure, function, and external form of the nose.
Footnotes
Acknowledgments
The authors wish to thank Wen-ting Hu for her support in collecting data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Qingdao Medical talents training project [Grant Number VDTR2017Y15].