
Abstract
Background:
Laryngeal carcinoma is one of the most common malignant tumors of the head and neck. Researchers have refined the study of surgical margin in the anatomical subarea of the larynx to determine the most appropriate distance of the surgical margin for laryngeal carcinoma, to achieve accurate resection of laryngeal carcinoma and to improve the possibility of retention of laryngeal function.
Methods:
A comprehensive review of the primary literature was performed from 2009 to 2019 utilizing keywords laryngeal carcinoma, surgical margin, molecular margin, and prognostic factor. Articles were included at the discretion of the authors based on novel and/or contributions to the literature.
Results:
The prognosis of laryngeal carcinoma significantly correlates with the status of surgical margins. Patients with positive surgical margins have higher recurrence and metastasis rates and worse prognosis. Patients with negative pathological surgical margin but with the expression or altered expression levels of one or more tumor-related molecular biomarkers had high rates of recurrence and metastasis, and poor prognosis.
Conclusions:
Clinical intervention can improve the prognosis of patients with positive surgical margins. Patients with close margins should be followed closely. Among patients with negative surgical margins, patients with abnormal molecular margin results should be closely followed up. However, the specific selection of one or several molecular biomarkers as the detection index of molecular margin currently requires multicenter prospective or retrospective large sample study as guidance.
Introduction
Laryngeal carcinoma is one of the most common malignant tumors of the head and neck. The surgical treatment of laryngeal cancer has 2 purposes, one is to completely remove the tumor, and the other is to preserve the function of the throat as much as possible. Therefore, the scope of primary tumor resection is particularly important, and the surgical margins of laryngeal cancer are highly valued by clinicians. The prognosis of laryngeal carcinoma is significantly correlated with the condition of surgical margins. 1 -3 There are many classifications and confusing definitions of laryngeal carcinoma surgical resection margins.
Histopathological diagnosis is currently used to determine whether the surgical margins are safe. It has been reported that in patients with head and neck squamous cell carcinoma (HNSCC), the postoperative local recurrence rates of histologically negative surgical margins are 9% to 32%. It suggests that a histologically negative margin is not a truly safe surgical margin. 4 Studies have shown that changes in molecular levels and biochemical metabolism occur before changes in cell morphology. 5 Many researchers have tested expression of molecular biomarkers in laryngeal carcinoma and surgical margin tissues, compared the correlation between expression and prognosis, and explored the feasibility of molecular and surgical margins in guiding clinical treatment jointly.
Surgical Margins of Laryngeal Carcinoma
Negative and Positive Margins
At present, most clinicians use the result of histopathological diagnosis as the basis for judging whether the surgical margin is clean. The surgical resected tissue is continuously sliced at a thickness of 4 μm, according to whether there are residual cancer cells with the aim of determining its safety in the section. Sections with tumor cells in the margins are defined as positive surgical margins; if no tumor cells are seen in the surgical margin, this is a safe margin. 6 Early research suggested that traditional safe margins of more than 10 mm were recommended, and 10 mm and above were also referred to as ideal margins. Because of the patient’s strong desire to retain the function of the larynx and the required quality of life, surgeons strive to retain the function of the larynx to the greatest extent possible while achieving radical excision. The guideline of the National Comprehensive Cancer Network (NCCN) for Head and Neck Tumors (2019) defines clear margin as 5 mm or more from the infiltrating leading edge of the tumor, and 1 to 2 mm surgical margin zone was considered to be sufficient for glottic cancer. The presence of carcinoma in situ or infiltrating carcinoma on the surgical margin is defined as positive margin. Based on the relationship between the margin status and clinical prognosis, some scholars have proposed different criteria that considered the margin of the poor prognosis as a positive margin. They thought it included tumor tissue less than 5 mm from the surgical resection margin (the so-called close margin), margins with atypical hyperplasia epithelium, margins with carcinoma in situ, and margins with invasive carcinoma. 7
Close Margin
Close margins are the gray area between the pathological positive and negative margins. The NCCN guideline defines close margin of HNSCC as less than 5 mm from the infiltrating leading edge of the tumor. Alicandri-Ciufelli et al suggested that close margin of vocal cords should be no more than 1 mm, the close margin of the larynx should be no more than 5 mm in HNSCC. 8 These criteria may be the lower limit of surgical margin. Depending on the general situation of the patient, the stage of tumor and laryngeal function, the follow-up treatment could be appropriately expanded the scope of resection.
Safe Margin in Various T Stages
The growth of laryngeal squamous cell carcinoma is 3-dimensional, with both mucosal invasion and submucosal expansion. 9 The later the T stage of primary laryngeal carcinoma, the higher the degree of submucosal infiltration. 10 Existing research showed that there was a significant difference in the submucosal infiltration distances of the larynx between T1-2 and T3-4. For T1-2 stage laryngeal cancer, 5 mm can be used as the safe resection distance of the primary tumor. However, for the stage T3-4 laryngeal cancer, partial laryngectomy with the mucous membrane of the 5 mm margin, may result in submucosal tumor residual. And it should require approximately 10 mm distance of the mucous membrane as the safe margin. 11
Safe Margin After Induction Chemotherapy
Induction chemotherapy is aiming to minimize the scope of the primary tumor, to reduce the scope of surgical resection or radiotherapy, to eliminate or reduce microscopic cancers, and to prevent postoperative recurrence and dissemination. 12 After 3 cycles of TPF (taxol, cisplatin, fluorouracil) induction chemotherapy in the treatment group, Wang et al found that induction chemotherapy reduced the clinical stage of patients and reselected surgical procedures to increase the rate of laryngeal preservation after downstaging. 13 Lu et al adopted the DCF (docetaxel, cisplatin, fluorouracil) chemotherapy regimen to treat laryngeal cancer and hypopharyngeal cancer of T2-3 stages. After 3 cycles of induction chemotherapy, the results showed that preoperative induction chemotherapy shrank the tumors in some patients and reduced the scope of laryngectomy. After induction chemotherapy, resection of the tumor along the 5 mm range around the narrowed laryngeal cancer lesion can ensure that the surgical margin is safe, and did not increase the positive rate of surgical margins. 14
Relationship Between Surgical Margin and Prognosis of Laryngeal Carcinoma
Studies have shown that surgical margin is an independent risk factor affecting the prognosis of laryngeal carcinoma. According to the range of the resection edge, it can be divided into no more than 3 mm, 4 to 5 mm, and no less than 5 mm to compare the local recurrence rate and metastasis rate in these 3 sections. The 3-year and 5-year disease-free survival were compared according to the presence or absence of local recurrence or metastasis. The results showed that the smaller the surgical margin, the higher the postoperative local recurrence rate. Both the local recurrence rate and lymph node metastasis rate of patients with positive surgical margins were higher than those with negative surgical margins, and the prognosis was worse than those with negative surgical margins. 15 Studies of Sessions et al have shown that the survival rate and recurrence rate had nothing to do with total laryngectomy, laryngeal function preservation surgery, and whether surgery was combined with radiotherapy. But it was related to the status of surgical margin. Survival rates in the close margin group (less than 5 mm) were significantly lower than safe margin group. 16 Other researchers have drawn the same conclusion, that close margins mean lower survival rates and higher recurrence rates, and worse prognosis. 17,18
Due to the different anatomical structure characteristics of different primary tumor sites, such as lymphatic drainage, angiogenesis, or different natural barriers (cartilage, bone, etc), tumors have different invasion and metastasis capabilities to different sites. The positive rate of surgical margin in different directions and distances is also different. At present, the safety resection scope of primary tumor is still controversial. It may not be suitable to define the safe surgical margin of tumors in different parts with a single standard. Figure 1 summarizes the definition of surgical margins in different cases of laryngeal carcinoma.
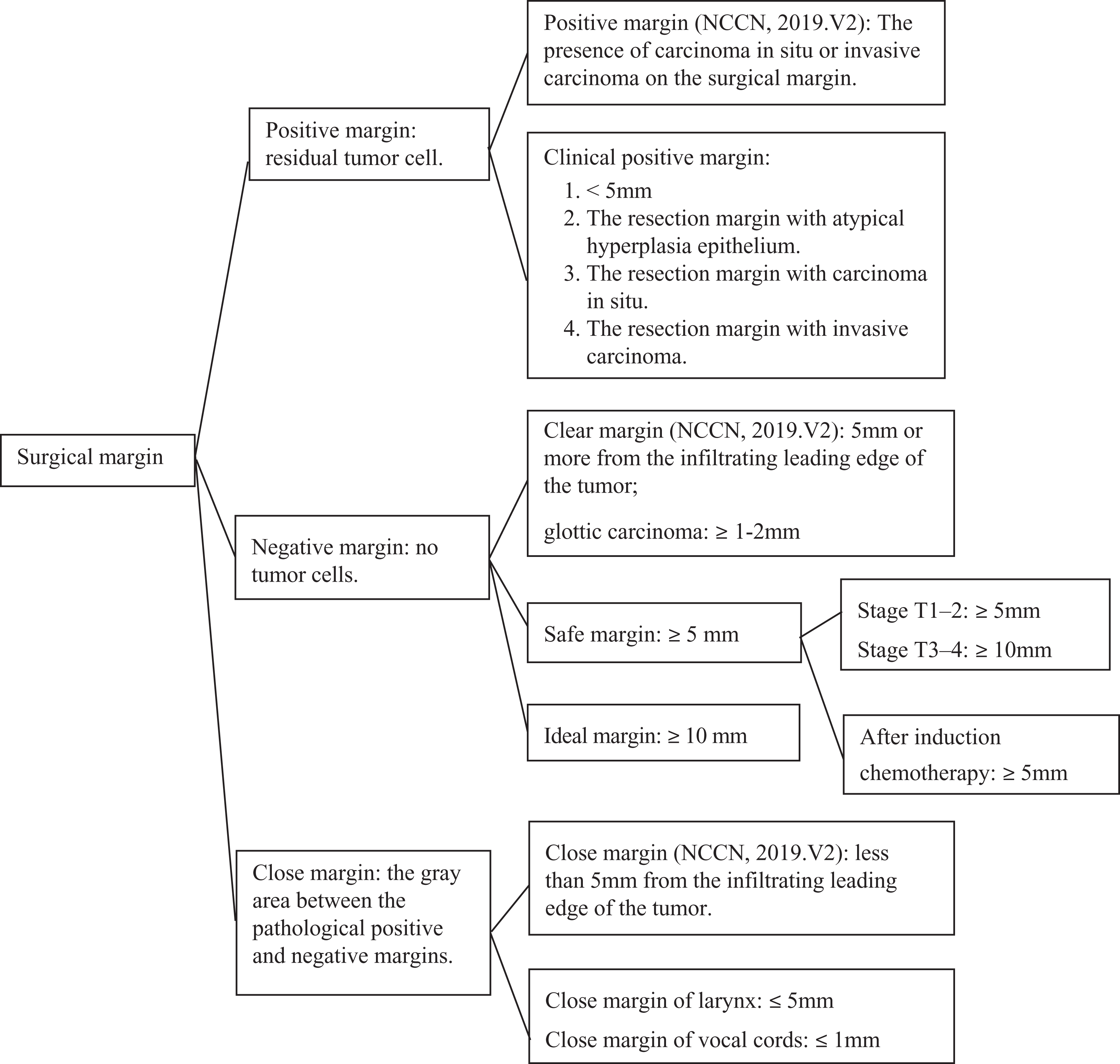
The definition of surgical margins in different cases of laryngeal carcinoma.
Therefore, appropriate tangents are selected according to the different primary sites, stages, and ranges of laryngeal carcinoma, to effectively reduce the occurrence of positive surgical margins and to achieve better prognosis. Tian and Wang proposed that even if there is an ideal safe margin, the surgeon could not completely remove the tumor according to this distance in practice. Especially when the deep infiltration boundary of tumor cannot be seen, at this time the operator is basically in the state of feeling to remove the tumor, so that the gap of 1 to 2 mm is insignificant when discussing the safe margin. 19 This researcher went on to point out that real-time marker display of intraoperative is a prerequisite for accurate resection of tumors. Fluorescence-guided surgery system is moving from animal experiments to clinical practice. This system can show the range of tumor in real-time during surgery, 20,21 providing real-time guidance for complete resection of tumor and acquisition of negative surgical margins, bringing new hope for accurate resection and functional retention of laryngeal carcinoma.
Molecular Margins of Laryngeal Carcinoma
Definition of Molecular Margins
Boudewijn et al 5 showed that there were 2 reasons for false negative results in pathological examination of the incisional margin. On the one hand, the existence of residual tumor cells, known as micrometastases, could not be detected by current pathological techniques, leading to local recurrence. On the other hand, there were precancerous lesion areas, and these precancerous cells had undergone molecular changes leading to local recurrence. 5 Brandwein 22 and Sidransky et al 23 proposed the concept of molecular margin based on the above content, and believed that molecular margins can predict tumor recurrence and prognosis more accurately.
Detection Method for Molecular Margin
At present, most researchers use the methods of immunohistochemical staining, reverse transcription-polymerase chain reaction (RT-PCR), and fluorescence in situ hybridization (FISH) to measure expression of molecular biomarkers at the protein and nucleic acids level in laryngeal cancer and surgical margins to discuss the qualitative situations of molecular margins. One of the most commonly used and economical detection methods is immunohistochemistry. Studies have shown that changes in molecular level occur prior to tumor cells undergo significant changes. 24
Relationship Between Common Molecular Biomarkers and Prognosis
With the in-depth study of tumor cell cycle and its regulatory mechanism, it is gradually recognized that tumors are diseases caused by multigene changes leading to disordered cell cycle and uncontrolled cell growth. 25
Tumor Suppressor Genes
When tumor suppressor genes such as P53, P27, and PTEN are mutated or deleted, they may play a key role in the initiation stages of local recurrence of laryngeal cancer.
The P53 protein encoded by the mutated tumor suppressor gene P53 has been widely studied. P53 mutations exists in 50% to 60% of patients with HNSCC. 26 If the P53 protein is detected in the surgical margin, it indicates that early tumor events have begun to appear in the cells. The local recurrence rate of patients with P53 protein expression at the surgical margin is higher than that of patients without expression. And the detection of P53 protein in the margin indicates the possibility of local recurrence after surgery. 27 Ozturk et al proposed that, in the surgical treatment of early glottic carcinoma, overexpression of P53 was more valuable for predicting recurrence and prognosis in the incisional margin tissue than in the primary tumor tissue. 28
P27 is a member of the cyclin-dependent kinase inhibitors family, which plays a negative regulatory role in the cell cycle, preventing the cell cycle from entering the S phase, thereby inhibiting cell proliferation. 29 After detecting the expression of P27 protein in laryngeal squamous cell carcinoma, researchers concluded that the inactivation of P27 in resection margin tissues was closely related to local recurrence of laryngeal cancer. 30
PTEN leads to cell cycle termination in G phase through a complex signal pathway, inhibiting cell malignant proliferation and tumor development, and inhibiting tumor angiogenesis and invasion. Yang et al combined detection of P27 and PTEN in the surgical margins of laryngeal cancer by CO2 laser resection. The result showed that the recurrence rate in patients with low expression of P27 and/or PTEN in the pathologically negative surgical margins was higher than that of the high expression group. 30,31 Other studies have also shown that the decrease or deletion of PTEN expression in the surgical margin of laryngeal cancer was closely related to postoperative local recurrence.
Oncogene
The oncogene c-myc is closely related to the occurrence, development, and outcome of many tumors. Studies have shown that the expression of c-myc protein in precancerous lesions and cancers is generally higher than that in normal tissues, and its expression in adjacent tissues is also higher than in normal. 32 However, Krecicki examined the expression of c-myc protein in laryngeal cancer and found that c-myc oncogene may be less important in laryngeal cancer than in other cancers. 33 The same conclusion was reached in another group of studies. The recurrence rate of the c-myc negative and positive groups of laryngeal cancer resection margins were not significantly different. And the expression of c-myc in the primary tumor of laryngeal cancer was also low. Therefore, c-myc should not be considered as a molecular indicator of the resection margin of laryngeal cancer. 34
Related to Cell Cycle
The excessive proliferation of tumors is closely related to the disorder of the regulatory factors of cancer cell cycle. 35 Eukaryotic initiation factor 4E (EIF4E) is a translation initiation factor for eukaryotic cells. When EIF4E is highly expressed, the key factors controlling the cell cycle increase disproportionately, and cells may undergo abnormal mitosis and/or apoptosis leading to genetic instability and carcinogenesis. 36 Franklin’s prospective study showed that patients with a loss of EIF4E expression in the negative surgical margin of laryngeal cancer have a better prognosis. 37 Eukaryotic initiation factor 4E was almost 95% expressed in HNSCC, and the rate of local recurrence is significantly higher in those who express EIF4E at the surgical margin than those who do not express EIF4E. This suggests that EIF4E can be used as a molecular biomarker to predict local recurrence of head and neck cancer, and has higher sensitivity than P53 protein. 38 Moreover, the elevated expression of EIF4E in the surgical margins of laryngeal cancer can be considered an independent risk indicator for predicting the prognosis of laryngeal cancer.
Proliferating cell nuclear antigen (PCNA) is an auxiliary factor of DNA polymerase delta. The content of PCNA changes with various stages of cell proliferation cycle, which is consistent with DNA synthesis, and can reflect the degree of cell proliferation. 39,40 The results of the present study showed that in patients with early-stage laryngeal cancer, who had a local recurrence during the 2-year follow-up period, the positive expression rates of PCNA in negative resection margin were significantly higher than those in the nonrelapsed patients. Highly expressed PCNA in the surgical margin was an important biological marker for the prognosis of patients with early laryngeal carcinoma. 41
Excessive expression of CyclinD1 can cause cells to lose their dependence on growth factors and continuously enter the cell cycle resulting in malignant proliferation and carcinogenesis. 42 In the resection margin of laryngeal cancer, the expression of CyclinD1 was different between the recurrent group and the nonrecurrent group. CyclinD1 was highly expressed in the recurrent group and the prognosis was poor. 43
Related to Apoptosis
Inhibiting apoptosis is also an important way to cause malignant proliferation of cells. Survivin blocks the apoptosis process and regulates the function of cell division leading to the unlimited proliferation of tumor cells. 44 The expression of survivin is highly positive in laryngeal cancer tissues, and it becomes less positive in the adjacent mucosa with further distance from the cancer focus. Patients with high expression of survivin in the resection margin have a poor prognosis. Survivin may serve as an independent prognostic predictor for laryngeal cancer. 45
B cell lymphoma 2 (Bcl-2) is an antagonistic gene for process of apoptosis or programmed cell death. 46 Overexpression of Bcl-2 protein is associated with poor differentiation of head and neck malignant tumors. 47 Giotakis et al measured expression of Bcl2 messenger RNA (mRNA) in laryngeal cancer tissue samples by RT-PCR, and found that high expression of Bcl2 mRNA was associated with poor prognosis. 48 Studies in laryngeal cancer have shown that the closer the incisional margin is to laryngeal cancer, the stronger is the expression of Bcl-2 protein. The positive expression of Bcl-2 protein in tissue 5 mm adjacent to the cancer was significantly different from that 10 mm adjacent to the cancer. This suggests that the surrounding tissues within 5 mm from the cancer focus are prone to carcinogenesis, and these tissues may be the source of postoperative recurrence of laryngeal cancer. 49 Table 1 illustrates the relationship between these commonly used molecular markers and the prognosis of laryngeal cancer.
The Relationship Between These Commonly Used Molecular Markers and the Prognosis of Laryngeal Cancer.
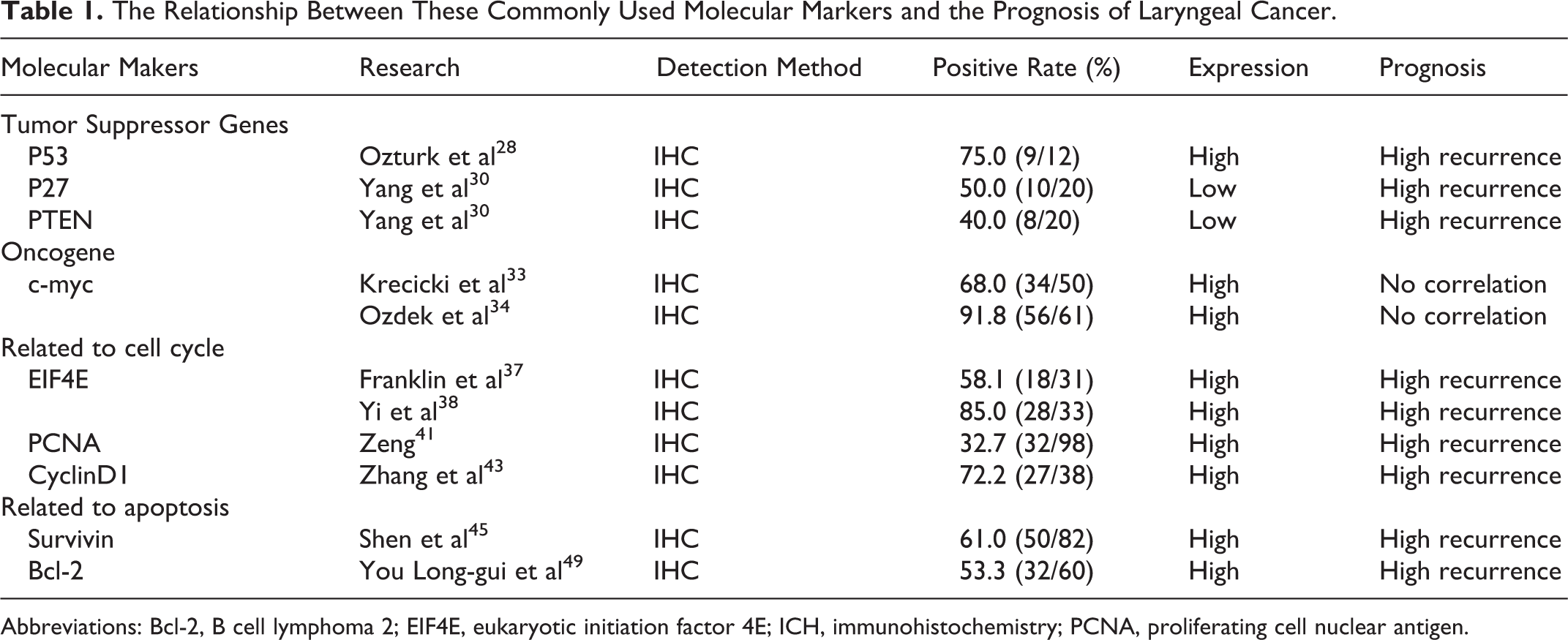
Abbreviations: Bcl-2, B cell lymphoma 2; EIF4E, eukaryotic initiation factor 4E; ICH, immunohistochemistry; PCNA, proliferating cell nuclear antigen.
Conclusion
The majority of studies have shown that patients with close margins or positive surgical margins of laryngeal cancer have higher recurrence rates, metastasis rates, and worse prognosis than those with negative margins. Clinically, patients with close margins can be followed closely. The prognosis of patients with positive surgical margin can be improved by postoperative adjuvant therapy. 50 For patients with high T stage, the distance of the safe surgical margin should be appropriately extended to ensure a better prognosis. For patients with effective induction chemotherapy, the conventional safe distance of the cutting edge can be selected, without the need to expand the distance.
However, patients with pathological negative surgical margin but with the expression or altered expression levels of one or more tumor-related molecular biomarkers had high rates of recurrence and metastasis, and poor prognosis. The abovementioned commonly used molecular biomarkers such as P53, PCNA, EIF4E, CyclinD1, survivin, and Bcl-2 are highly expressed in the negative surgical margin; P27 and PTEN are lowly expressed in the negative surgical margin. Various molecular biomarkers play different roles in occurrence and development of laryngeal cancer, and the positive expression rate of each molecular biomarker in the surgical margin is also different. Simultaneous positive expression of multiple molecular markers appears to be more accurate in predicting the prognosis of laryngeal cancer than that of single molecular biomarker, which reminds clinicians to pay more attention to the patients with negative pathological margin. Currently, there is no unified conclusion regarding which molecular biomarker is selected as the detection indicators. It requires a multicenter, large-sample prospective or retrospective experiment combined detection of multiple molecular biomarkers, while comparing the sensitivity and specificity.
Furthermore, there remains great controversy regarding whether adjuvant radiotherapy and chemotherapy should be actively used in patients with altered expression of gene or protein in surgical margins. And how to choose further treatment and their effects remain to be further clinical study. Further research on the accurate margin of laryngeal carcinoma can better guide clinical work, and most importantly improve the prognosis of patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Received financial support from Tianjin Health Bureau Science and Technology Fund (2011KZ75).