
Abstract
Intradiploic epidermoid cysts are benign tumors that account for ∼1% of all intracranial space occupying lesions. Because of the indolent growth, symptoms are usually gradual in onset with a prolonged duration. While they can originate from any part of the skull, temporal bone epidermoids are rare. We describe a case of an unusual presentation of a temporal bone epidermoid cyst. A 64-year-old male presented with sudden right-sided hearing loss and worsening right eyelid ptosis was found to have a nonenhancing lobulated mass above the right tegmen tympani with complex signal and possible communication with the apical turn of the cochlea on magnetic resonance imaging (MRI). He underwent subtemporal craniotomy with excision of the cyst lining and matrix without any complications and was discharged home on postoperative day 1. Complete excision was not possible given that the facial nerve and cochlea were improved. He had subjective improvement in his hearing immediately after surgery. Intradiploic epidermoid cysts are benign tumors that can present anywhere in the skull with variable presentation. While complete excision is the goal, neurovascular involvement may make this challenging. The use of computed tomography scan and MRI can prove to be invaluable in determining accurate diagnosis and size for surgical planning.
Introduction
Intradiploic epidermoid cysts are rare lesions that account for approximately 0.2% to 1% of all intracranial space occupying lesions. 1 They can originate from any part of the skull, with frontal and parietal bones being the most common. Epidermoids of the temporal bone are exceedingly rare, with only roughly 20 cases having been reported in the English literature. 2
Case Report
A 64-year-old male presented to an outside physician complaining of sudden right-sided hearing loss and worsening right eyelid ptosis after a flight. He was initially treated conservatively with high-dose steroids without improvement. He subsequently underwent contrast-enhanced magnetic resonance imaging (MRI) of the brain which revealed an 11 × 16 × 7 mm nonenhancing, lobulated mass centered above the anterior tegmen tympani with complex signal on T2 and possible communication with the apical turn of the cochlea (Figure 1). There was no evidence of brain parenchyma in the lesion. At this point, he was referred to our institution for definitive management. His tuning forks (256 and 512 Hz) lateralized to the ipsilateral side of the loss, and both forks demonstrated a conductive hearing loss. Physical examination revealed a normal ear canal and tympanic membrane bilaterally. Facial function was noted as House-Brackmann 1/6 bilaterally but did show mild right upper eyelid ptosis. His audiogram revealed right moderate-to-severe mixed hearing loss with absent reflexes. A computed tomography (CT) scan was performed which showed a lytic mass in the right temporal bone involving the superior aspect of the tympanic cavity with dehiscence of the apex of the cochlea (Figure 2). In addition, the mass involved the posterior wall of the right glenoid fossa medially as well as suspected partial erosion of the anterior surface of the head of the malleus. The facial nerve canal was indistinguishable from the mass anteriorly. When compared with a maxillofacial CT done 8 years prior to evaluation (for an unrelated issue), he was noted to have a smaller lesion without cochlear involvement present at that time.
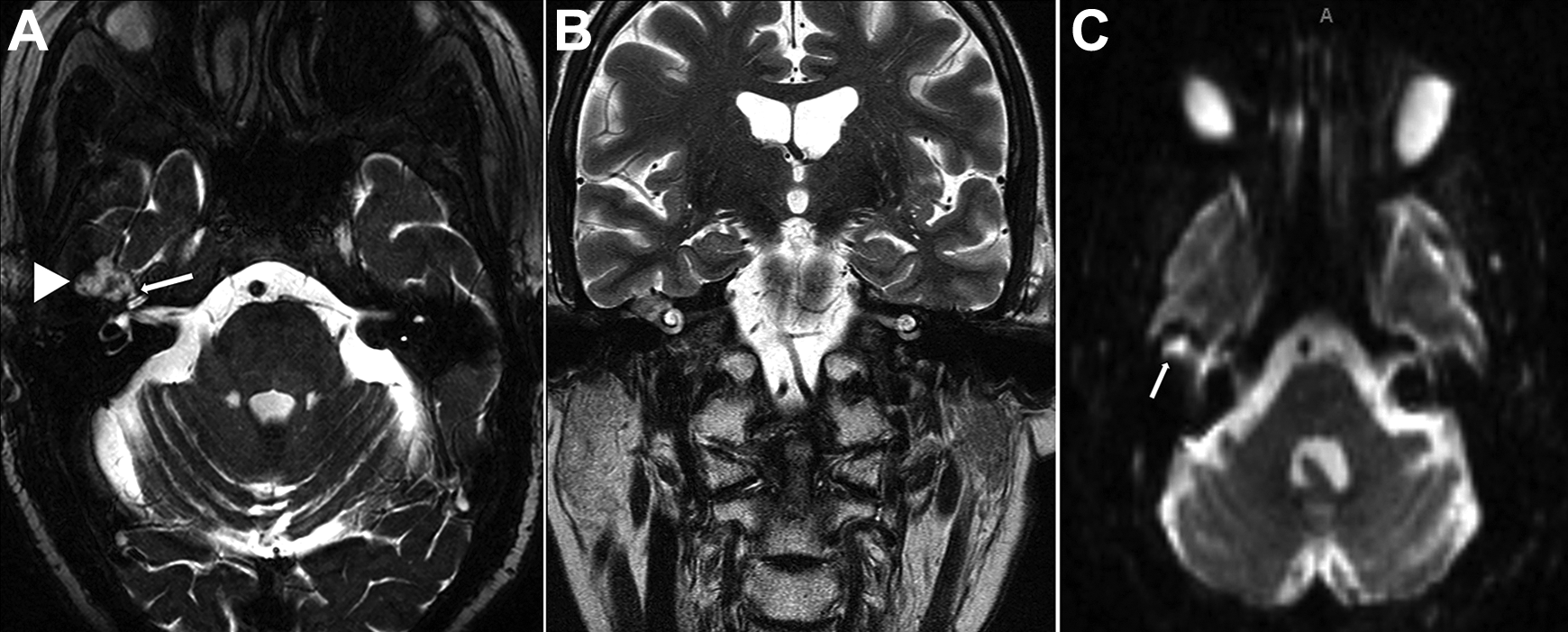
A, T2 axial MRI showing lobulated lesion (arrowhead) in the right subtemporal skull base with complex signal and communication with the apical turn of the cochlea (arrow). B, T2 coronal MRI. C, Diffusion weighted-imaging axial MRI (arrow). MRI indicates magnetic resonance imaging.
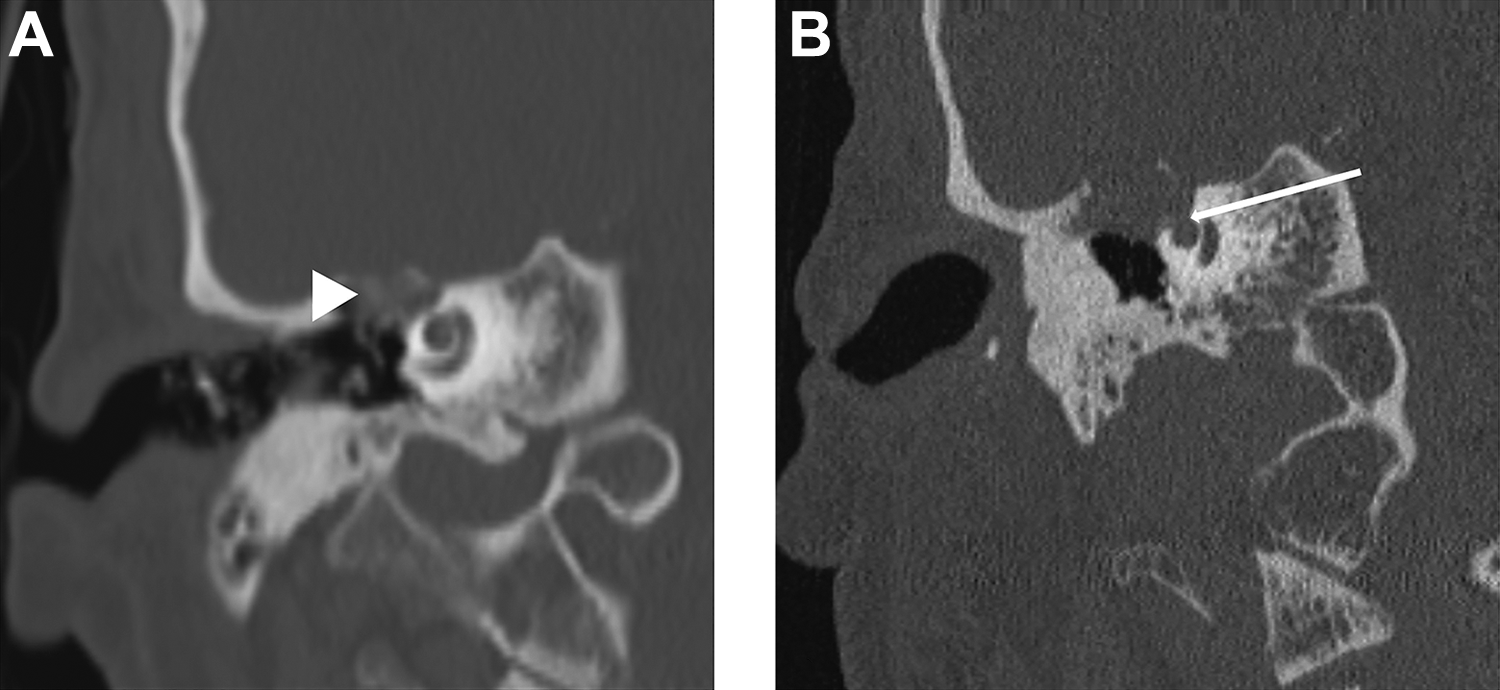
A, Coronal CT without contrast performed 8 years prior to surgery showing skull base erosion (arrowhead) at the anterior tegmen tympani. B, Recent coronal CT demonstrating growth of the lesion, now with communication (arrow) with the apical cochlea. CT indicates computed tomography.
After discussing the various approaches to address this suspected epidermoid, a subtemporal craniotomy for mass debulking was recommended. At the time of surgery, a pearly mass consistent with epidermoid was clearly visualized from above, at the tegmen tympani. A subtotal excision of the cyst lining and matrix was performed, taking care to leave matrix overlying the cochlear fistula and labyrinthine facial nerve. The ossicles were preserved. He tolerated the procedure well and was discharged home on postoperative day 1. He noted immediate subjective improvement in his hearing. His postoperative course was uneventful with unchanged objective facial nerve function, although subjective improvement by the patient. Repeat audiogram at 3 and 12 months showed an improved but persistent moderate mixed hearing loss (improved conductive hearing and stable sensorineural hearing).
Discussion
Epidermoid cysts are benign masses lined with stratified squamous epithelium that contain keratin, cellular debris, and cholesterol. They are commonly found in the cerebellopontine angle but can originate in the temporal bone as a result of obstructed squamous epithelium. Because of the slow growth rates of these cysts, patients are often asymptomatic at the time of diagnosis. When symptoms are present, they are gradual in onset with a prolonged duration. 1,3 Symptoms are related to the direction of spread which can occur into the mastoid, middle ear, middle fossa, inner ear/cochlea, facial nerve, internal auditory canal, or intradural. The complete intratemporal nature of this growth makes this case somewhat unique in this regard and is, to our knowledge, the first reported cases of sudden sensorineural hearing loss caused by an epidermoid.
The differential diagnosis for a mass in the tegmen tympani includes epidermoid, cholesteatoma (acquired or congenital), cholesterol granuloma, mucocele, encephalocele, hemangioma, facial nerve tumor, and a variety of rarer neoplasms. Both CT and MRI can be helpful to make the diagnosis. Epidermoid cysts usually appear as a homogenous, lobulated mass with clear demarcation on CT that is hypo- or isodense with the brain. On MRI, they classically appear heterogeneous and hypointense on T1-weight imaging and also do not enhance with contrast. However, on T2-weighted imaging, they are hyperintense but are reported to be less intense than cholesteatoma. 4 Diffusion weight imaging, the best imaging sequence in diagnosing epidermoid cysts often shows restricted diffusion with higher signal intensity than that of cerebrospinal fluid (CSF). 5
For any tumor of the tegmen tympani, 3 surgical approaches can be considered—subtemporal/middle fossa craniotomy, transmastoid, and endoscopic. These approaches are generally determined by a variety of variables including age, gender, type of temporal bone pathology, history of previous surgery, size and location of tumor, and clinical presentation. A subtemporal/middle fossa approach allows for better visualization of more medial structures including the internal auditory canal, facial nerve, and greater superficial petrosal nerve while offering the possibility of facial function and hearing preservation. 6 However, such an approach requires a craniotomy with its attendant risks, along with potentially prolonged retraction of brain, leading to increased incidences of parenchymal and neurovascular injury as well as postoperative complications such as CSF leakage, meningitis, and epilepsy. 7 The transmastoid approach may also be considered for tumor excision or decompression especially when the pathologic lesion is located on the tympanic or mastoid segment. But given the somewhat confined scope of view in this approach, it may not be optimal in cases when certain structures are to be clearly exposed, such as the geniculate ganglion, in which alternative approaches might provide a more superior exposure. 7 The recent introduction and acceptance of otoendoscopic surgery to treat these tumors offer other advantages as it provides direct surgical access to the lesions and minimizes the risks and complications associated with brain manipulations, all while also maximizing aesthetic outcome and hastening recovery time. 8 In extensive disease, the endoscopic transcanal approach, such as translabyrinthine-transcochlear approach, provides the anatomical advantage of reaching the lesion with minimal soft tissue dissection as well as leaving vital adjacent structures, such as the mastoid, untouched. However, this approach requires facial nerve mobilization in which skeletonization of the nerve would carry a higher risk of postoperative facial nerve dysfunction.
In this particular case, the radiologic findings in this case, and notably the CT scan performed 8 years prior to presentation, provided critical information for the presurgical decision-making process. The extremely slow-growing nature of this mass combined with the low likelihood of hearing preservation by complete excision led to the decision to excise/debulk. The subtemporal approach was selected based on patient age, ease of access, visualization of the adjacent dura involved by tumor, and the ability to reconstruct the skull base to better prevent against future encephalocele formation. Likewise, exteriorization of the tumor sac to the middle ear and mastoid would have required at least partial removal of the ear canal wall and the subsequent inconveniences of office-based debridement. While the middle fossa approach proved to be successful for this patient, depending on age, growth rate, location, hearing, and facial nerve function, the other approaches may prove to be equally as successful.
Conclusion
Intradiploic epidermoid cysts of the temporal bone are rare masses, and their presentation may be minimally symptomatic, if at all. We present a usual case of sudden sensorineural hearing loss secondary to cochlear invasion. Although complete excision of these cysts is optimal, proximity to neurovascular structures may preclude this due to unacceptable morbidity. Accurate diagnosis and estimation of size and spread by both CT and MRI can prove invaluable in surgical planning, especially in cases where hearing and facial function preservation are prioritized.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.