
Abstract
Aim:
The aim of this study was to determine the correlation between nasal function assessment and anxiety scales.
Methods:
A total of 120 patients with the complaint of nasal obstruction were classified as nasal septum deviation group (DNS) and no nasal pathology group (NON). A control group was formed of 57 healthy participants. Nasal obstruction severity was assessed using the Nasal Obstruction Symptom Evaluation (NOSE) scale, nasal resistance level with rhinomanometry and anxiety levels with the Agoraphobic Cognitions Questionnaire (ACQ), and the Body Sensations Questionnaire (BSQ).
Results:
There was a statistically significant difference between both the DNS and the NON groups and control group in terms of NOSE scale, ACQ, and BSQ (P < .001). The total nasal resistance values were higher in the DNS group compared to both the NON and control groups (P < .001), although the difference between the NON group and control group was not statistically significant.
Conclusion:
The results of this study showed that patients with nasal breathing complaints, but no organic pathology, had the same level of nasal obstruction symptoms as patients with nasal septal deviations. Anxiety levels are elevated in patients with symptoms of nasal obstruction, even when there is lack of organic nasal pathology.
Keywords
Introduction
Nasal pathologies constitute serious airway problems, as the nasal cavity contributes to more than half of the total airway resistance. 1 Nasal pathologies such as septum deviation and concha hypertrophy can impair the nasal opening due to narrowing of the nasal cavity and increased resistance to airflow. 2,3 Nasal obstruction is one of the most common reasons for patients to visit the ear, nose, and throat (ENT) specialist, and nasal septum deviation (DNS) is common among these patients4,5
Symptoms of nasal obstruction are subjective and can therefore be misleading. On the other hand, the findings of nasal examination and endoscopic evaluation may not always correlate with the complaints of patients. While, sometimes severe deviations, giant concha bullosa or advanced inferior concha hypertrophies cause minimal nasal obstruction, in some patients it may be completely asymptomatic, and occasionally minimal nasal pathologies can cause a feeling of serious nasal obstruction. This feeling of obstruction can also cause a high degree of anxiety in patients.
In this study, patients who applied to our clinic with the complaint of nasal obstruction were divided into 2 groups as those diagnosed with DNS and those with no nasal pathology (NON) through clinical examination by headlight and nasal speculum and endoscopic evaluation findings. It was aimed to determine the correlation between objective and subjective evaluation tests and anxiety scores in these groups.
Methods
The study included 120 patients, comprising 64 females and 56 males, aged 18 to 60 years, with no systemic disease or chronic drug use history who presented at our polyclinic with complaints of nasal obstruction between May 2016 and November 2016. A prospective evaluation was made of the Nasal Obstruction Symptom Evaluation (NOSE) scale values, and total nasal resistance (TNR) values calculated according to rhinomanometry measurements and anxiety scores. Approval for the study was granted by the Ethics Committee of our hospital (Ref No: 5409). Informed consent was obtained from all the study participants.
Patients were evaluated for DNS, nasal polyp, concha bullosa, allergic rhinitis, acute, and chronic infectious diseases according to anterior rhinoscopic examination with nasal speculum and endoscopic examination findings using a 3.2-mm flexible fiberoptic nasopharyngoscope (Stema Medizintechnic GmbH, Stockack, Germany). Computed tomography (CT) of nose and paranasal sinuses 5-mm thick imaging scans in the axial, coronal, and sagittal planes was recorded (Aquillon64, Toshiba, Otawara, Japan). The patients were divided into 2 groups: those with DNS and those with NON. Patients with nasal polyps, allergic rhinitis, and acute and chronic infectious diseases were excluded from the study. A control group was formed of 57 patients who had no complaints of nasal obstruction, no findings of any nasal obstruction by examinations, and no systemic disease.
The NOSE scale was used to assess subjective symptoms of nasal obstruction. This scale consists of 5 questions. Each question is rated from 0 (no problem) to 4 (serious problem). The results were evaluated by multiplying the data by 5 to obtain a balanced scale between 0 and 100.
In this study, rhinomanometry was applied to each patient to objectively evaluate the patient complaints. The rhinomanometry test was applied in a room at a temperature of 25°, and patients were admitted to the room 20 minutes prior to the rhinomanometry test. The device was opened 30 minutes before the test and was calibrated before each patient. Active anterior rhinomanometry (Rhinoscan version 2.6; Interacoustics, Denmark) was performed 3 times in the right nostril and 3 times in the left nostril, requiring the patient to breathe at a constant speed from the nose after 10 minutes of spraying with 1 mg xylometazoline hydrochloride in both nostrils. Total nasal resistance values were calculated to exclude the nasal cycle according to rhinomanometry results. All measurements were made at a pressure of 150 Pa, determined according to international standards. 6
Each patient was requested to answer questions in 2 separate questionnaires: the Agoraphobic Cognitions Questionnaire (ACQ) consisting of 14 questions and the Body Sensations Questionnaire (BSQ) composed of 17 questions for the assessment of anxiety.
The ACQ is a self-administered questionnaire with 14 items. This questionnaire measures the cognitive properties of the fears associated with agoraphobia. The frequency of catastrophic thoughts that arise in anxious situations is evaluated on a 5-item scale. There are 2 subscales that measure the concerns of the physical aspect and the concerns in the social behavioral area. The validity and reliability study of the Turkish version was carried out by Kart and Türkçapar. Raw points are used when scoring. 7,8 The BSQ is also a self-administered questionnaire that measures many physical feelings about being afraid of fear (fearful of physical symptoms of anxiety) with 17 items. Anxiety caused by physical symptoms is scored on a scale of 5 points. Cronbach α values varied from 0.89 to 0.94. The validity and reliability of the Turkish version of the scale were determined by Kart and Türkçapar. 7,9
Statistical Analysis
Statistical analyses were made using IBM SPSS for Windows Version 22.0 software. Numerical variables were stated as mean ± standard deviation and median (Min-max) values. Categorical variables were stated as number (n) and percentage (%). The Kolmogorov Smirnov test was used to examine whether the numerical variables showed normal distribution. The similarity of group variances was investigated with the Levene test. One-way analysis of variance was used when parametric test assumptions were provided in group comparisons, and the Kruskal-Wallis test was used when not. When differences were determined, binary comparisons were made with the Tukey test or the Siegel Castellan test. The relationship between categorical variables was determined using the chi-square test. The relationship between numerical variables was shown by the Spearman correlation coefficient. A value of P < .05 was accepted as statistically significant.
Results
The DNS group comprised 34 (43.6%) males and 44 (56.4%) females with a mean age of 33.1 ± 11.8 years. The NON group comprised 22 (52.4%) males and 20 (47.6%) females with a mean age of 36.4 ± 12.3. Control group comprised 20 (35.1%) males and 37 females (64.9) with a mean age of 38.2 ± 13.5. There was no significant difference between the 3 groups in terms of age and gender (Table 1).
Age and Gender Comparison Between the Groups.

Abbreviations: F, female; DNS, nasal septum deviation; M, male; NON, no nasal pathology.
The NOSE scale value was 65 in the DNS group, 50 in the NON group, and 0 in the control group. The ACQ values were 4 in the DNS group, 5 in the NON group, and 0 in the control group. The BSQ value was 14 in the DNS group, 15 in the NON group, and 1 in the control group. The TNR values were 0.24 in the DNS group, 0.16 in the NON group, and 0.16 in the control group. There was a significant difference between DNS and control groups in terms of NOSE, ACQ, BSQ, and TNR values (P < .001). There was a significant difference in NOSE, ACQ, and BSQ values between NON and control groups (P < .001); however, there was no difference between TNR values (P = .549). There was a significant difference in the TNR values between the DNS and the NON groups (P < .001); however, no difference was found in terms of NOSE (P = .514), ACQ (P = .805), and BSQ values (P = 1.000; Table 2).
Comparison of NOSE, ACQ, BSQ, and TNR Values Between the Groups.
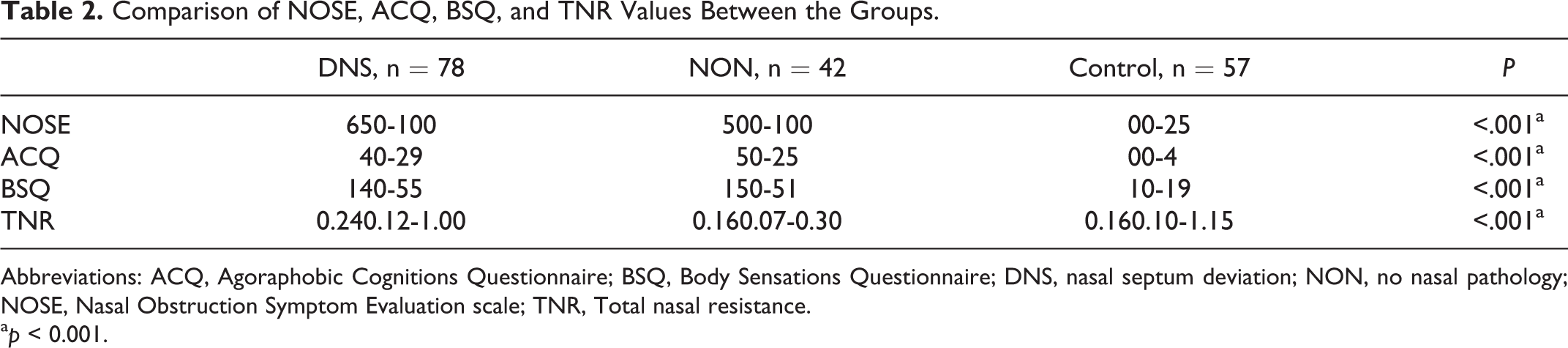
Abbreviations: ACQ, Agoraphobic Cognitions Questionnaire; BSQ, Body Sensations Questionnaire; DNS, nasal septum deviation; NON, no nasal pathology; NOSE, Nasal Obstruction Symptom Evaluation scale; TNR, Total nasal resistance.
ap < 0.001.
There was a positive correlation between ACQ and BSQ values and NOSE scale in all 3 groups. There was a negative correlation between NOSE, ACQ, BSQ, and TNR values (Table 3).
Correlation Between NOSE, ACQ, BSQ, and TNR Values Between all Groups.
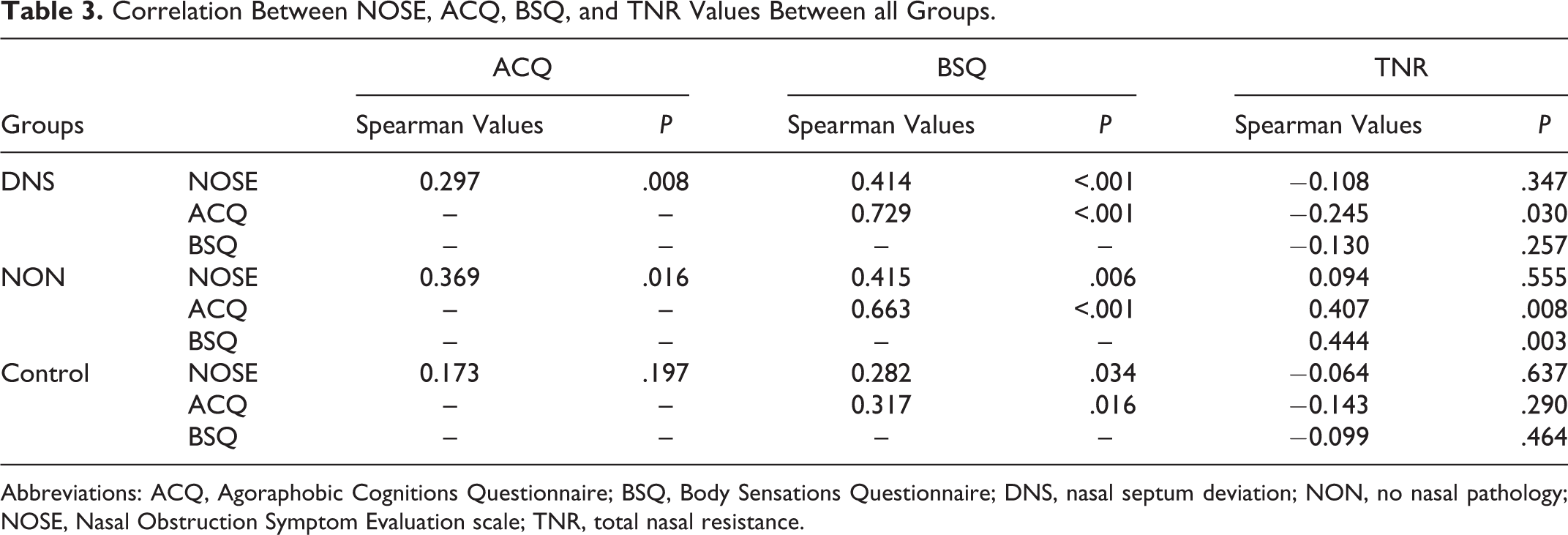
Abbreviations: ACQ, Agoraphobic Cognitions Questionnaire; BSQ, Body Sensations Questionnaire; DNS, nasal septum deviation; NON, no nasal pathology; NOSE, Nasal Obstruction Symptom Evaluation scale; TNR, total nasal resistance.
Discussion
Two important results emerged from this study: (1) There was a significant relationship between nasal obstruction symptoms and anxiety level. (2) Not only the increase in nasal resistance due to deviation of the nasal septum but also the belief that the patient cannot breathe psychologically is associated with anxiety.
Nasal obstruction is a symptom that should be carefully considered, as there is more than 1 etiology, and it is the most frequent cause of patients presenting with sinonasal diseases to ENT physicians. Obstruction could be due to mucosal causes such as allergic/nonallergic rhinitis, rhinosinusitis, and nasal cycle, as it can arise from many structural events that reduce the internal nasal volume such as nasal septal deviation, nasal valve pathologies, concha hypertrophy, concha bullosa, nasal polyps, and tumors. 10,11 As a result, it is thought that nasal obstruction may lead to psychological problems due to brain electrolyte imbalance, which results from the fact that blood pH levels reach more acidic levels due to an increased blood CO2 level. 1
Although there are a number of causes that can lead to nasal obstruction, there is sometimes no underlying pathology, despite all the investigations. Therefore, it is very important to determine whether nasal obstruction is caused by an organic pathology or not in the preoperative period in terms of both patient and physician. Our study’s subjective assessment findings of the patients presenting at the clinic with nasal obstruction complaints without nasal pathology were found to be at the same level of severity as those patients with advanced septum deviations, and the severity level of anxiety was also found to be the same. When the TNR values of these patients were examined, they were found to be significantly lower than those of patients with septum deviation. These patients believe that there is an underlying organic nasal pathology because they cannot breathe through the nose, and although the nasal resistance values are at the same level as the normal population, they have the same symptoms as patients with DNS. They visit many different ENT physicians in the belief that they have an organic pathology. It is very difficult to convince these patients that they are normal. Avoidance behaviors and psychological symptoms due to severe anxiety and fear become inevitable in these patients. Many studies have reported that people with somatic anxiety symptoms apply to other medical branches instead of the psychiatry clinic. 12,13 The results of the current research also support this view.
Anxiety disorders are common conditions that include separation anxiety disorder, specific phobias, social phobias, panic disorder, agoraphobia, generalized anxiety disorder, nonspecific anxiety disorder, posttraumatic stress disorder, and obsessive–compulsive disorder. If anxiety disorder is linked to unavoidable fears, it can be caused by agoraphobia, and these patients show avoidance behavior in environments where it is not possible to receive urgent medical services such as in crowded places and shopping centers. 14 -16 It has been reported that the fears are due to anxiety disorders associated with increased blood pressure and respiratory rate and the feeling of chest tightness. 15 To the best of our knowledge, however, there are not enough studies in the literature that have investigated the effect of anxiety disorder on nasal breathing.
In addition to physical symptoms such as an increase in heart rate and shortness of breath, it is considered to be a defining feature of panic in cognitive symptoms such as loss of control, insane, and fear of drowning and death. In the literature, a large number of studies have shown that patients with panic disorder are more likely to be concerned about their anxiety and are more susceptible to physical changes and thus misinterpret these bodily changes more frequently. When people with panic disorder were compared to healthy individuals, it was observed that they were more anxious to observe and perceive their bodies more closely and to interpret the changes. In a prospective study conducted by Godeman et al in 93 patients with vestibular neuronitis, they followed these patients for 2 years and reported that the variance of vertigo anxiety in the development of panic and somatoform disorder gradually increased to 60% at the end of 2 years. 17
There have been studies that have investigated the objective and subjective improvement in septoplasty on nasal obstruction. However, it must be accurately demonstrated that the nasal obstruction is really connected to an organic nasal pathology and presence of the surgical indication of this pathology because unnecessary nasal surgery may not improve the patient’s complaints but rather lead to further complaints. 18,19
Li et al. evaluated 44 septum deviations and 37 control group patients who received a diagnosis of septum deviation, and the prevalence of depression and anxiety in patients with DNSs was found to be higher than in the control group. 20 In our study, this relationship with a much larger number of patients was similarly demonstrated. In addition, this study proves that not only deviation of the nasal septum but also the belief that nasal pathology exists (although nasal functions are completely normal) increases the level of anxiety. In the literature, a similar relationship between nasal obstruction and anxiety has been demonstrated with obstructive sleep apnea syndrome (OSAS) and seasonal allergic rhinitis. 21,22,1 In one study, anxiety symptoms were reported to be even more severe than allergic rhinitis symptoms. 21
This connection of anxiety with nasal obstruction can also affect the success of surgery. Studies have shown that people with a high level of anxiety have lower rates of postoperative satisfaction. Saragusty et al. reported that patients with high attachment anxiety had much lower levels of quality of life, improvement in nasal obstruction, and facial pain rates in the postoperative period. The association of operative success with the person’s mental status and personality traits was demonstrated. 23
The most important limitation of this study is the lack of postoperative anxiety levels. Knowing whether there is a decrease in postoperative anxiety scores in patients with septum deviation may be beneficial in terms of showing the effect of treatment of nasal obstruction on anxiety. Hence, future studies are needed to support or disapprove these results.
Conclusion
The results of this study showed that patients with nasal breathing problems had the same level of nasal obstruction symptoms as patients with DNSs, although there were no organic nasal pathologies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.