
Abstract
The purpose of this study was to investigate the effects of craniofacial structure and nasal septal deviation on frontal sinus morphology 3-dimensionally. This study of anatomy, anthropology, morphology, and radiology included 74 dry skulls as study sample. The craniofacial measurements were made through conventional anthropometric methods by the use of calipers. The nasal septal deviation measurements were done by computerized software on photographs taken from frontal view. Frontal sinus volumes were estimated by the computerized tomography-based volumetry. The relationships between craniofacial structure, nasal septal deviation, and frontal sinus morphology were tested by linear regression and correlation analysis. The analysis of numerical variables and categorical variables within different groups was done by Mann-Whitney U/Kruskal-Wallis, and χ2 tests, respectively. There appeared a positive relationship between the dimensions of the frontal sinuses and the maximal cranial length and the nasal height especially on the left side (P < .05). However, after multivariate linear regression model for both factors was created, solely the nasal height kept being a positive factor for frontal sinus size as an independent variable. No statistical relevance was detected between the presence of metopic suture and frontal sinus morphology. Septal deviation itself affected frontal sinus morphometry, but the morphometry did not differ between the deviation side and the opposite side. In conclusion, the cranial structure does not affect the frontal sinus morphology but nasal structure affects. The true influences, among measured craniofacial elements, in relationship with the pneumatization of frontal sinus are appeared to be the nasal structure related.
Introduction
The frontal sinus (FS) is a unique anatomical structure that varies in size and shape and has a different morphology across individuals. André Vésale (1514-1564), known as the founder of anatomical science, described the FS as “a cave full of air” in his famous book “De-Humani Corporis Fabrica libri septem.” 1
In terms of evolutionary development, most studies examining the anatomy of the FS were conducted in primates. Orangutans, unlike African apes and humans, do not have an FS. 2 In 2000, Blaney noted that the FS was found only in humans and in some large African apes, and there were racial variations in FS size among the African Great Ape populations, which mirrors the human condition. 3 This is why it is not surprising that several fields have placed much emphasis on the FS for its key roles in areas such as anatomy, paleontology, anthropology, and forensic medicine given its unique structure. Furthermore, the FS has been used as a biometric marker, similar to fingerprints, for individual identification. 4
The development of the FS begins late and is not present at birth. In the first year of life, primary pneumatization of the frontal bone is rather slow. Rapid pneumatization begins at the age of 2 years from the beginning of sequestering pneumatosis to adolescence, and after about 3 years, the FS becomes visible by computerized tomography (CT). Pneumatization of the FS, which becomes detectable at age of 8 years firstly, continues until approximately 18 to 20 years of age. 5,6 Possinger and Bookstein describes the development of the sinus according to age in the study of FS morphometry. 7 Studies from Ruf and Panchez on FS development in relation to somatic development and skeletal development have shown that the largest dimensional increase in FSs and optimal recognition of the sinuses are accompanied by increases in body height after the peak age of 1.4 years. 8
Some clues exist about the relationship between craniofacial structure and FS morphology. Although its ontogenic development is grounded in the development of the first and second ethmoturbinalles 9 , FS development has been associated with craniofacial structure and the presence of metopic suture dating back to Schaeffer findings. 6 Another study showed that nasal pyriform aperture size, head measurements such as curvature, and spino bregmatic height also play roles in FS development. 10
It is known that the structure of the FS differs across climatic regions or in communities with different ethnic origins. 11 -15 As craniofacial development is also affected by these factors, it is worth investigating whether there is a linear relationship between FS morphology and craniofacial morphology. Some studies have shown a relationship between FS aplasia and the presence of a peristaltic metaplastic suture, a fusion anomaly in the cranial developmental process. 16 -19 However, predicting FS morphology according to craniofacial structure is considered an advanced research area. 20
This study sought to investigate the relationships between FS morphology and craniofacial structure in Aegean Turkish individuals using conventional anthropometry and CT-based volumetry.
Materials and Methods
Individuals
After the Ethics Committee of Dokuz Eylul University approved the study, we scanned dry skull collections available in the Department of Anatomy of Dokuz Eylul University Medical Faculty to determine suitability for 3-dimensional measurements. Seventy-four adult skulls in the craniofacial study collection with complete cranial and facial bones and an intact bony nasal septum were included in the study.
Anthropometric Studies
Craniofacial measurements were made with conventional anthropometric methods using 0.01-mm-sensitive calipers. Craniofacial anthropometric distances were measured as indicated by Vallois, who identified the cephalometric points of the craniofacial indices. 21
Photographic Studies
Photographs of the 74 skulls were shot at the “norma frontalis” position. 22 A 1-mm pitch ribbon ruler was used during the shots in order to calibrate the measurement unit in each photographic image. By using the “UTHSCSA Image Tool for Windows version 3.00” program, measurements of bony nasal septal deviation (BNSD) and facial asymmetry were performed with the photographs (Figure 1).
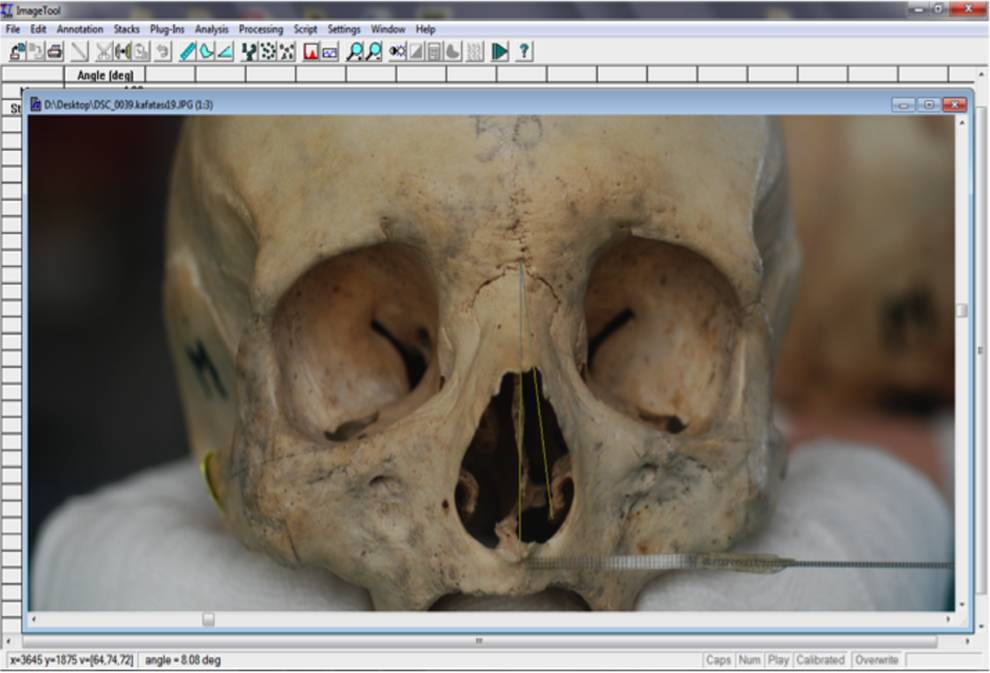
Photographic measurements for bony nasal septal deviation.
Classification of BNSD
The presence of BNSD was classified according to the diagnostic value points of “deviation width” defined in the photographic measurements of a thesis study conducted in our department. 23 A “no deviation” diagnosis was made for deviation widths less than 2.62 mm, and an “absolute deviation” diagnosis was given for widths greater than 4.24 mm. No BNSD classification was made for deviation values between 2.62 and 4.24 mm. 23
Computerized Tomography-Based Volumetry Analysis
The CT images in this study were obtained using a “Brilliance” model 64-canal (Philips, Amsterdam, the Netherlands) CT unit, and volumetric procedures were performed with the cursor using the area magnification algorithm with a procedure (Figure 2) previously defined by this study group. 24 One hundred forty-eight FSs of the 74 skulls were evaluated separately for measurements of FS width (FSW), FS height, FS depth (FSD), and FS volume (FSV). Frontal sinus pneumatization was classified according to the defined diagnostic cutoff values including “hypoplasia” for FSV less than 1131.25 mm3, “hyperplasia” for FSV greater than 3328.50 mm3 and “medium-sized” if FSV was between 1131.25 and 3328.50 mm3.
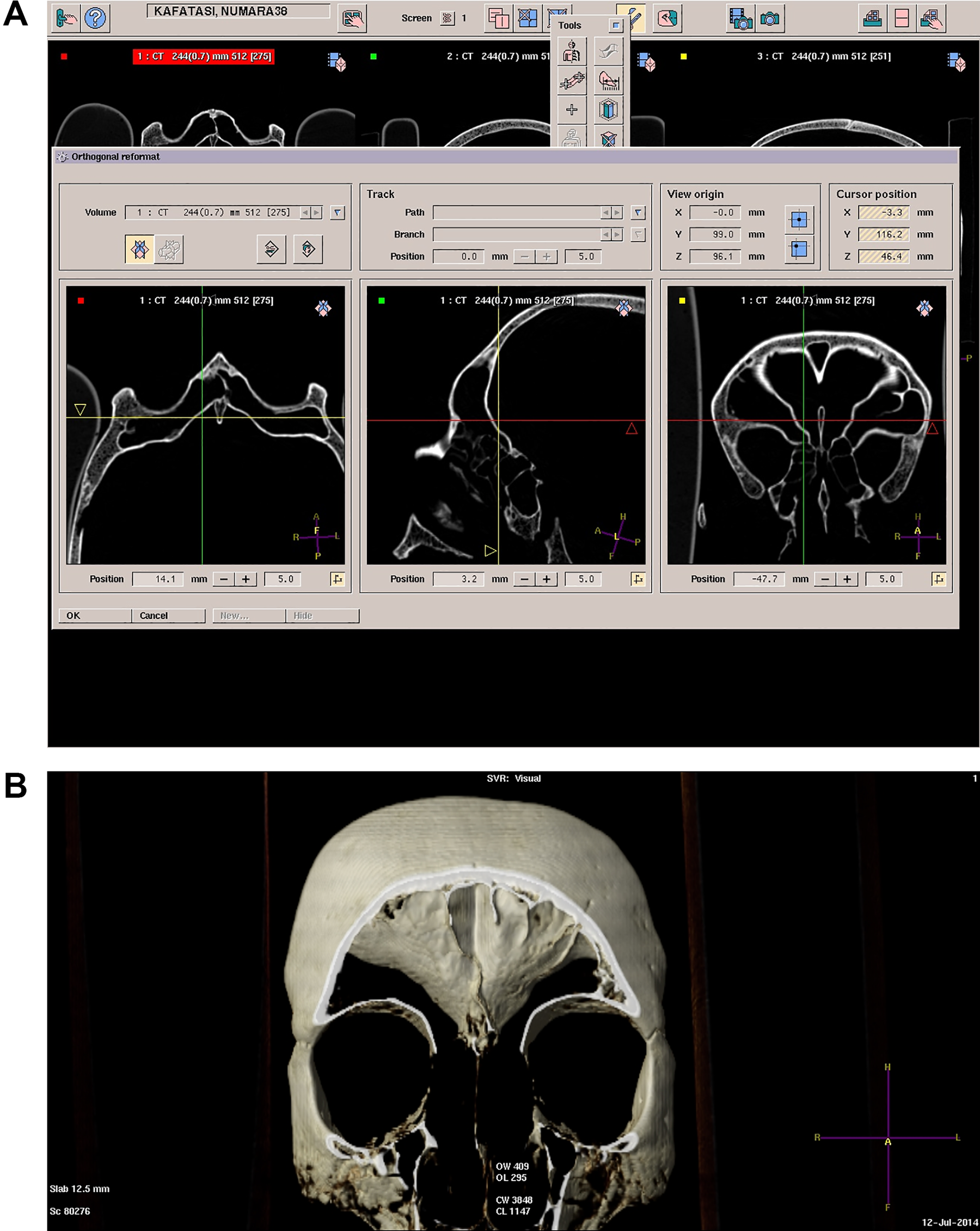
Frontal sinus segmentation (A) and volumetric study (B) on 3-D CT. 3-D CT indicates 3-dimensional computerized tomography.
Calculation of the FSV Asymmetry Ratio
The FSV asymmetry ratio (FSVAR) was calculated using the following formula 25 :
FSVAR (%) = (right FSV − left FSV)/((right FSV + left FSV)/2) × 100.
Classification of FS Pneumatization
Grouping of FS pneumatization variations was established according to previously defined diagnostic cutoff volumetric values from this research group. 24
Statistical Analysis
For numerical variables, means, standard deviations, minimum, and maximum values were estimated to define craniometric examination measurements, photographic BNSD measurements, and CT-based morphometric examinations of the FSs.
Relations between craniofacial structure, nasal septal deviation, and FS morphology were tested by linear regression and supported by correlation analysis. The significant variables were examined by multivariate analysis with linear regression modeling to identify independent risk factors. Numerical variables were compared among different groups using Mann-Whitney U/Kruskal-Wallis tests. Chi-square test and Fisher exact tests were used to analyze categorical variables among the different groups. Relationships of numerical parameters between 2 different sides of FSs were analyzed by paired t test.
All statistical analyses were performed using the SPSS version 20.0 software package for Windows (SPSS Inc, Chicago, Illinois). The results were evaluated with 95% confidence intervals, and P < .05 was considered to be statistically significant.
Results
The anthropometric measurements and indices (Table 1) of 74 skulls revealed that, in general, the Aegean region population has a cranium type of medium/wide head, wide forehead, medium upper face, and narrow nose (Table 2). Among 74 dry skulls, FS aplasia was found in 3 skulls bilaterally and there was no any unilateral aplasia noted. The measurements of BNSD also showed that this population generally has a deviated nose, plus 28 skulls showed a deviation between the 2.62 and 4.24 mm definitive values and thus were not classified as an absolute deviation type.
The Craniofacial Characteristics of the Dry Skulls Regarding Conventional Anthropometry.
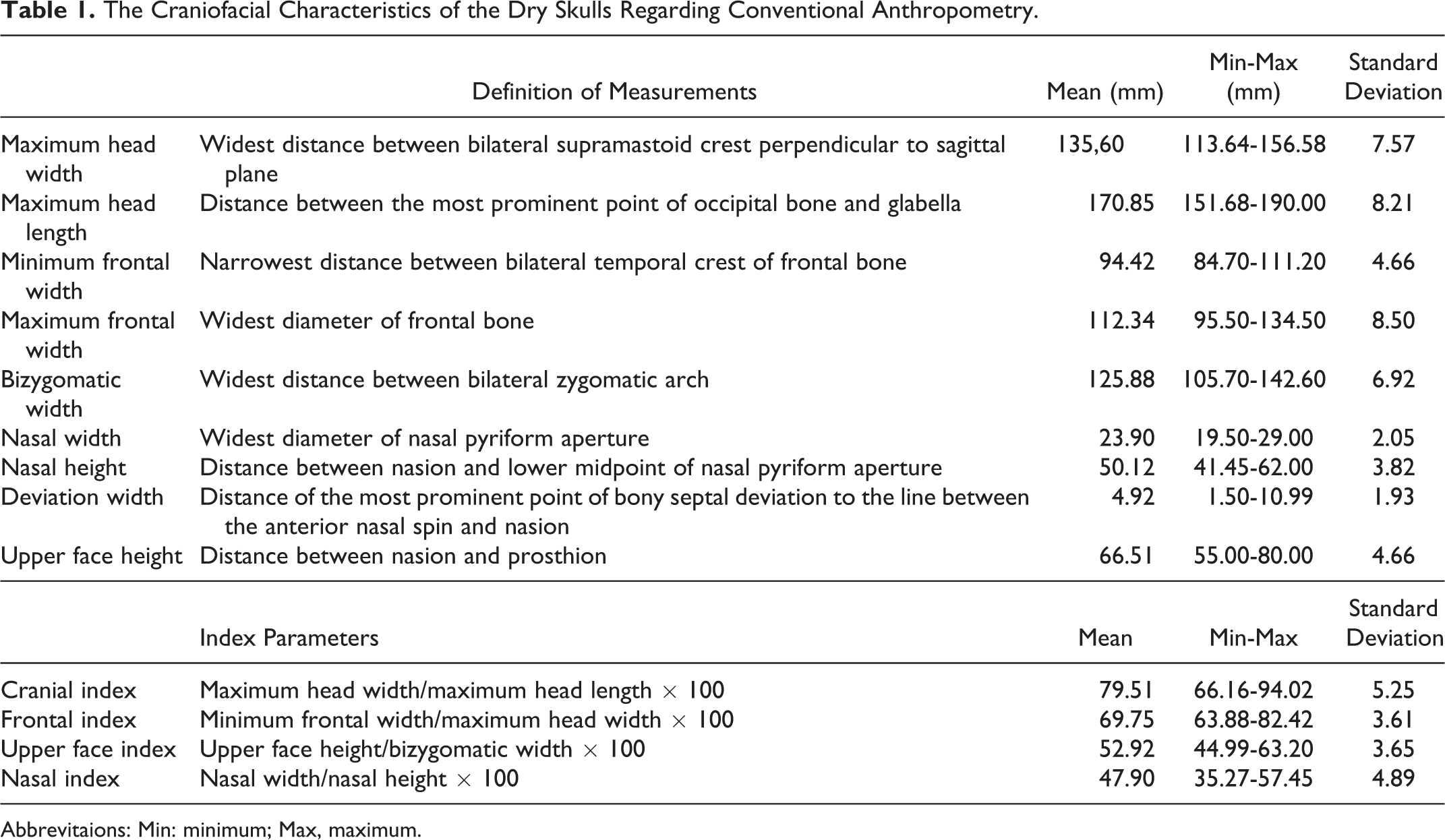
Abbrevitaions: Min: minimum; Max, maximum.
The Morphologic Grouping of the Dry Skulls Regarding Craniofacial Indices.
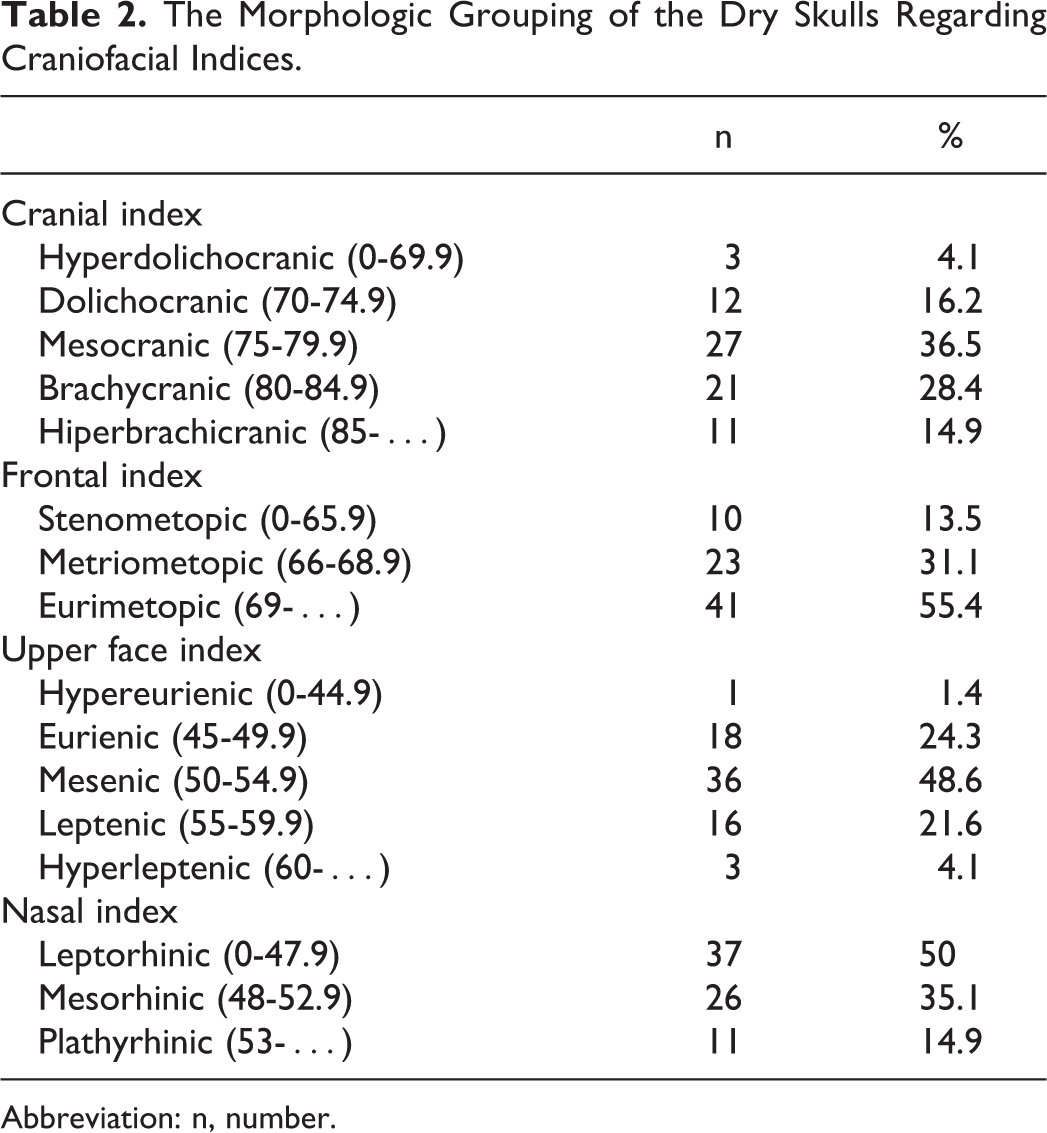
Abbreviation: n, number.
In the univariate linear regression analysis, a model was created with the “maximum head length” and “nasal height” variables that were found to influence the length and volume measurements of the FSs independently of the other variables (Table 3). The analytic results of the model are shown in Table 4. The model’s “Adjusted R 2 ” value showed that this model correctly estimated right sinus volume in 9.1% of the samples and estimated left sinus volume in 13.6% of the samples. Thus, a model including maximum head length and nasal height together was not detected to have a powerful effect on FSV (P > .05). However, nasal height was correlated with FS morphometry in the model for left-sided measures (Table 4).
The Analytic Findings of Univariate Linear Regression With Respect to the Craniometric Variables If They Affect The Frontal Sinus Morphometry.
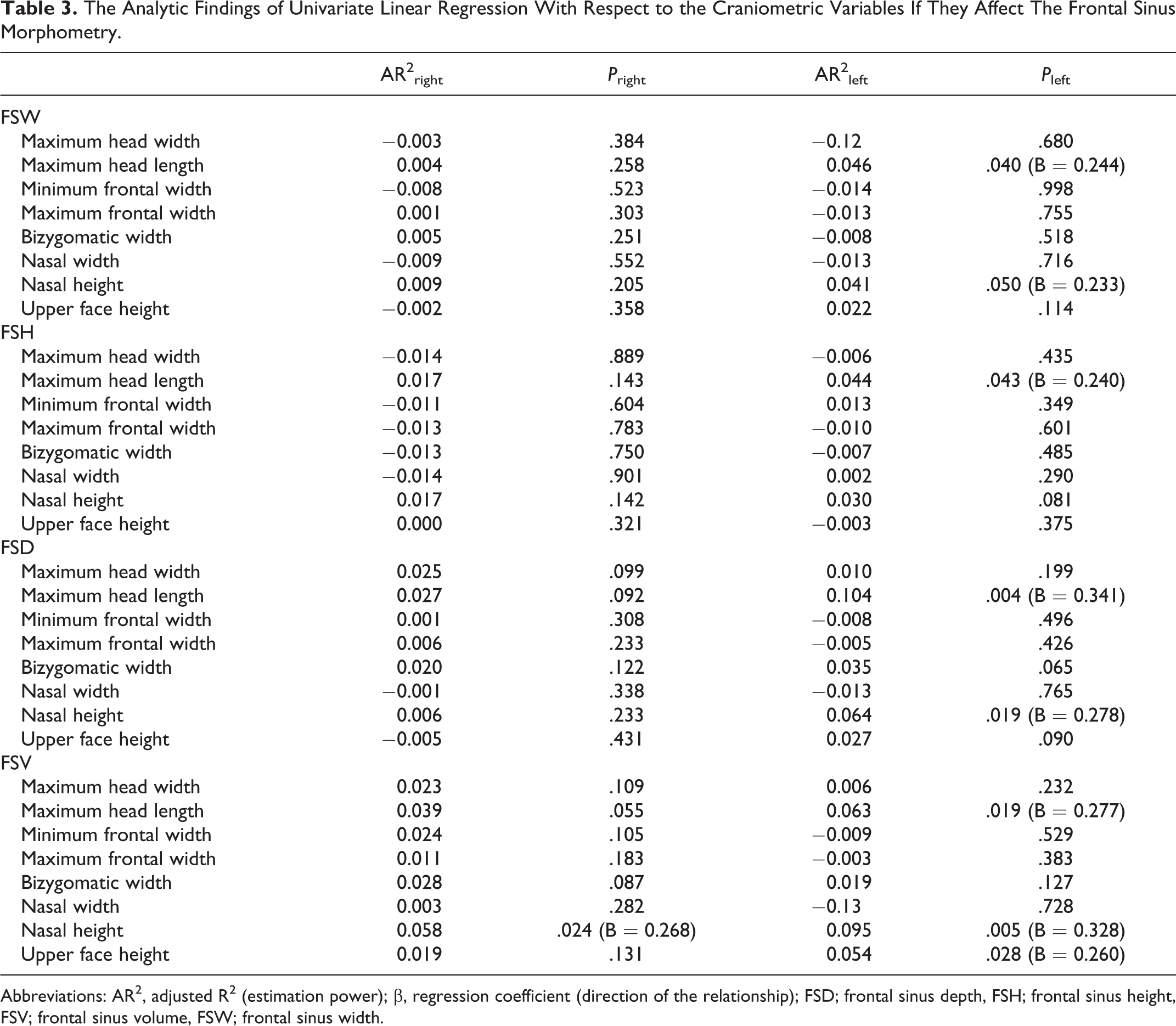
Abbreviations: AR2, adjusted R2 (estimation power); β, regression coefficient (direction of the relationship); FSD; frontal sinus depth, FSH; frontal sinus height, FSV; frontal sinus volume, FSW; frontal sinus width.
The Findings of Multivariate Linear Regression Analysis With Respect to the Independent Craniometric Variables If They Affect the Frontal Sinus Morphometry.
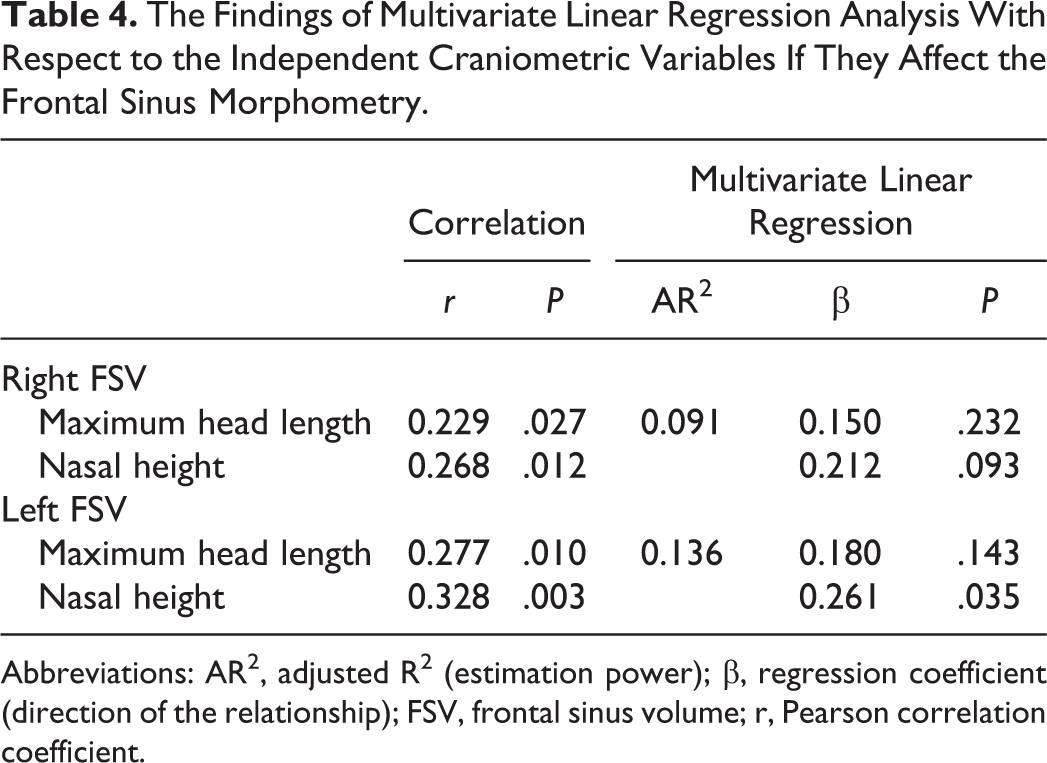
Abbreviations: AR2, adjusted R2 (estimation power); β, regression coefficient (direction of the relationship); FSV, frontal sinus volume; r, Pearson correlation coefficient.
The numbers and percentages of differently pneumatized FSs within the craniofacial and BNSD groups are shown in Table 5. We identified several significant relationships with respect to craniometric variables among the FS pneumatization subgroups of aplasia/hypoplasia, medium size, and hyperplasia using the Kruskal-Wallis test; these included maximum head length (P = .05), upper face height (P = .039), and nasal height (P = .045) for right-sided FS subgroups and maximum head length (P = 001), bizygomatic width (P = .018), and nasal height (P = .015) for left-sided FS subgroups. However, similar to most other craniometric measurements and indices (except for maximum head length and nasal height; Tables 3 and 4), craniofacial structure type also did not show a relationship with FS length and FSV measurements according to the inverse nonparametric analysis comparing the different craniofacial morphologies (Table 6). Frontal sinuses were mostly medium-sized in the non-BSND group, whereas they were mostly hyperpneumatized in both the unclassified and absolutely present BNSD groups. In contrast, BNSD is positively correlated with the FSW and FSV measurements, as FSW and FSV increased with the presence of BNSD (Table 6).
The Number and Percentages of Differently Pneumatized Frontal Sinuses Within Craniofacial and Bony Nasal Septal Deviation (BNSD) Groups.
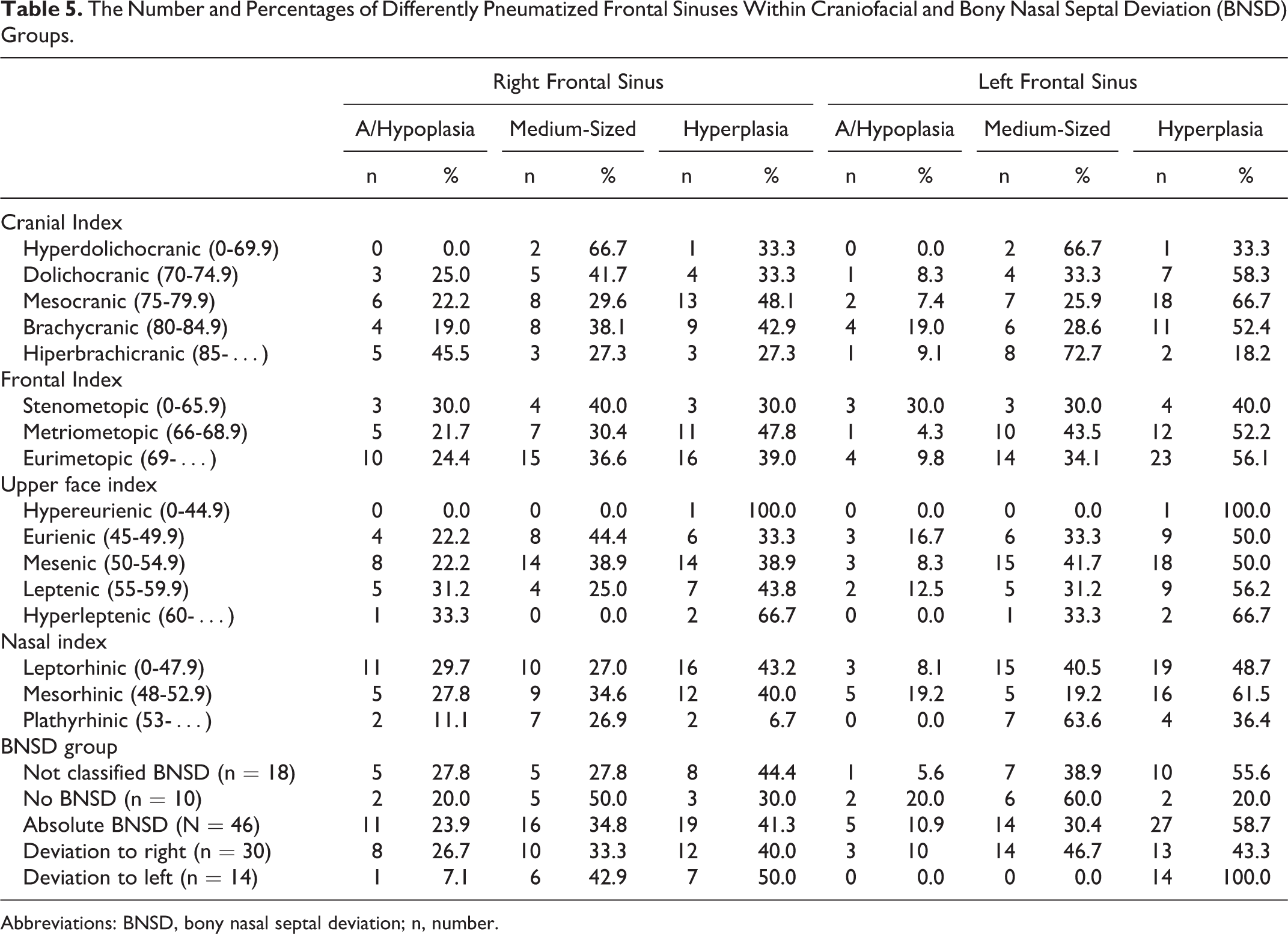
Abbreviations: BNSD, bony nasal septal deviation; n, number.
The Analytic Findings of Linear Regression of Mean Frontal Sinus Morphometric Measurements (FSW, FSH, FSD in “mm” and FSV in “mm3”) With Craniofacial and Bony Nasal Septal Deviation (BNSD) Groups.
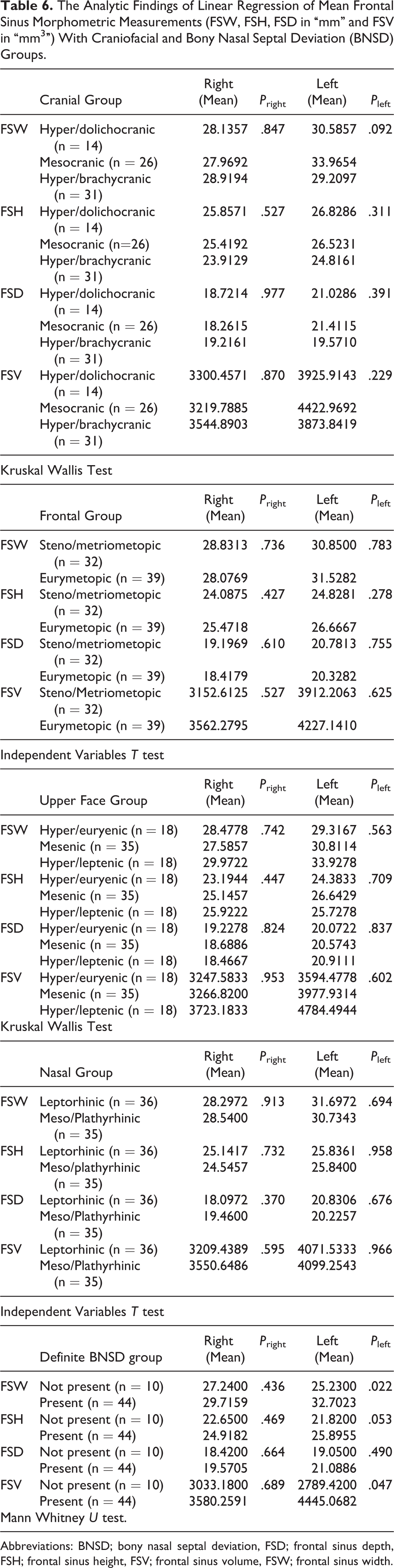
Abbreviations: BNSD; bony nasal septal deviation, FSD; frontal sinus depth, FSH; frontal sinus height, FSV; frontal sinus volume, FSW; frontal sinus width.
Although we observed greater morphological measurements for the bilateral sinuses of the skulls with BNSD, only the left-side FSW and FSV measurements were found to be significantly greater in deviated skulls compared to skulls without BNSD (P < .05). Two of the 46 skulls with BNSD showed FS aplasia (4.3%), and the remaining 44 skulls were compared with respect to the FS morphometric measurements between the deviation side and the opposite side. In 30 skulls, the BNSD was toward the right side, whereas the other 14 skulls showed BNSD toward left side. Frontal sinus morphology did not differ between the deviation side and opposite side according to paired t test (P > .05), and correlation analysis showed that the morphometric measurements were similar and positively related to both sides (P < .05).
Assessing potential differences in FS morphology with the presence of metopic suture as a craniofacial structure characteristic, metopic sutures (Figure 3) were observed in 5 of the 74 skulls (Table 7). Frontal sinus morphometric measurements and craniometric measurements were compared for the 5 skulls with metopic suture versus the other 69 skulls. Among the craniometric measurements, maximum head width and minimum and maximum frontal width measurements were observed to be greater in those with metopic suture than those without (n = 5 for the metopic suture group; statistical analysis was not applicable), whereas no differences were found with the other craniometric variables and FS morphometry measurements.

Cranium with metopic suture (arrow).
The Classification of Craniofacial and Frontal Sinus Morphology of the Skulls With Persistent Metopic Suture.
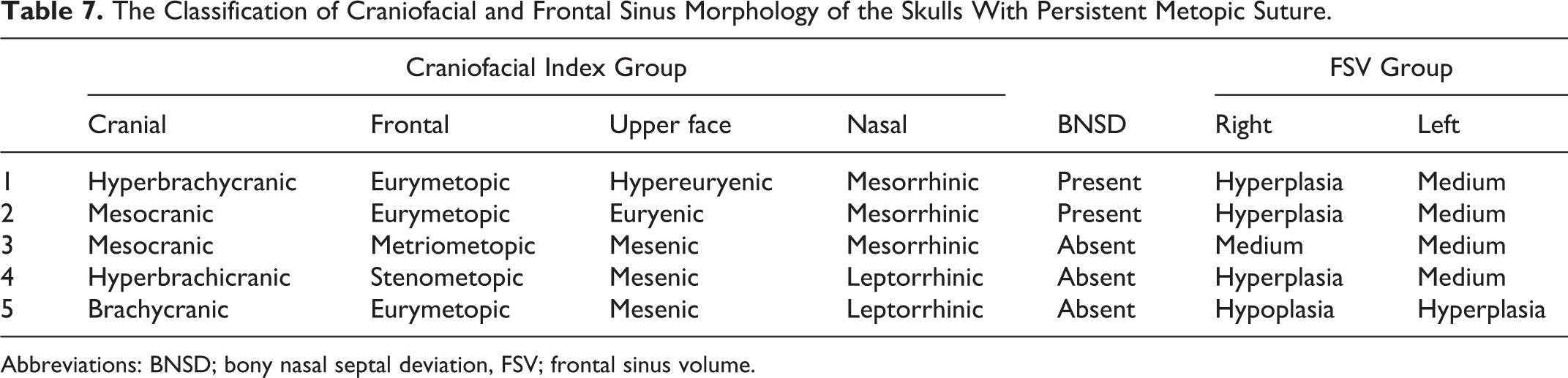
Abbreviations: BNSD; bony nasal septal deviation, FSV; frontal sinus volume.
As summarized in Table 8, there were no significant differences in FSVAR values among the cranial subgroups, frontal subgroups, upper facial subgroups, and nasal subgroups (P > .05). However, when the data in Table 8 were analyzed numerically, the ratio of right–left asymmetry was found to change in favor of the right sinus without altering the asymmetry direction in the skulls with wide/very wide head structure (hyper/brachycranic), narrow/very narrow upper face structure (hyper/euryenic), and the skulls without BNSD. The FSVAR values for the skulls with metopic suture were also not significantly different from the others (P = .141).
The Analytic Differences of Frontal Sinus Volume Asymmetry Ratios Between the Craniofacial and Bony Nasal Septal Deviation (BNSD) Groups.
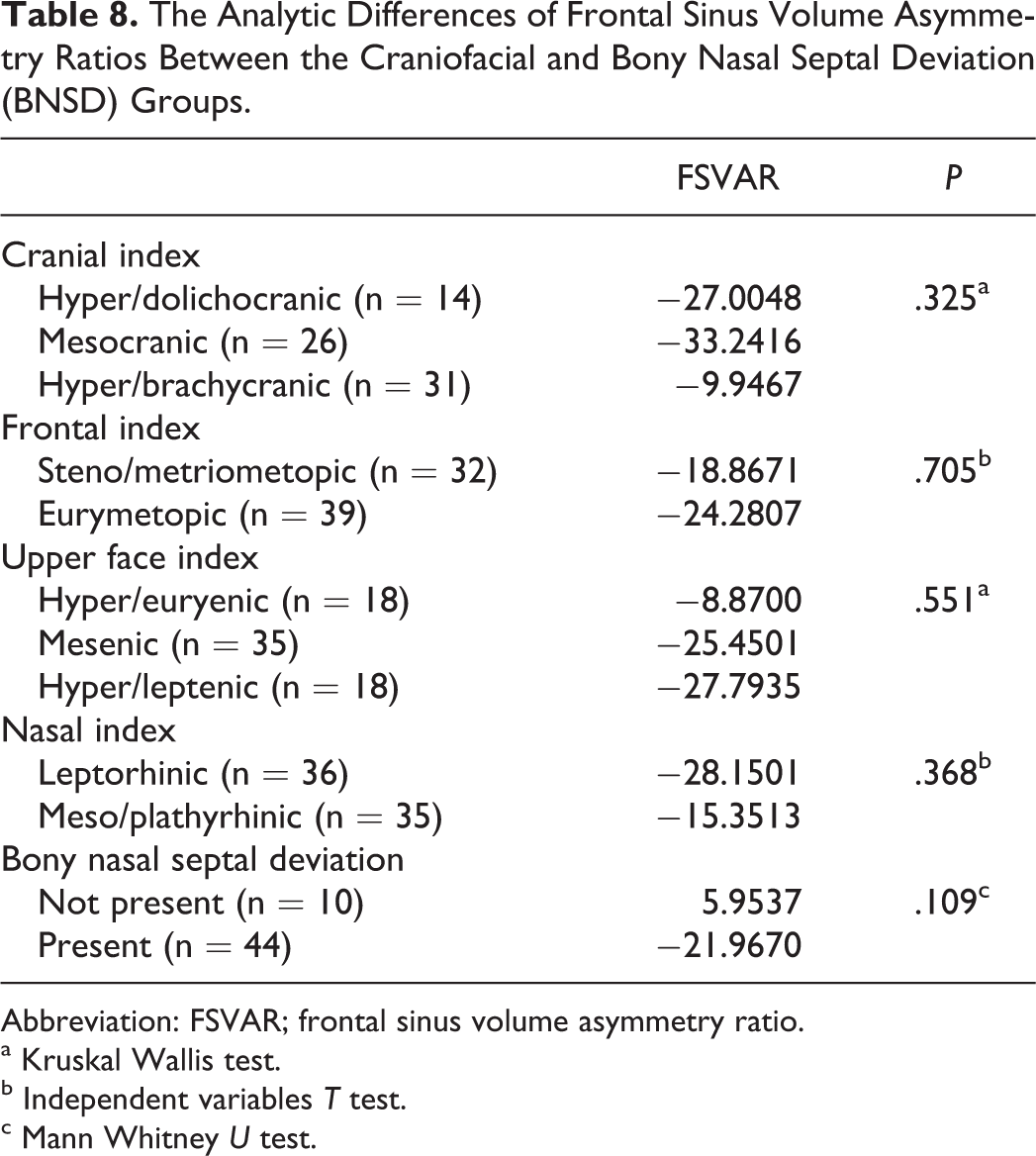
Abbreviation: FSVAR; frontal sinus volume asymmetry ratio.
a Kruskal Wallis test.
b Independent variables T test.
c Mann Whitney U test.
The asymmetry analysis showed that the morphometric FS measurements at the opposite side of the intersinus septum deviation (especially in the case of deviation toward the right) were greater than the measurements at the deviation side (P < .05). With intersinus septum deviation toward the right side, FSVAR showed significant asymmetry in favor of the side opposite to the deviation as detected in the measurements (P < .001). However, with intersinus septum deviation toward the left, the mean FSVAR remained in a positive direction. The association between the presence of intersinus septum and BNSD was not statistically significant. Six of the 10 skulls without definite BNSD also lacked intersinus septal deviation. None of the 14 skulls with left-sided BNSD showed left-sided intersinus septal deviation (n = 5 for right-sided, n = 9 for no intersinus septal deviation). The percentages of right-sided, left-sided, and absence of intersinus septum deviation in the 30 skulls with right-sided BNSD were 23.3% (n = 7), 33.3% (n = 10), and 43.3% (n = 13), respectively.
Discussion
Considering the multifactorial developmental effects of the FS, the current study assessed relationships between craniofacial morphology and FS dimensions in an Aegean population. The results suggest that FS morphology is related to facial and cranial structures at some points, especially the nasal structure, which links the anterior–posterior cranial base and the midface. In particular, developmental relations of FSs are important for surgical purposes as well as for anatomy, anthropometry, and ontogeny. The second area also connects with geographic and demographic characteristics of FSs for anthropologists. 26,27
Attempts to link different aspects of FS morphology with specific influences other than environmental factors, such as craniofacial development, have been inconclusive. In this study, we analyzed potential independent variables related to craniofacial structure that could affect fontal sinus morphology according to univariate and multivariate linear regression analysis, which is a superior method compared to other statistical tests used in the literature.
Statistical analysis showed that left-side sinus measurements correlated with the “maximum head length” and “nasal height” variables. Maximum head length and nasal height showed a linear relationship with FSW, FSV, FSD, and FSV on the left side; whereas only FSV showed this correlation in the right-side measurements. Potential reasons for the differences in left side measurements are suggested by the fact that the left-sided volumetric measurements were larger than those of the right side. When assessing why these 2 craniometric variables did not affect FS morphology to a statistically significant level on the right side, we observed that increases in maximum head length and nasal height were also associated with increases in sinus length and volume measurements on the right side, but the correlations did not reach statistical significance. However, the use of the 2 variables together was found to be a weak model for predicting sinus volume. “Maximum head length” together with “nasal height” was found to have no significant effect on FSV separately from the other independent variables (P > .05).
In contrast, nasal height was correlated with both right and left sinus volumes in the univariate and multivariate linear regression analysis. Filho et al also found a relationship between nasal pyriform aperture area and left FSV (r = 0.435, P = .011) and reported that the degree of nasal cavity aeration affects FS development. 10 In this study, there appears to be a positive linear relationship between nasal height and frontal morphometry. In addition, the effect of nasal height is more apparent than maximum skull length for most of the analyses.
Previous studies have suggested that FSs are larger in brachiocephalic heads than dolichocephalic heads. 10 Filho et al found a relationship of spin bregmatic distance and glabella-lambda curvature with left FSV (r = 0.450, P = .009 and r = 0.433, P = .012, respectively). 10 In another report by Tehranchi et al, a recent study that utilized a weak methodology, they showed a correlation between FS dimensions and anterior facial height in males and increased gonial angle in females. 28 However, no significant relationship was detected among the craniometric groups with respect to FS morphology in the present study, which used a stronger methodology along with appropriate data analyses compared to the above 2 reports.
The well-known work of Stammberger and Kennedy 9 defined FS development as a continuation of frontal recess. Accordingly, the previous study of this research group suggested a relationship of frontal recess and the ostium with FS morphology. 29 Together with the associations gathered from this study, the data clearly show that nasal structure has a unique influence on FS morphology.
In the 44 skulls with BNSD, morphometric measurements of the FSs at the deviation side and the opposite side did not differ statistically. In the correlation analysis, morphometric measurements at the deviation side and opposite side were detected to be similar and linearly related to each other (P < .05). In the study of Hafezi et al, individuals with nasal asymmetry showed retarded orbital and face development on the side where the nose was concavity. 30 In the present study, no similar data were generated for FS development with respect to BNSD, such as whether the FS grows less on the deviation side. However, in the presence of BNSD, asymmetry rates are greater and negative (FSVAR = −21.97) compared to the nondeviation group. Although this difference was not statistically significant, the observed negative asymmetry rates indicate that the FS measurements taken at the deviation side are smaller than those of the counterparts when considering the formula calculating these rates.
No studies investigating the developmental association between nasal structure and FS structure were found in the literature. In the present study, the relationship between bony nasoseptal and FS morphometry was also investigated. There was a linear relationship between the presence of BNSD and FSW and volume measurements. In the presence of a deviation, this relationship did not differ between the deviation side and the opposite side.
In addition to craniofacial index and BNSD groups, when the relationship between the presence of metopic suture and FS morphology was analyzed, the hypothesis that sinus aplasia or hypoplasia developed in the presence of metopic suture was refuted. It has been suggested that the data supporting a relationship between metopic suture and FS aplasia or hypoplasia may be incidental. Among the 74 skulls in the study, metopic sutures were found in 5 (6.8%). When the FS morphology and asymmetry measurements were compared between the skulls with and without metopic suture, no significant difference was observed. In the study of Bilgin et al, among 631 patients, FS aplasia was found in 22.7% and metopic suture was found in 9.7%; importantly, no relationship was found between these 2 states. 31 However, other studies have also suggested an increase in FS aplasia frequency in the presence of persistent metopic suture. 16 -19,32
Pirner et al showed asymmetry between the right and left FSs in 3-dimensional models. 33 Yoshino et al suggested that the degree of FS asymmetry differs among different ancestors, which also indicates variation in craniofacial morphology. The present study is the first to examine the extent of the asymmetry between right and left FSs with respect to craniofacial structure. In this study, FSVAR was higher in skulls with narrow medium-sized heads, wide frontal and upper faces and narrow noses. This finding is in concordance with a report by Lang showing that dolichocephalic heads more commonly have asymmetric FSs. 34 Given the embryologically independent development of the right and left FSs even in monozygotic twins, 35 a statistically significant difference between the right and left FS morphometry measurements of the same skull was considered an expected result in the previous study. 29 It has also been reported that the intersinus septum separating the right and left FSs generally deviates to one side. 1 In this study, intersinus septum was found to deviate toward the right in 23% and toward the left in 18% of the skulls, and there was a nonsignificant relationship with BNSD in the negative direction. Statistical analysis of the FS asymmetry ratios has proven these facts, and the usage of the FS for identifying individuals continues to gain prominence.
The FS development is dynamic. They begin to develop during the second year of life, and they can be detected radiographically after the age of 5 years. 13 Although it is generally accepted that FSs approximately complete their development by the age of 20 years, Tatlisumak et al proposed that FSs show their largest morphometric values between the age of 31 and 50 years in both genders. 20 A recent study from the same group reported that FS size in females increased with age, whereas FS size in males decreased after the age of 50 years. 36 Regardless of age and gender, we found that FS morphology does not progress in the same direction as craniofacial structure development.
Decades of studies have investigated FS morphometrics in several respects, such as individuality studies 4 and even the complexity of FS mathematics. 7 The common ground and the greatest challenge of FS morphometric studies is that a normal distribution cannot be obtained for most data sets. 7 As an anatomical structure at the intersection of many subsciences due to its proximity to the cranial base, orbita, and maxilla, it is very important to understand the morphology of the FS according to cladistic and phylogenetic constructions and to recognize its importance in evidence-based developmental science.
However, it is important to take certain measures when analyzing the radiologic features of FS structure, as specific environmental factors such as sport activities, trauma, sinonasal, or certain systemic diseases may cause postmortem changes that alter FS morphology. Another limitation of this study was its lack of sex assessment of the dry skulls. However, previous studies have clearly shown that there is no significant differences in average FS size between the sexes, as the FS itself has a unique morphology specific to each individual. 13,37 The other limitation of this study was the indeterminate situation of the dental structures and the upper and the lower jaw, which is outside the scope of this study and is a topic of future research.
As an unfortunate situation, surgeons sometimes enter the cranium through the FS and being aware of asymmetric FS is crucial to minimize the surgical complications. During FS surgeries, especially for the patients who have asymmetrical skull base angulation and FS and have narrow or medium width head and/or upper face structure and/or nasal septum deviation; because of the high frequency of anatomic variations and their close proximity to vital organs such as the orbita and anterior skull base; anatomical knowledge, preoperative evaluation of the CT scans, and surgical experience of the surgeon are very important. There is a need for further studies in various populations that will provide the basis for determining methods and equipment for navigation technology and robotic surgeries to be used for FS surgeries in the future.
The findings of this study will direct discussions on the relationship between FS structure and craniofacial elements, which has not yet been evaluated due to the different conclusions generated from previous reports. These will facilitate improved understanding of FS-related physiological associations through the expansion of anatomical and anthropometric knowledge.
Conclusion
In conclusion, the presence of metopic suture and cranial structure characteristics do not show a linear relationship with FS morphology, but “nasal structure” does. Frontal sinus and nasal morphology are both unique to each individual, and future studies will provide stronger evidence indicating the FS and the nasal structure are well associated.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dokuz Eylul, University Radiology Department Research Group, financially supported this thesis project.