
Abstract
Objective:
To investigate the indications, efficacy, safety, and outcomes of potassium-titanyl-phosphate (KTP) laser procedures for treatment of laryngeal disease.
Methods:
PubMed, Cochrane Library, and Scopus were searched for studies providing information about the indications, efficacy, and safety of both in-office and operative suspension microlaryngoscopy KTP laser procedure in treatment of laryngeal disease. Diagnostic criteria and clinical outcome evaluation of included studies were analyzed using Preferred Reporting Items for Systematic Reviews and Meta-Analyses criteria.
Results:
Of the initial screened 140 papers, 17 met our inclusion criteria. Six papers involved KTP laser procedures for benign and malignant vocal fold lesions in suspension microlaryngoscopy only, 10 papers focused on only in-office KTP laser procedures for benign vocal fold lesions, and 1 paper included both in-office and suspension microlaryngoscopy procedures. The following lesions may be considered as indications for KTP laser procedures: Reinke’s edema, sulcus vocalis, vocal fold hemorrhage, polyp, granuloma, cyst, scar, papillomatosis, dysplasia, leukoplakia, and early vocal fold malignancies. Irrespective of the types of procedure (in-office vs suspension microlaryngoscopy), the KTP laser is associated with a low complication rate and overall good vocal fold vibration recovery. There is an important heterogeneity among studies concerning laser settings, indications, and outcomes used for the assessment of treatment effectiveness. There are no controlled studies directly comparing KTP laser with other lasers (ie, carbon dioxide laser).
Conclusion:
The use of KTP laser procedures for treatment of laryngeal disease has increased over the past decade, especially for office-based management of vocal fold lesions. Future controlled studies are needed to compare the safety and outcomes of the KTP laser to other techniques.
Introduction
The 532-nm pulsed potassium titanyl phosphate (KTP) laser is a photoangiolytic laser widely used for urologic and dermatologic indications, and since its introduction in 2006, it has been increasingly used for laryngeal surgery as well. 1 The 532-nm wavelength of the KTP laser is selectively absorbed by hemoglobin so that coagulation of the sublesional microcirculation with less thermal damage to the surrounding tissue is possible. This selectivity in laser energy absorption can create less vocal fold damage and scarring when compared to other lasers commonly used in laryngeal surgery. For example, the pulsed KTP laser slowly heats intravascular blood, which is associated with a reduced risk of the photothermal injury and vessel wall rupture. 2 Over the past decade, the use of KTP laser has increased, especially for in-office laryngeal procedures, allowing treatment of many lesions of the vocal folds, for example, papillomatosis, 1 polyp, 3 ectasia, 4 cyst, 5,6 pseudocyst, 5 scar, 5,6 granuloma, 5,6 Reinke’s edema, 7 and leukoplakia/dysplasia. 8 In the same way, KTP laser is used in suspension laryngoscopy for the same diseases as well as for early vocal fold squamous cell carcinoma. 9
Currently, there is no updated systematic review summarizing the indications and outcomes of both in-office and suspension microlaryngoscopy KTP laser procedures. The aim of this systematic review is to investigate the current literature about indications, efficacy, safety, and voice outcomes of KTP laser procedures.
Materials and Methods
The population, intervention, comparison, and outcome framework 10 was used for considering studies for the systematic review.
Types of Studies
Prospective and retrospective studies published in peer-reviewed journals have been included in the review if they explored the effectiveness, safety, and outcomes of KTP laser procedure in vocal fold surgery. The surgical procedure had to be in-office (local anesthesia) or suspension microlaryngoscopy (under general anesthesia). We included studies published in either English or French.
Participants and Inclusion/Exclusion Criteria
Papers were included for analysis if they clearly described the types of laryngeal lesions treated by KTP laser procedure and the methods for lesion diagnosis. Included studies established diagnosis of vocal fold lesions through videolaryngostroboscopy or histological examination after treatment. The patients had to be treated with KTP laser. Composite studies investigating KTP and other (pulsed dye laser [PDL]) lasers were also considered.
Outcomes
The first study outcome was review of effectiveness of KTP laser therapy, including the feasibility of the procedure for the underlying lesion. The second study outcome was review of potential postoperative complications. The third study outcome was evaluation of voice quality from pre- to postprocedure, for example, use of patient-reported outcome questionnaires, perceptual subjective voice scale, aerodynamic, or acoustic measurements. Heterogeneity among included articles in patient lesions, laser settings, and outcomes measures limited ability to combine data statistically into a formal meta-analysis, limiting analysis of the current systematic review to qualitative rather than quantitative summary of the available information.
Intervention and Comparison
The procedure using KTP laser had to be described. For each study, the laser setting characteristics were extracted. Two types of comparisons were included: the pre- to postoperative comparison of voice outcomes and, in case of controlled study, the postoperative outcome result comparison between 2 groups of patients.
Search Strategy
A PubMed, Cochrane, and Scopus search were conducted by the authors for identifying studies about the effectiveness of KTP laser procedure for benign and malignant laryngeal lesions. The following key words were used: “KTP”; “laser”; “surgery”; “lesion”; “vocal”; “laryngeal”; “larynx”; and “voice.” The authors determined final article selection and provided a critical analysis of the publication’s content. The data of studies are summarized in the present publication. The review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses checklist for systematic reviews. 11
Epidemiological Characteristics and Outcomes
The investigators analyzed the following characteristics of studies: number of patients, study design, inclusion and exclusion criteria, quality of study, evidence level, and outcomes used for the assessment of the surgery/treatment effectiveness. The risk of bias was assessed with the Tool to Assess Risk of Bias in Cohort Studies developed by the Clarity Group and Evidence Partners. 12
Results
Initial screening identified 140 papers. From these papers, 17 met our inclusion criteria and were kept for analysis: 6 papers focused on KTP laser procedures during suspension microlaryngoscopy (Table 1), 3,4,13 -16 10 papers focused on in-office KTP laser procedures (Table 2), 1,5 -8,17 -22 and 1 paper included both in-office and in-suspension KTP laser procedures and is presented in both tables. 7
Research Studies on Suspension Laryngoscopy KTP Laser Procedures.
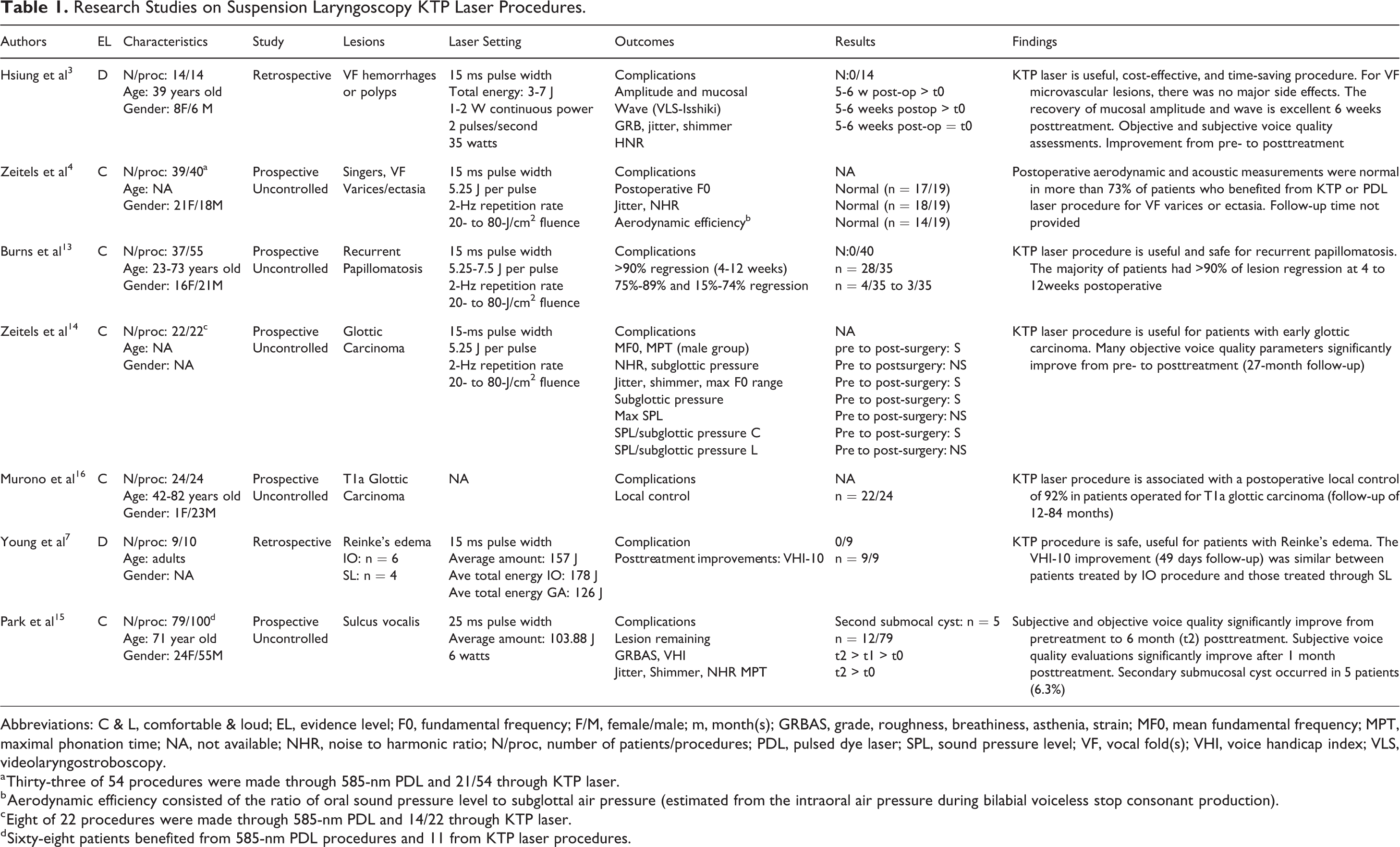
Abbreviations: C & L, comfortable & loud; EL, evidence level; F0, fundamental frequency; F/M, female/male; m, month(s); GRBAS, grade, roughness, breathiness, asthenia, strain; MF0, mean fundamental frequency; MPT, maximal phonation time; NA, not available; NHR, noise to harmonic ratio; N/proc, number of patients/procedures; PDL, pulsed dye laser; SPL, sound pressure level; VF, vocal fold(s); VHI, voice handicap index; VLS, videolaryngostroboscopy.
a Thirty-three of 54 procedures were made through 585-nm PDL and 21/54 through KTP laser.
b Aerodynamic efficiency consisted of the ratio of oral sound pressure level to subglottal air pressure (estimated from the intraoral air pressure during bilabial voiceless stop consonant production).
c Eight of 22 procedures were made through 585-nm PDL and 14/22 through KTP laser.
d Sixty-eight patients benefited from 585-nm PDL procedures and 11 from KTP laser procedures.
Research Studies on In-Office KTP Laser Procedures.
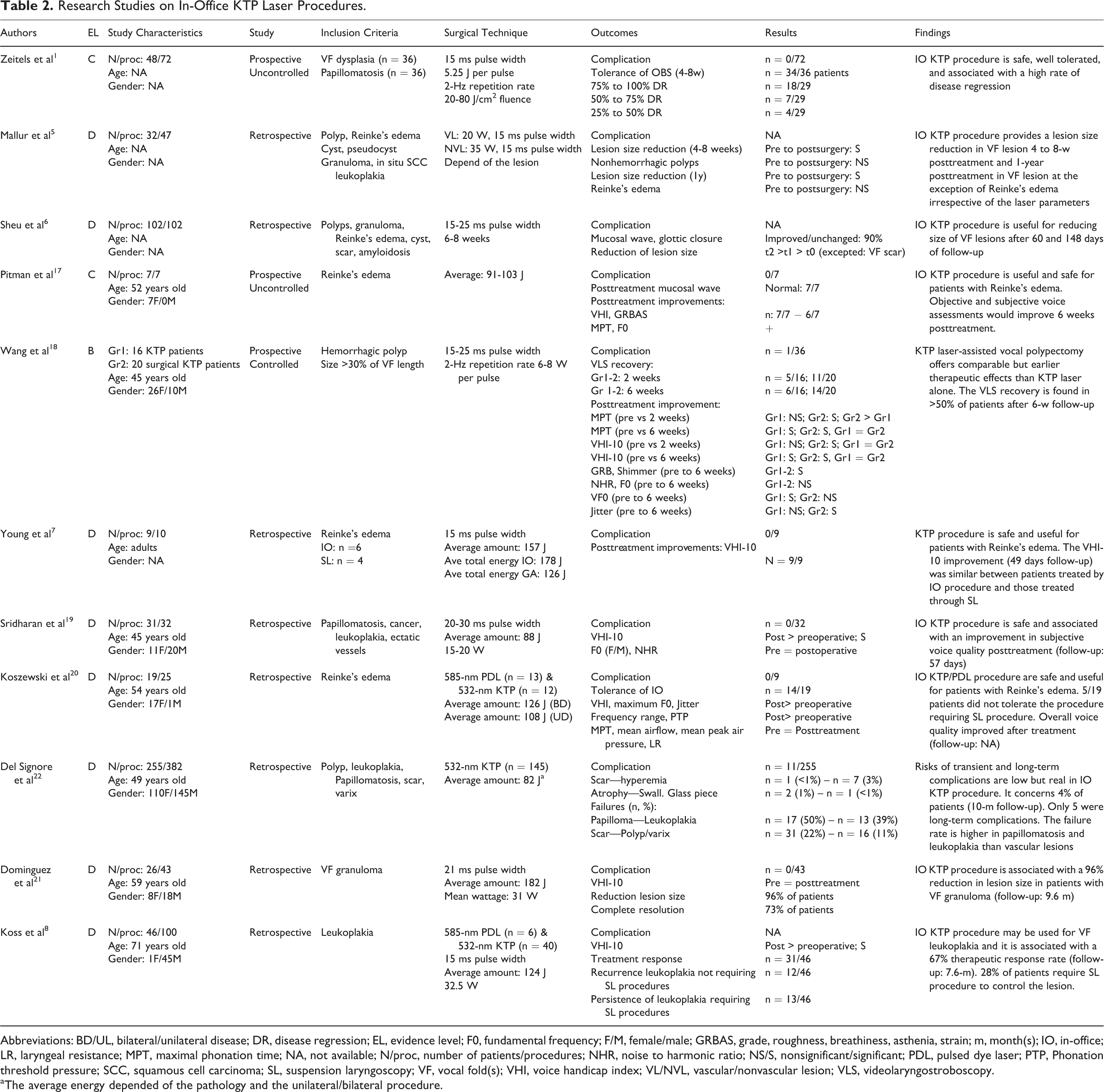
Abbreviations: BD/UL, bilateral/unilateral disease; DR, disease regression; EL, evidence level; F0, fundamental frequency; F/M, female/male; GRBAS, grade, roughness, breathiness, asthenia, strain; m, month(s); IO, in-office; LR, laryngeal resistance; MPT, maximal phonation time; NA, not available; N/proc, number of patients/procedures; NHR, noise to harmonic ratio; NS/S, nonsignificant/significant; PDL, pulsed dye laser; PTP, Phonation threshold pressure; SCC, squamous cell carcinoma; SL, suspension laryngoscopy; VF, vocal fold(s); VHI, voice handicap index; VL/NVL, vascular/nonvascular lesion; VLS, videolaryngostroboscopy.
a The average energy depended of the pathology and the unilateral/bilateral procedure.
Vascular Lesions (Varix, Ectasia, and Polyps)
Because the KTP laser is a photoangiolytic laser acting on the sublesional microcirculation, treatment of vascular lesions was among the first KTP laser procedures reported. In 2003, Hsiung et al used suspension microlaryngoscopy with KTP laser for vocal fold hemorrhages or polyps in 14 patients. 3 The authors reported significant improvements in mucosal wave at the videolaryngostroboscopy (VLS; Isshiki assessment), perceptual grade of dysphonia, roughness, breathiness, and acoustic measurements (jitter and shimmer). There were no complications among the 14 procedures. In 2006, Zeitels et al prospectively treated 39 singers with KTP laser in the operating room via suspension microlaryngoscopy 4 and reported normalized postoperative F0, jitter, and noise-to-harmonic ratio (NHR) parameters in 89%, 95%, and 95% of patients, respectively. Fourteen (74%) singers had postoperative normalized aerodynamic efficiency, which was defined as the ratio of oral sound pressure level to subglottal air pressure. Wang et al compared the use of in-office KTP laser procedures for treatment of hemorrhagic polyp versus the use of operative in-office KTP laser-assisted vocal polypectomy via microlaryngoscopy in a cohort of 36 patients. 18 These authors reported that the use of KTP laser-assisted vocal polypectomy in the operating room offered comparable and earlier therapeutic effects than office-based KTP laser alone. Specifically, the KTP laser-assisted vocal polypectomy was characterized by improvements in maximum phonation time (MPT), voice handicap index-10 (VHI-10), grade of dysphonia, roughness, breathiness, shimmer, and jitter at a 6-week time point. The procedure was safe and characterized by a 3% complication rate (n = 1/36) consisting of vessel rupture and hemorrhage during the in-office procedure. 18 The other studies that have included vascular polyps or ectasias report similar findings of low complication rate and significant improvement in postoperative voice quality outcome assessments. 5,6,19
Leukoplakia and Dysplasia
Leukoplakia has been studied by Koss et al on 46 patients (40 treated through KTP laser and 6 with PDL). 8 These authors have investigated the local recurrence of leukoplakia and the need for suspension microlaryngoscopy procedure for controlling the disease. Overall, in-office KTP laser procedure provided a local control rate of 72%. In this study, 13 patients required suspension microlaryngoscopy KTP laser procedures for persistent leukoplakia not controlled through in-office procedures alone. In a retrospective chart review of 255 patients and 382 procedures, Del Signore et al reported a 39% failure rate (lack of resection of the entire lesion) of in-office KTP laser procedure for leukoplakia (n = 13/33 patients), being the second most difficult lesion to control through in-office procedures alone after papillomatosis. 22 To date, this study is the most comprehensive, which looks at factors that predict ability to control dysplasia or papilloma in the office alone when compared to need for suspension microlaryngoscopy KTP laser procedures. Regarding voice quality outcome, VHI-10 significantly improved 7.6 months posttreatment. These authors did not specify the occurrence of complications. Leukoplakia is reported in other studies which include it among a variety of different pathologies. 5,19,22 Overall, the authors did not report significant postoperative complications associated with the treatment of leukoplakia, 5,19 and outcomes overall seem to be a sufficient posttreatment reduction in lesion size reduction 5 and improved posttreatment voice quality outcomes. 19 Similarly, Zeitels et al reported that the use of in-office KTP procedure for vocal fold dysplasia is safe (no complications) and associated with a high rate of disease regression. 1
Reinke’s Edema
Three studies focused on in-office KTP laser procedure for Reinke’s edema, all of them considering both unilateral and bilateral procedures. 7,17,20 Koszewski et al retrospectively studied the tolerance and complication rates of 9 patients who benefited from in-office KTP or PDL procedures for Reinke’s edema. 20 Five (55%) patients did not tolerate the procedure, requiring suspension microlaryngoscopy procedures. There were no postoperative complications. Some subjective (VHI) and objective (maximum F0, frequency range, jitter) voice quality assessments indicated substantially improved voice quality after treatment, but the low number of patients and even lower number of patients who tolerated office-based treatment limited the realization of consistent statistical analysis. The low complication rate (0%) and the improvement in subjective voice quality evaluation (VHI) have been corroborated in the case series of Young et al (10 patients, 49 days follow-up) and Pitman et al (7 patients, 6-week follow-up). 7,17 In addition, in the study of Pitman et al, the patients treated through in-office KTP laser procedures had an improvement in grade, roughness, breathiness, asthenia, strain (GRBAS) scale parameters, MPT, and F0. 17 However, as in Koss et al, the low number of patients in both Young et al and Pitman et al also limited definitive statistical analysis.
Potassium-Titanyl-Phosphate Laser in Papillomatosis
Laryngeal papillomatosis is defined by repeated local recurrence and need for repeated treatment recurrences, making the in-office procedure interesting as a means to help patients avoid repeated general anesthesia. Zeitels et al first reported on 36 in-office KTP laser procedures for laryngeal papillomatosis in 2006. 1 The authors reported high tolerance (94%), no complication, and the lesion size was estimated to have improved in 62% of patients. 1 In 2007, Burns et al reported the outcomes of 55 suspension microlaryngoscopy KTP laser procedures in 37 patients with recurrent papillomatosis. There were no complications, and 28 (80%) patients had more than 90% regression of the lesions 4 to 12 weeks after the surgery. 13 Even when the procedure is successful in reducing burden of papilloma, the nature of the disease is to recur, and further treatments will be necessary—emphasizing the potential cost savings of in-office treatment. 22 The low complication rate, good patient tolerance, and improvement in pre- to posttreatment voice quality all support use of the KTP laser for treatment of laryngeal papilloma, both in the office and in the operating room. 19
Cysts, Pseudocysts, Granulomas, Scars, and Sulcus Vocalis
Dominguez et al evaluated the utility and safety of in-office KTP laser procedure for vocal fold granulomas. Although the authors did not report on complication rate, treatment was successful—when KTP treatment was combined with anti-reflux treatment, 73% of patients had complete resolution of the granuloma(s) without recurrence at 9 months posttreatment. 21 Other authors studied the feasibility and safety of in-office KTP laser procedure for granuloma(s) among other lesions such as cysts, pseudocysts, and scars. Overall, they reported few complications, good tolerance, and satisfactory voice quality outcomes after various follow-up periods. 5,6,22 Only Park et al assessed the usefulness of KTP laser procedure in sulcus vocalis. These authors reported 5 complications (consisting of secondary submucosal cysts) on 79 patients and 100 procedures. The KTP laser procedure failed in 12 (15%) patients who had persistent sulcus postoperatively. Nevertheless, subjective (GRBAS and VHI), objective (jitter, shimmer, and NHR), and aerodynamic (MPT) measurements significantly improved from pretreatment to 6 months posttreatment measures. 15
Early Glottic Carcinoma
To date, 2 studies have investigated the postoperative oncological and voice quality outcomes in patients treated with KTP laser for T1a or T1b glottic carcinoma. In a prospective case series of 22 patients, Zeitels et al found a significant improvement in aerodynamic (MPT, subglottic pressure, ratio sound pressure level/subglottic pressure at comfortable pitch) and acoustic measurements (Mean F0, max F0 range, jitter, and shimmer) which were durable at 27 months posttreatment. 14 They did not specify the complication rate. The laser setting was similar to other studies of the Zeitels’ team (15-millisecond pulse width, 35 Watts, and 2-Hz repetition rate). Four years later, Murono et al conducted a prospective uncontrolled study on T1a glottic carcinoma analyzing the local control rate of a KTP laser approach. 16 They reported good local control (N = 22/24; 92%) 12 to 84 months after the surgery. No information was provided about the complication rate and the laser setting.
Epidemiological Analysis
The levels of evidence of the studies included in this review are low (Tables 1 and 2): 7 were uncontrolled prospective studies (level C evidence) 1,4,13 -17 and 9 were retrospective (level D evidence). 3,5 -8,19 -22 One study was controlled (level B) for the type of surgical procedure, but the authors did not compare the outcome of KTP laser with another laser. 18 For the suspension microlaryngoscopy KTP laser procedures, the diagnosis of excised lesions was confirmed through histopathological analyses 3,14,16 or was based on VLS examination. 4,13,15 For in-office KTP laser studies, histopathological analysis was less used, especially for Reinke’s edema 7,17,20 or recurrent papillomatosis. 1 Some authors using VLS did not specify if the diagnosis of benign lesions of the vocal folds was supported through postoperative histopathological analysis. 5,6,19
The laser setting was totally or partially specified in the majority of studies (Tables 1 and 2). One team did not specify laser settings. 16 As shown in Tables 1 and 2, some setting differences exist for the same diseases across studies, that is, particularly the case for Reinke’s edema. 7,17,20
Voice quality has been studied in 12 papers. The voice quality outcomes and the mean duration of follow-up for patients vary substantially across studies. The tools used for assessment of voice quality differed from 1 study to another (Table 3). The most used voice quality outcomes are VHI scales (n = 6), jitter (n = 6), NHR (n = 6), F0 measurements (n = 6), VLS (n = 4), maximum phonation time (n = 5), shimmer (n = 4); and GRBAS scale (n = 4).
Voice Quality Outcomes.
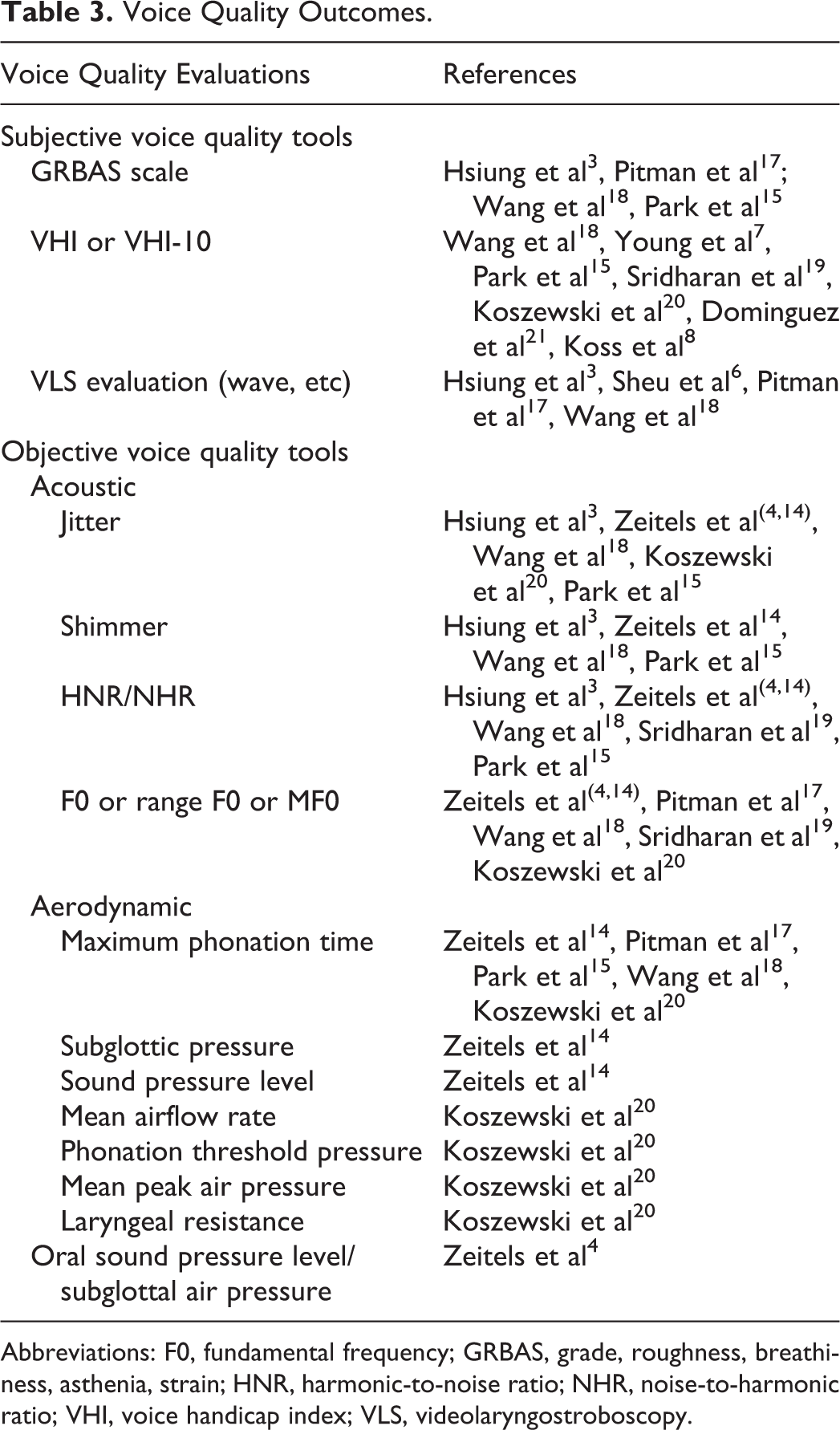
Abbreviations: F0, fundamental frequency; GRBAS, grade, roughness, breathiness, asthenia, strain; HNR, harmonic-to-noise ratio; NHR, noise-to-harmonic ratio; VHI, voice handicap index; VLS, videolaryngostroboscopy.
Discussion
The KTP laser was brought into laryngology with the potential for photoangiolytic, fiber-based laser treatment to offer in-office treatments in addition to use during suspension microlaryngoscopy, few postoperative complications, and good voice quality outcomes. The current review shows that over the past decade, increasing reports on use of KTP laser in the office and operating room for treatment of laryngeal disease show that the laser is meeting these expectations. Currently, it is being used for a number of indications, with favorable outcomes.
The main advantage of KTP laser is probably the possibility for using it for in-office laryngology, which is not possible with carbon dioxide (CO2) laser; office procedures offer cost savings and reduce morbidity for patients. Currently, the management of vocal fold benign lesions involves a global cost ranging from US$577 to US$953 per patient per year. 23,24 This cost implies speech therapy, medical treatment, and the points related to surgical procedure (general anesthesia, surgery, and hospitalization). The lack of general anesthesia, the safety, and the ease of scheduling in-office procedures are all cost-effective arguments for developing local procedures in laryngology. In-office KTP laser procedures may be proposed for selected patients with some benign lesions of the vocal folds, including unilateral or bilateral Reinke’s edema, cyst, pseudocyst, sulcus vocalis, ectasia, polyps, papillomatosis, dysplasia, leukoplakia, and granuloma. 5,8,14,17,19,21,22 For some of these processes, office treatment may be a 1-time occurrence; in others, such as leukoplakia and papilloma, the disease process itself is characterized by recurrence and need for repeated treatments—which makes potential office-based care all the more important. The use of in-office KTP laser procedure for invasive/malignant lesions is still controversial.
Second, the low postoperative complication rate is another important strength of the KTP laser procedure. The focus on the sublesional microcirculation, the fiber size (reducing the damage to the working channels of laryngoscopes), and laser pulse width are several points that underscore the low complication rate of the KTP laser compared to other approaches. 25 For instance, Zeitels et al reported that the wavelength of the KTP laser (532 nm) is well absorbed by hemoglobin, and the extended pulse width of the KTP laser when compared to the fixed 0.5-millisecond pulse width of the PDL allows for distribution of energy over a longer time period, resulting in more effective intravascular coagulation through slower intraluminal heating and avoiding vessel rupture and thermal injury to the superficial lamina propria. 1,4 Although an increasing number of studies report on KTP laser procedures, there is no controlled study that demonstrates the better safety of KTP laser over PDL or CO2 laser. Although both PDL and KTP lasers have been used in 3 studies, these authors did not directly compare the outcomes between the laser types. 1,8,20
Third, voice quality outcomes are favorable with the use of the KTP laser when reported. However, only 12 studies investigated pre- to posttreatment evolution of voice quality outcome(s), most of them being incomplete (patients lost to follow-up, incomplete data, and so on) or using 1 or 2 subjective evaluations without objective measurements or vice versa. With regard to objective measurements, the method used for measuring acoustic parameters was not or partly specified 19,17,20 or substantially differed from one to another paper (vowel, duration of phonation time, number of samples, and so on). 3,15,14,18 However, it has been shown that depending on the time interval over which the acoustic parameters are measured, the clinical effects of treatment may or may not be captured statistically. 26 Here, the follow-up time differs significantly from one study to another. The lack of controlled study comparing voice quality outcomes of patients according to the type of treatment (KTP vs PDL vs CO2 laser vs no laser) limits our ability to draw conclusions about which laser might offer best voice outcomes, and current data support good voice outcomes for KTP laser treatment in the absence of control groups. Any future studies that aim to compare one laser directly to another will have to consider many points. An ideal study would be prospective, well-controlled across different lasers and clear about indications for study enrollment relative to lesion type and lesion size. A variety of outcomes relative to complication rate, treatment effect, and voice quality would need to be considered, with both short- and long-term follow-up periods. Additionally, the methods used for the laser procedure (laser setting) and the measurement of acoustic parameters have to be specified for the reproducibility of the study. Finally, sample size would need to be adequate to draw meaningful conclusions. For these reasons, it might be that comparative studies of one laser type compared to another may remain lacking, and case series of a single laser’s results within a single disease state may provide the bulk of our existing literature for the time being.
Conclusion
Potassium-titanyl-phosphate laser procedures are safe and effective across a number of laryngeal pathologies, and the KTP laser can be used well for both in-office and suspension microlaryngoscopy approaches. The use of office-based treatment in particular, especially for disease states that might require repeated treatments, is very cost-effective. Direct comparison of KTP laser approaches to other surgical techniques remains lacking, and future controlled studies with clear inclusion criteria and well-defined clinical and voice quality outcomes are needed.
Footnotes
Authors' Note
Jerome R. Lechien is now affiliated with Department of Otolaryngology-Head Neck Surgery, Foch Hospital, UFR Simone Veil, University Versailles Saint-Quentin en Yvelines (University Paris Saclay), Paris, France.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.