
Abstract
We present the case of a 31-year-old woman with isolated symptomatology accusing positional vertigo. The videonystagmography (VNG) including Dix-Hallpike testing we have performed, highlighted atypical eye movements. We have observed a positional downbeating nystagmus with characteristics that could be accounted for anterior semicircular canal benign paroxysmal positional vertigo. Furthermore, examining the atypical nystagmus at the measurements performed during VNG recordings, we suspicioned a central positional vertigo. The abnormalities observed at the positional nystagmus were the lack of latency period, the downbeating component not limited in time, and the atypical torsional component. The magnetic resonance imaging examination recommended showed multiple white matter lesions characteristic for multiple sclerosis. The patient was referred to the neurology department for further evaluation and treatment. The diagnosis was unexpected because the patient did not have any other symptom that could have been linked to multiple sclerosis.
Introduction
Benign paroxysmal positional vertigo (BPPV) is the most frequent vestibular disorder. The disease is caused by dislodged otoconia from the utricular macula entering the semicircular canals. The posterior canal is involved in the disease in most of the cases. The gold standard for the diagnosis of posterior canal paroxysmal positional vertigo is the Dix-Hallpike maneuver that elicits a typical kind of nystagmus—torsional–upbeating. Downbeating nystagmus elicited by this maneuver is an indication for the anterior semicircular canal involvement. The anterior canal BPPV is extremely rare accounting for approximately 1% of the BPPV.
Central positional vertigo is a type of positional vertigo in which the otolithic displacement is not the cause of the disease. Different types of lesions in the central nervous system may produce positional vertigo without otolithic involvement. Demyelinating lesions in multiple sclerosis can be a cause for central positional vertigo.
Case Report
We present the case of a patient, a 31-year-old woman, who was referred to our department accusing positional vertigo, especially when adopting the supine position. She noticed the symptoms several months prior to the examination. The patient described short sensations of rotational vertigo triggered by head movements, without associated nausea, vomiting, or other neurovegetative manifestations.
The patient did not have any other symptom or any other medical history. She reported no disequilibrium, no audiologic symptoms, and no neurologic symptoms. The only other symptom she accused was the intense fatigue. The otorhinolaryngologic examination was within normal limits. The audiogram and the otoacoustic emissions were normal.
The vestibular examination we performed at presentation showed no spontaneous nystagmus, the Romberg and Fukuda tests were negative. In Figure 1, it is presented the recording of the videoinystagmography (VNG) examination of the spontaneous nystagmus, without fixation. There are not any abnormal movements noticeable on the graph, no spontaneous nystagmus.
The next step of the examination was the Dix-Hallpike test. The patient reported short sensations of vertigo with a duration of seconds in both Dix-Hallpike positions. In Figure 2, it is represented the ocular response at the Dix-Hallpike right position. The ocular movements were not as we expected. Instead of torsional nystagmus beating to the right and upward, the nystagmus we elicited was beating to the right ear and downward, without a latency period.
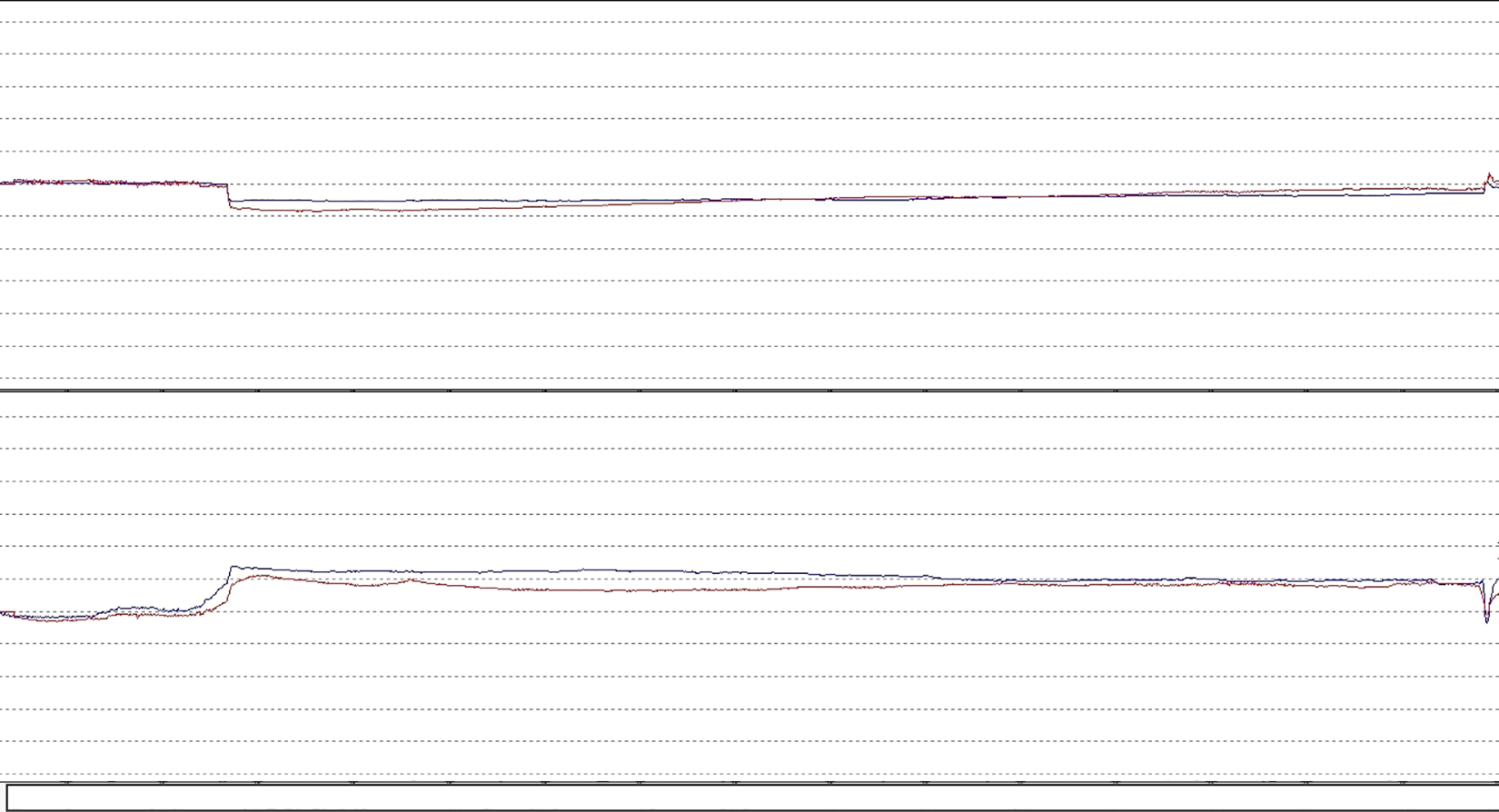
Videoinystagmography (VNG) graph: recording of the spontaneous nystagmus test.
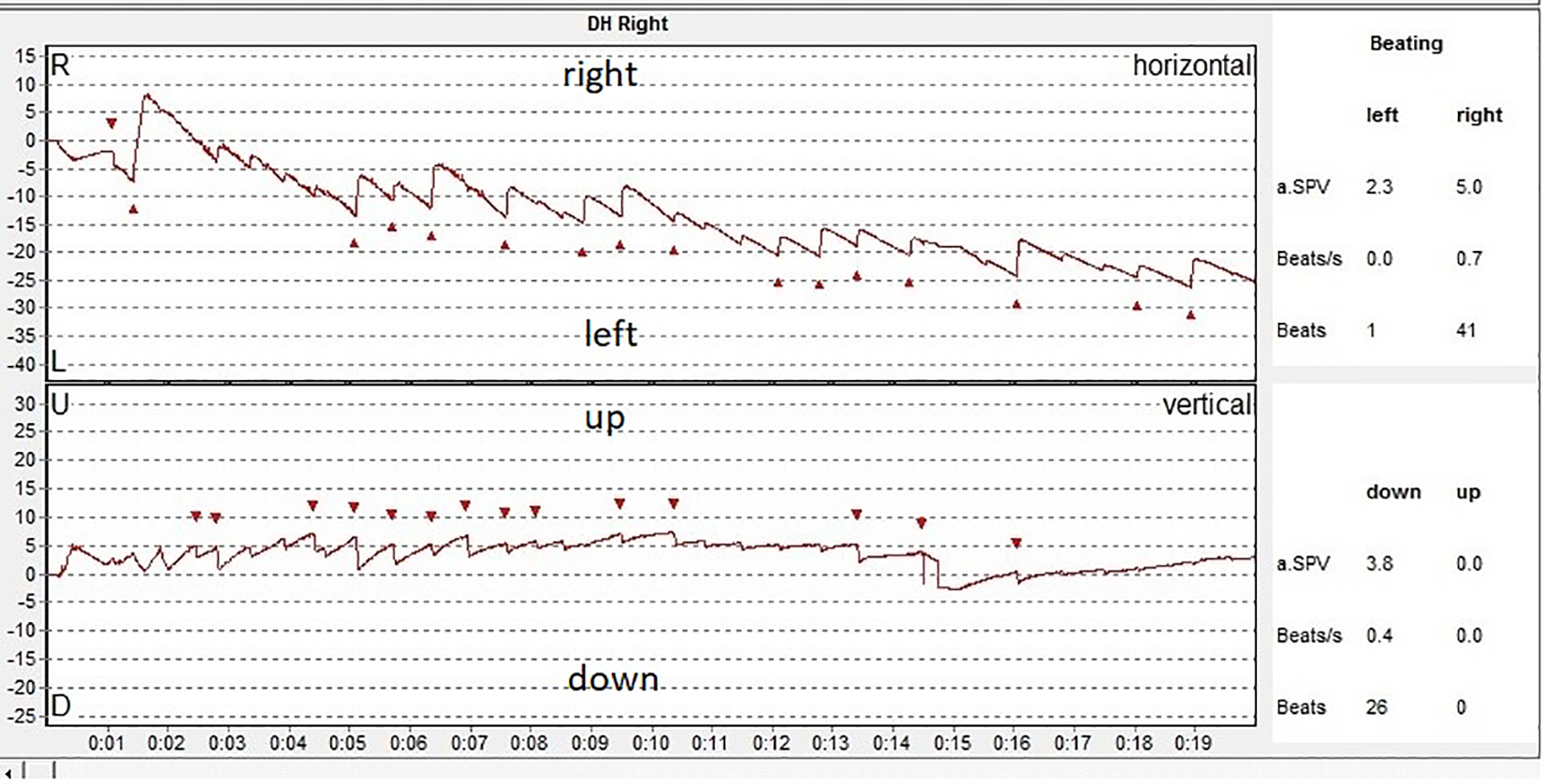
Videoinystagmography (VNG) graph: recording of the eye movements at the right Dix-Hallpike test.
The graph we obtained when testing the Dix-Hallpike left position is presented in Figure 3. In this case, we elicited a downward nystagmus with very few right beating components and latency period as well. The nystagmus we triggered did not have a limited time duration and continued for as long as the supine position was maintained although the sensation of vertigo was limited in time (few seconds). The right beating component was also atypical for the BPPV of a left posterior canal that could have been elicited in this position. The normal nystagmus expected in case of left posterior canal BPPV would have been upbeating torsional to the left ear.
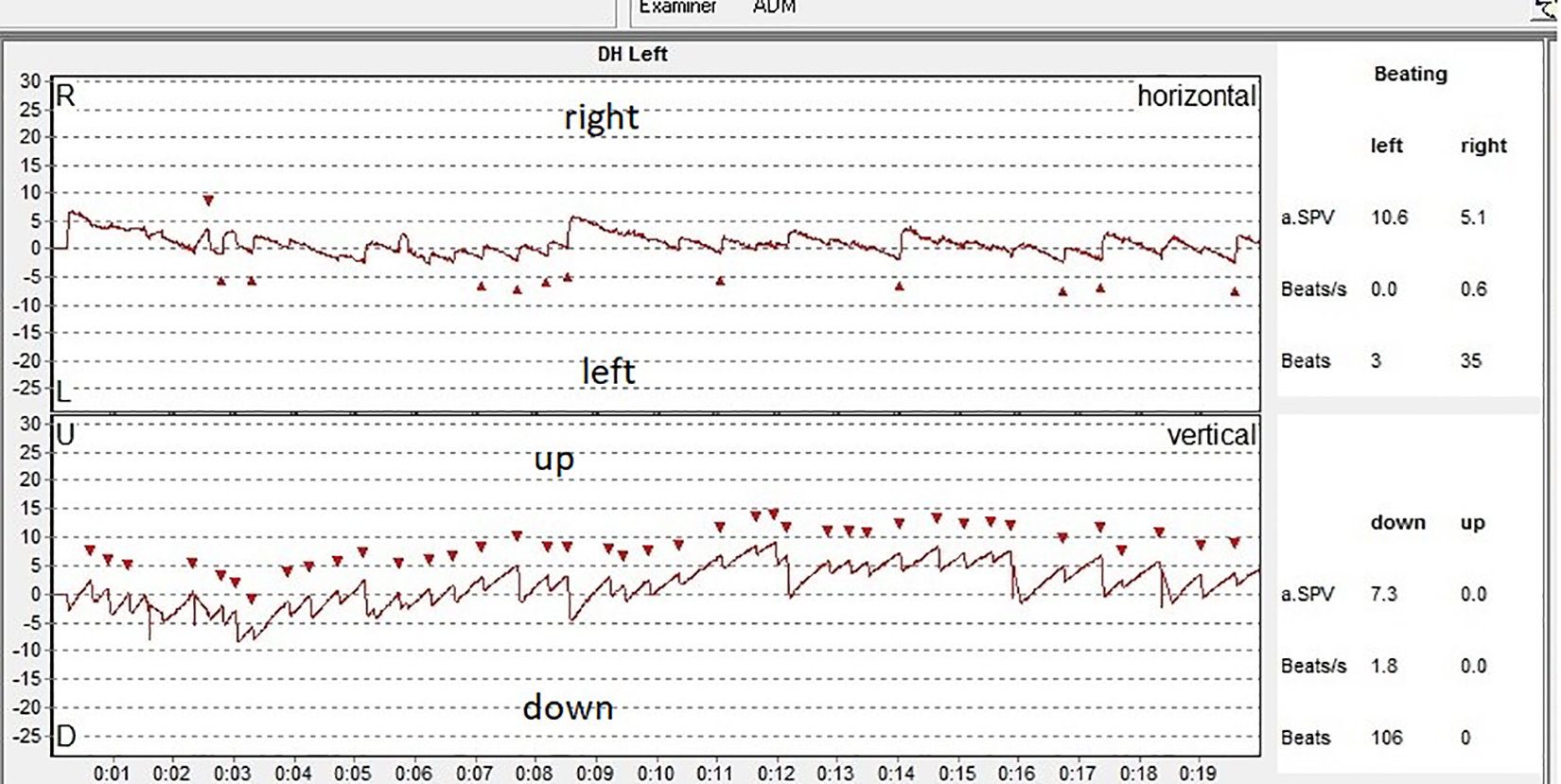
Videoinystagmography (VNG) graph: recording of the eye movements at the left Dix-Hallpike test.
At that point, our first suspicion was the fact that the patient had an anterior canal paroxysmal positional vertigo. In an anterior canal lithiasis, the expected eye movement at Dix-Hallpike would have been a downbeating with or without torsional movement. In case of torsional nystagmus, the torsional component beats clockwise for the left ear and contraclockwise for the right ear. The VNGgraph has limitations in reflecting the rotatory component of the nystagmus, but the video recordings performed illustrated a slight rotatory component of the nystagmus. We also performed a caloric test which proved to be within normal limits.
Although we tried to treat the patient using the “deep head-hanging maneuver,” we did not achieve any positive results as the symptoms persisted after the repositioning maneuver.
Considering the multiple abnormalities that we discovered at the Dix-Hallpike testing such as the lack of latency period, the abnormal downbeating not limited in time, the atypical torsional contraclockwise beating when adopting the left position, and the lack of response to the repositioning maneuvers, we decided to perform a magnetic resonance imaging (MRI) examination.
Figure 4 represents images of the cerebral MRI of the patient. The result, consisting of multiple demyelinating lesions in different stages of evolution which were observed, was unexpected especially considering that the disease seemed to be evolving for a long time and no other signs or symptoms were noticeable until the presentation, except may be for the fatigue. The patient was referred to the neurological department for evaluation and treatment.
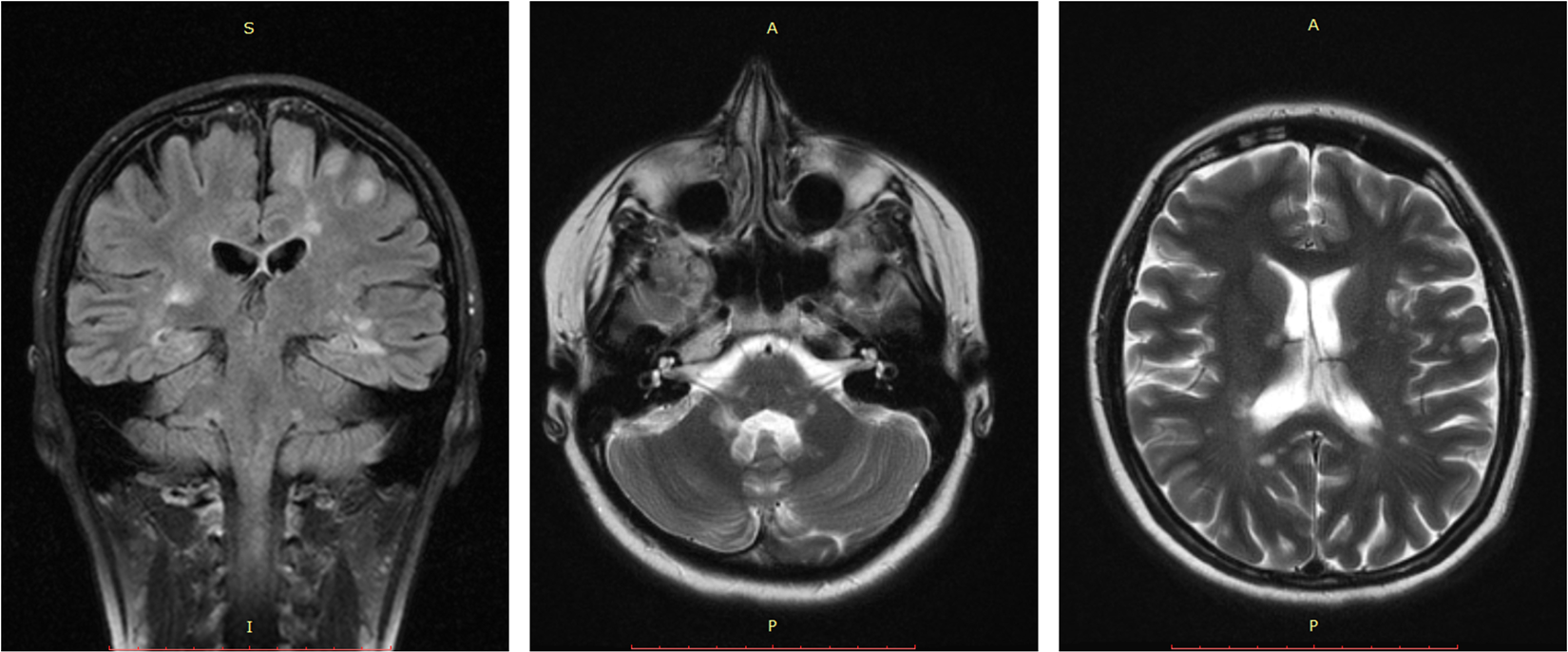
Magnetic resonance imaging (MRI) of the patient showing multiple white matter lesions with topography characteristic for multiple sclerosis.
Discussion
Multiple sclerosis is an autoimmune-mediated disease of the central nervous system characterized by the destruction of the myelin sheath of the neurons. 1 International statistics say that approximately 2.1 million people are affected by multiple sclerosis (MS) worldwide. The prevalence for the United States varies from 58 to 95 per 100 000 population. Multiple sclerosis is diagnosed usually in persons aged 15 to 45 and is more frequent in women. 2,3
The disease is diagnosed based on a combination of clinical signs, laboratory testing, and medical imaging. 4 Magnetic resonance imaging is the procedure of choice in establishing the diagnosis and monitoring the progression of the disease. 5 Lesions in the white matter are pathognomonic. Typical MS lesions are located in the white matter cortically or juxtacortically, periventricular, in brainstem, cerebellum, or spinal cord. 6
A person with multiple sclerosis can have any neurological manifestation such as sensory, motor, or autonomic depending on the location of the lesions in the central nervous system (CNS). Multiple sclerosis symptoms may include sensory loss, motor or autonomic spinal cord symptoms, cerebellar symptoms, optic neuritis, or other ophthalmic symptoms namely internuclear ophthalmoplegia, trigeminal neuralgia, heat intolerance, fatigue, pain, depression, seizures, aphasia, or cognitive dysfunction. Fatigue is one of the most common symptoms of multiple sclerosis. 7
Multiple sclerosis may commence in a variety of ways on account of the location of the demyelinating lesion that determines the symptoms. Equilibrium disorders are quite frequent in MS being caused by the involvement of the cerebellum and the brain stem. 8
Authentic vertigo is estimated to affect about 20% of patients with multiple sclerosis. Demyelinating lesions are the cause of the vertigo, but true BPPV is not uncommon in MS. 9
There are reports of central positional vertigo caused by small lesions in the inner part of the superior cerebellar peduncle. 10
Vertigo and dizziness are not uncommon in the evolution of multiple sclerosis, but patients evaluated for vertigo and dizziness in otorhinolaryngology department are only rarely diagnosed with multiple sclerosis. Although the patients presenting for otoneurological examination due to vertigo or hearing loss are generally worried about having MS, we seldom diagnose the disease. Patients with dizziness and cerebellar syndrome are more prone to have multiple sclerosis compared to patients with vertigo. 11,12
Benign paroxysmal positional vertigo is the most frequent type of vertigo we encounter in everyday practice. There are some very typical characteristics of the BPPV that are used to diagnose the disease. The Dix-Hallpike test is considered the gold standard for the diagnosis of the BPPV of posterior semicircular canal. The nystagmus elicited by this test should meet some characteristics. It should begin after a period of latency between 5 and 20 seconds, it has a crescendo–decrescendo pattern disappearing in a period under 1 minute. It is also characterized by fatigability in case of repetition of the test. The nystagmus elicited at the test is typical for the posterior canal and it is described as torsional upbeating, the upper pole of the ear beating toward the dependent ear, and the vertical component beating upward. 13 All the positional vertigo that do not fulfill these diagnostic criteria have to be suspected of central origin and investigated properly.
Soto-Varela et al proposed diagnostic criteria for the suspicion of nonbenign positional vertigo: (1) association with signs or symptoms of neurological disorder, (2) nystagmus without dizziness in positional diagnostic tests, (3) atypical nystagmus direction, (4) poor response to therapeutic maneuvers, and (5) recurrence (confirmed by positional tests) on at least 3 occasions. 14
Central positional vertigo is usually less frequent compared to BPPV. The etiology is represented by vascular, tumoral, or demyelinating lesions in the cerebellum or the brainstem. The diagnosis of the central positional vertigo is based on the deviations from the classic diagnostic criteria of the benign positional paroxysmal vertigo. 15
In a study on 50 patients with downbeating nystagmus, most of the patients had central positional nystagmus associated with different CNS disfunction manifestations (38), only 12 patients had idiopathic positional nystagmus, possibly anterior canal lithiasis. 16
Anterior canal BPPV is the rarest form of BPPV accounting only for 1% to 2% of all BPPV. The diagnosis of this type of positional vertigo is based on the Dix-Hallpike maneuver in which a downbeating nystagmus is elicited, with or without of a torsional component (clockwise for the left canal and contraclockwise for the left canal). 17,18 Anterior canal BPPT is extremely rare and the diagnosis should include the careful examination of the eye movement and associated signs and symptoms in order to exclude a central etiology.
Conclusion
We consider this case particular given the fact that the patient who seemed to be having MS for a long time did not experience any other symptom except for the positional vertigo and nystagmus. Central positional nystagmus must be suspicioned whenever the nystagmus elicited at the positional testing is atypical.
The examination of the eye movements at the positional and positioning testing has to be very accurate because minute modifications cannot be observed easily. VNG recording of the nystagmus is useful in diagnosing atypical eye movements. The anterior semicircular canal paroxysmal positional vertigo must always be carefully evaluated to exclude a potential central etiology.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.