
Abstract
We present a case of a 50-year patient with a severe form of otosclerosis (double ring) that was successfully implanted. We used a bone-anchored hearing implant for restoring the hearing in the right side and a cochlear implant in the left side; both surgeries did not show any complications. For reducing the risk of a secondary bone ossification related to the trauma of cochleostomy for electrode’s insertion, we used a round window approach. The patient recovered a normal auditory threshold and normal speech perception capacity both in silence and noise conditions 1 year after surgery.
The use of cochlear implant (CI) in advanced otosclerosis is still debated despite it has been shown that its use allows a good recovery of hearing functions. 1 The controversies are related to an increased risk during the surgical procedures 2,3 , and a possible hearing loss recurrence caused by a bone ossification of the cochlea related to the trauma of electrode’s insertion. 4 An electrode insertion through a cochleostomy determines an important inflammation responsible of the increased ossification’s risk. 5 Some authors proposed to insert the CI through the round window 6 because this procedure is less traumatic 6 than cochleostomy.
We present a case of 50-year-old man admitted to the Otolaryngology Department of a tertiary referral center in July 2019 reporting a worsening of hearing loss due to a known bilateral otosclerosis. The patient had a binaural hearing aid (HA), but he had referred that currently he was uncapable to correctly understand the speech especially in noise condition.
Pure tone audiometry (PTA) showed a severe sensorineural hearing loss in the left side and a moderate conductive hearing loss in the right side. Tympanogram was within normal limits; stapedius reflexes were absent bilaterally. A speech perception test in quite conditions with HA showed a 75% discrimination on the right side and 25% on the left side. The same test performed in noise, showed a bilateral 20% decrease in discrimination. High-resolution computed tomography (HRCT) scan revealed a bilateral pericochlear hypodensity named as “double ring” (arrows), a clear and rare sign of advanced-stage cochlear otosclerosis (Figure 1).
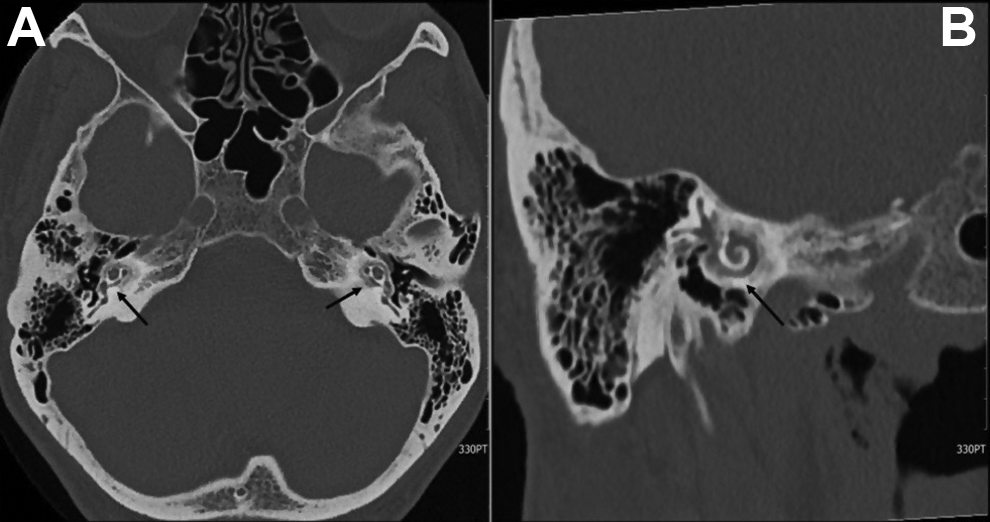
High-resolution computed tomography (HRCT) scan of a patient with “double ring” due to severe otosclerosis. The black arrows show the additional cochlear turn that was identified during the radiologic exam in axial (A) and coronal view (B). The middle ear structures were bilaterally preserved and normal as well the labyrinths.
We decided to use a bilateral implant for restoring a symmetric auditory function due to the impact that an asymmetric hearing ability may have on the professional life, and the cognitive ability of our patient. 7 A bone-anchored hearing implant (BAHI) was used in the right side and a CI in the left side. As BAHI, we used a BAHA (R) applied with standard technique. 8 As CI, we used a Synchrony 2 by Medel; the CI electrode was inserted through the round window as illustrated in Figure 2. The patient did not present any complication after both surgeries.
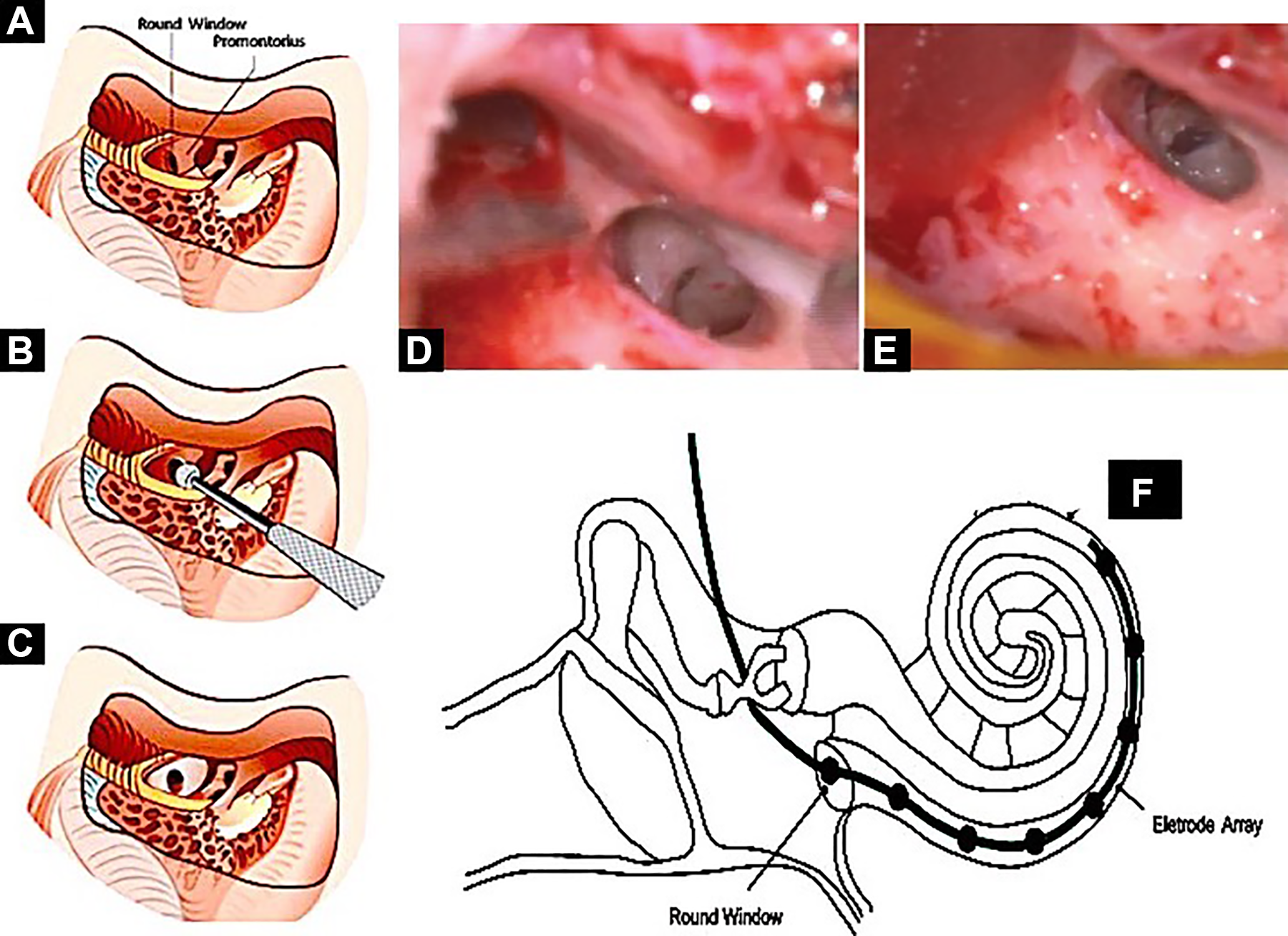
Surgical technique of cochlear implant (CI). A, Drawing illustrates the position of the round window. B, Drilling of the bone close to the facial nerve for improving the visualization of the round window. C, Opening of the round window by soft drilling of the bone over the fenestra. D, Surgical view of round window in vivo. E, Opening of round window in vivo before the insertion of the electrode into the cochlea. F, The drawing shows the electrode after its introduction into the cochlea.
Follow-up hearing evaluations were performed monthly; at 1-year follow-up, the patient presented normal auditory thresholds in quite conditions at PTA. Speech discrimination in noise was 85% in the right and 88% in the left side.
Otosclerosis is an osteodystrophy of the otic capsule that affects people in the second to fourth decade of life and can determine a conductive, mixed, or sensorineural hearing loss. The diagnosis is made by auditory investigation and HRCT. The treatment of hearing loss is based on the computed tomography findings; in case of an antefenestral involvement, stapedoplasty is the elective treatment, while in cases of retrofenestral damage, HA treatment is preferred to CI due to difficulties in electrode insertion caused by the cochlear osteodystrophy that increase the risk of short- and long-term complication. 6
The follow-up of our patient is still too short to affirm that by using round window approach is possible to avoid bone ossification, 4 but we can confirm that no intraoperative, perioperative, or postoperative complications came out during the electrode insertion by using this technique. 6 We suggest, by observing our results, to use a round window approach instead of cochleostomy in advanced otosclerosis, especially in type 2A otosclerosis. 6 The restoration of symmetric hearing capacities is strongly recommended for improving the performances of these patients especially the ones in young/adult age.
Footnotes
Authors’ Note
The data sets used and/or analysed during the current study are available from the corresponding author on reasonable request. A.D.S. and M.R. wrote the manuscript draft and performed literature search. D.M. and A.G. contributed to data interpretation and manuscript correction. A.D.S. was responsible figure editing. All authors were equally involved in clinical diagnosis and surgical management of the patient. All authors have approved the final version of the manuscript. Written informed consent to publication was obtained.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.