Abstract
The indications for cochlear implantation have gradually expanded as advancements in technology have evolved, resulting in improved audiologic outcomes for both adult and children. There remains a significant underutilization of cochlear implant technology in the United States, and recognition of the potential benefits of cochlear implantation for non-traditional indications is critical for encouraging the evolution of candidacy criteria. Adult cochlear implantation candidacy has progressed from patients with bilateral profound sensorineural hearing loss (SNHL) to include patients with greater degrees of residual hearing, single-sided deafness and asymmetric hearing, and atypical etiologies of hearing loss (eg, vestibular schwannoma, Ménière’s disease, and otosclerosis). Indications for pediatric cochlear implantation have similarly evolved from children with bilateral severe to profound SNHL to implanting children at a younger age, including those with residual hearing, asymmetric hearing loss, inner ear malformations, as well as cochlear nerve deficiency. In this editorial, the literature investigating cochlear implantation for nontraditional indications is reviewed with an aim to use the best available evidence to encourage the evolution of candidacy criteria.
Keywords
Introduction
Cochlear implantation is a well-established treatment for adults and children with sensorineural hearing loss (SNHL). Since the approval of the original single-channel cochlear implant (CI) by the US Food and Drug Administration (FDA), the device has rapidly evolved into several commercially available multichannel systems. 1 –3 Due to advancements in engineering and speech processing technology, associated improved outcomes, and increased familiarity of the medical and audiologic communities, indications have slowly but consistently expanded. Despite the gradual expansion of candidacy criteria, there is significant underutilization of very effective technology. In this editorial, the evolving criteria for adult and pediatric cochlear implantation are reviewed with an eye to encouraging appropriate utilization of CI.
Adult Cochlear Implantation
Audiologic candidacy for cochlear implantation has historically been based on aided sentence recognition performance (eg, AzBio sentences). Traditional FDA criteria evolved from bilateral profound SNHL to bilateral moderate to profound levels of hearing loss with limited benefit from conventional amplification. 4 –7 Food and Drug Administration thresholds for candidacy increased to ≤50% speech recognition ability in the ear to be implanted or ≤60% in the binaural best-aided condition. Scores up to 60% are currently used by many private insurers while Medicare criteria remain ≤40%. Protocols for incorporating noise into CI evaluations vary by institution; however, patients who qualify exclusively with noise have been shown to benefit from CIs. 8 Monosyllabic word recognition has been proposed as an alternative tool due to performance ceiling effects and the semantic context associated with sentences. 4,5 Monosyllables are challenging and provide a more accurate metric for monitoring improvement. Sladen et al described the ceiling effect with AzBio sentences within 3 months of CI use, while consonant–nucleus–consonant (CNC) monosyllabic word scores only reached 80%. 4 The study included patients with CNC scores up to 40% and demonstrated speech recognition outcomes at least equivocal to the 2007 Nucleus Freedom North American trial, which used a stricter criterion of CNC <30%. A CNC score of ≤40% has thus been suggested as a threshold for candidacy. The Sladen et al study also demonstrated the potential benefit of CI in patients whose performance exceeded “traditional” criteria. 4,7 Gifford et al investigated speech perception in CI users with preoperative CNC scores ≥30% (ie, exceeding the criteria of the Nucleus Freedom trial). 5,7 Improved scores were seen regardless of listening condition (CI with or without contralateral amplification). Several studies have demonstrated similar results in patients whose performance exceeded “traditional” criteria. 4,6,9 –12 The authors encouraged a reassessment of candidacy criteria to include patients not benefitting from conventional amplification. As traditional criteria evolve, guidelines may specify word recognition performance as the primary indicator of potential benefit from CI.
Patients with residual low-frequency hearing who struggle with hearing aids are an example of those who may fail to meet traditional CI criteria. For these patients, CIs with “electric-acoustic stimulation” allow amplification of low frequencies and electrical stimulation of the middle- and high-frequency ranges. 13 Electric-acoustic stimulation, introduced in 1999 and FDA approved in 2014, improves speech recognition in noise and provides a finer spectral resolution of complex auditory stimuli (eg, music). 6,14 –16 Food and Drug Administration labeling for a shortened electrode array specifies unilateral CNC word scores ≤60% for candidacy, although the addition of acoustic amplification is possible even with a full-length array. As “hybrid” CIs gained popularity, efforts turned toward minimizing trauma during electrode insertion to preserve intracochlear structures and thus residual hearing. Electrode length was identified as a critical factor: greater insertion depth provides improved speech perception in “traditional” candidates but may destroy residual hearing. Shorter electrodes, however, may compromise outcomes for patients who ultimately lose residual hearing and require electric-only stimulation. 6,17 –19 Optimizing insertion depth (∼360°), thinner electrodes, and round window insertions (vs cochleostomy) were recognized as strategies for “soft” surgery. 20 –22 Intraoperative monitoring via electrocochleography has also become available as an adjunctive tool to minimize intracochlear trauma. 23,24 Intraoperative electrocochleography may be obtained directly through the CI during insertion; acoustic stimulation is provided with an insertion of earphone, whereas cochlear hair cell and neural responses are detected through the electrode array. 25 The recorded signal provides intraoperative feedback regarding cochlear hair cell function and may influence the insertion technique or depth of insertion when hearing preservation is intended.
A difficult question for unilateral CI users may be the decision to pursue a second implant. Two implants provide the benefits of binaural hearing, including sound localization, binaural summation and squelch, and speech recognition with spatially separated noise. 26 –28 Cochlear implant users with residual hearing in their contralateral ear may receive complementary (ie, “bimodal”) input when aided. However, for patients who are not clearly receiving bimodal benefit, the decision to pursue a second CI is not straightforward. Gifford and Dorman compared speech recognition between adults using bimodal stimulation and adults with bilateral CIs. 26 No significant differences in speech perception or binaural summation were seen using traditional clinical measures. Interestingly, the patient’s perception of whether a second CI is warranted appeared to be of greater clinical utility than routine objective testing.
Cochlear implants have increasingly been performed for patients with single-sided deafness (SSD). Traditional treatments included contralateral routing of signals or bone-conduction hearing aids. Cochlear implants were initially discouraged due to the misconception that electric stimulation would not integrate with contralateral acoustic input. However, van de Heyning et al demonstrated feasibility after implanting 21 patients with SSD and debilitating tinnitus. 29 All patients experienced tinnitus improvement and became daily CI users. Implanted SSD patients experience a reduction in tinnitus as well as improved speech perception in noise, sound localization, and quality of life. 30 –35 In 2019, MED-EL’s CI system was the first device approved by the FDA for SSD.
Cochlear implants have also been performed for atypical etiologies that may introduce unique challenges and unpredictable outcomes. Patients with advanced otosclerosis may develop cochlear ossification or round window obliteration, requiring an extended cochleostomy. 36,37 Cochlear ossification may impact the electrode–neural interface, affecting performance. 38 Posttraumatic SNHL (eg, temporal bone fracture) may be associated with intracochlear fibrosis. 39,40 Cochlear implantation has also been well-described for patients with Ménière’s disease (MD) with favorable audiologic outcomes. 41 However, these patients may pose a challenge postoperatively by exhibiting fluctuating performance requiring device reprogramming. 41,42 In patients with bilateral MD, the status of the contralateral vestibular system must be considering CI as surgical violation of the inner ear may result in additional vestibular injury. Patients with MD who have previously undergone labyrinthectomy may require updated imaging (ie, computed tomography) to ensure a patent cochlear duct is present. Approximately one-third of patients undergoing a labyrinthectomy develop cochlear ossification, which would preclude insertion of an electrode array. 43 Patients with vestibular schwannomas can also benefit from CIs, regardless of treatment modality, if an intact and functional cochlear nerve can be preserved. 44 –47 The imaging artifact created on magnetic resonance imaging by CIs must be considered in patients for whom surveillance is desired. For intralabyrinthine or intracochlear schwannomas, cochleostomy or cochleoectomy may be required; the electrode may be inserted through tumor if resection is not possible. 48 –50
In conclusion, adult CI criteria have expanded to include patients with greater degrees of residual hearing, SSD, and atypical etiologies of SNHL. However, CIs are only being provided to the minority of patients who would meet candidacy criteria. 51 Reasons for this underutilization may include poor regional access, unfamiliarity with the device, and a lack of understanding the population who may benefit. As awareness of the technology improves, research efforts will continue to expand the definition of candidacy and potential indications for CI.
Pediatric Cochlear Implantation
Clearly, the evidence supports expanding indications for adult CI candidacy. It is arguably even more critical for children to have sufficient access to sound to facilitate the development of speech and language. As such, one might expect pediatric CI candidacy to be more expansive to ensure that children do not miss out on critical opportunities for the development of higher-level auditory centers and associated communication abilities. Counterintuitively, the CI candidacy criteria for children is actually more stringent than adults, creating potential, at times, insurmountable barriers to CI until a child demonstrates unmistakable difficulty with hearing and communication. In fact, according to FDA labeling, children must miss 70% to 88% of the incoming signal to qualify for CI. 52 Since the late 1990s, FDA labeling for pediatric CI has remained static, requiring children under 2 years of age to have profound (>90 dB HL) bilateral SNHL and children 2 to 17 to have severe-to-profound bilateral SNHL. In both cases, they must also demonstrate little to no benefit with appropriately fitted hearing aids. Yet, the evidence in the literature is compelling that attitudes and clinical decision-making toward CI must be more aggressive and progressive than labeling suggests in order to obtain the best outcomes. This perspective is particularly true in 4 aspects of candidacy: asymmetric hearing, residual hearing, age at implantation, and structural anomalies.
First, studies have demonstrated that, as with adults, considering each ear individually is critically important in the determination of CI candidacy for pediatric patients. 52 –54 Maintenance of binaural stimulation is essential for localization and understanding speech in noise. Fortunately, FDA labeling was updated in July 2019 to include children aged 5 years and older who have SSD or asymmetric hearing loss with extremely poor word recognition (<5%). While the expansion of the indication to recognize the benefits of adequate binaural hearing, the literature suggests that children with greater degrees of word understanding in the poorer hearing ear may similarly benefit from implantation. 52,55 –57 Further, children under the age of 5 have also been successfully implanted. Cushing et al suggest that every effort must be made to limit the period of auditory deprivation in CI candidate ear, encouraging CI as early as possible before the age of 4 years in the case of congenital deafness. 53,58 Importantly, the combination of acoustic hearing in the better ear with electric in the poorer hearing ear, generally improves the pediatric recipient’s outcomes.
Second, residual hearing in the implanted ear need not be a contraindication to implantation. In fact, multiple studies have suggested that, although not FDA indicated, electroacoustic stimulation, sometimes combined with short electrode arrays, are similarly beneficial in children as adults. 59 –61 This benefit is particularly noticeable in background noise, where the signal-to-noise ratio is poor, 59 which is a common environment for school-age children.
Third, the current FDA guidelines for candidacy for pediatric CI require profound bilateral SNHL in children 9 to 24 months (age limits expanded in 2020). There is robust evidence supporting early implantation before 12 months of age but now, there is increasing evidence that shows that even earlier implantation, as early as 6 months, is safe and has improved outcomes. 62,63 Cochlear implant surgery in infants has been shown to have a slight increase in readmission rates, 64 but similar complication rates as older children. 63,65,66 In addition, earlier implantation has been shown to have better vocabulary outcomes, 67 better speech production, 63 auditory performance, and receptive language scores, 68 even if the contralateral ear is completely normal. 53 A series of 21 children who were implanted as early as 10 months (up to age 11 years) showed significant improvements in the combined head shadow effect, lateralization, and parental overall level of satisfaction. 69 Children also seem to be accepting of CI. In one series, children as young as 1 year of age have shown to be receptive of CI and shown consistent use of CI in setting of SSD. 70 Younger age at implantation thus seems to have beneficial outcomes whether CI is performed in setting of bilateral or unilateral hearing loss.
Cochlear anomalies, ossification, and cochlear nerve deficiency should not be viewed as an absolute contraindication for CI in children. Cochlear anomalies, which can range from mild to severe cochleovestibular dysplasia, have been shown to be safely implanted with favorable outcomes. A systematic review of outcomes with CI in inner ear dysplasia found postoperative speech perception abilities often ranges from 54% to 84% depending on the severity of dysplasia. 71 Although lower than reported outcomes when compared to CI in normal anatomy, there is still meaningful benefit noted in speech perception outcomes. 72 There is increased surgical difficulty noted in these patients, however, this is not prohibitive to implantation. 71,73 Similarly, cochlear ossification, which may be encountered after bacterial meningitis, has been shown to result in increased surgical difficulty and may affect audiologic outcome if sufficient electrodes are unable to be inserted. 74 Labyrinthitis ossificans has also been associated with an increased incidence of postoperative facial nerve stimulation after CI, which requires device remapping and electrode deactivation. 75
Distinct from inner ear malformations, cochlear nerve aplasia has long been considered a contraindication to CI. Cochlear nerve deficiency includes cochlear nerve aplasia in which the nerve is completely absent and nerve hypoplasia in which there is a smaller sized cochlear nerve in the internal auditory canal. Recently, the limitations of imaging in the differentiation of aplasia and cochlear nerve (CN) deficiency have been recognized. Kutz et al reported on a series of 7 patients who underwent CI with no evidence of nerve identified on imaging. 76 In this study, one child developed early closed-set speech recognition and the other 6 children developed only speech detection or pattern perception. In another larger series with 64 patients with cochlear nerve aplasia who underwent CI, nearly 50% of the patients achieved Categories of Auditory Performance scores of 5 to 7. 77 However, further studies are needed to evaluate outcomes over prolonged follow-up and with quality of life assessments to determine guidance for considering CI before proceeding to auditory brainstem implantation.
Finally, a patient’s cognitive or developmental delay should not be considered a contraindication nor a reason to withhold CI. Studies have shown that although speech and language development may not result after CI due to the underlying disability, families report broadened communication skills, 78 improved interactions, 79 and less familial stress. 80
In summary, the evidence for the expansion of pediatric CI continues to grow. It is incumbent on clinicians to recognize that while FDA labeling is often utilized to determine insurance coverage, it is often too stringent to reflect standard clinical practice and innovative approaches to hearing rehabilitation in children. The FDA criteria certainly do not capture all circumstances in which a child may benefit from implantation. By considering individual ear performance, communicative abilities, and child-specific development, clinicians can best equip children with access to technology that optimizes hearing and communicative outcomes.
Conclusion
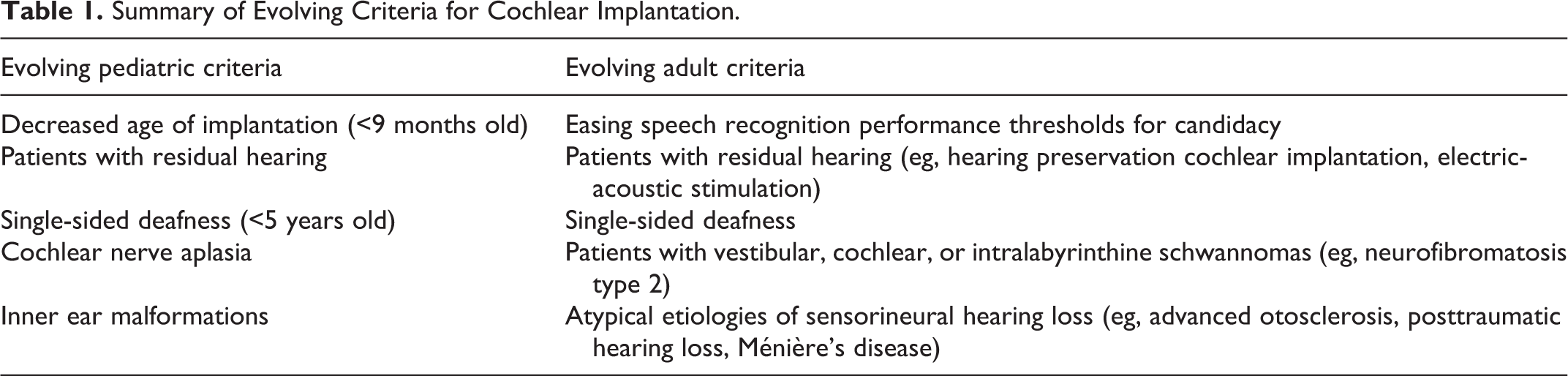
Candidacy for CI in both the adult and pediatric populations have continued to expand, at least in clinical practice (Table 1). It is important to realize that despite the available evidence, FDA and insurance payer criteria tend to lag behind the best clinical practice and should not be considered an inflexible requirement for determining candidacy. Although there may persist discrepancy between candidacy and coverage, the clinician’s role is to advocate for those patients who stand to benefit from CI and encourage utilization as early as possible to maximize outcomes. As criteria continue to expand, it is imperative to encourage modification to outdated protocols and guidelines such that they align with literature-supported best clinical practice.
Summary of Evolving Criteria for Cochlear Implantation.