
Abstract
Conidiobolomycosis is an uncommon, chronic, localized subcutaneous mycosis primarily affecting rhinofacial region. It is reported mainly from tropical and subtropical countries. The condition is underreported due to the lack of clinical suspicion and usually mismanaged. This rare mycosis is due to the genus Conidiobolus within the order Entomophthorales of class Zygomycetes. Here we present 3 cases of rhinofacial conidiobolomycosis in otherwise healthy adults from different parts of Sri Lanka over 1-year period. All patients had disfiguring subcutaneous lesions in the rhinofacial area. The diagnoses were based on isolation of Conidiobolus coronatus in clinical specimens.
Introduction
Conidiobolomycosis is an uncommon, chronic, localized subcutaneous infection. 1,2 This infectious disease is caused by a fungus belonging to the genus Conidiobolus within the order Entomophthorales of class Zygomycetes. 1 Conidiobolus coronatus, Conidiobolus incongruous, and Conidiobolus lamprauges have been reported as the 3 main species of the order Entomophthorales that lead the conidiobolomycosis in humans and animals. 2 The disease frequently presents as painless hard swelling of the rhinofacial region of immunocompetent patients in tropical countries. 2 However, the disseminated form of conidiobolomycosis has been reported rarely among both immunocompetent and immunocompromised patient populations. 2,3,4 The diagnosis is based on culture and histopathological evidence of biopsy from the affected region. 2,3 High degree of clinical suspicion is required for early diagnosis and treatment of the condition which was associated with severe facial disfigurement.
Our article will review 3 case reports of Conidiobolomycosis presented to the Department of Mycology, Medical Research Institute, Sri Lanka, and the difficulties in diagnosing this condition.
Case 1
A 17-year-old male from Kuliyapitiya, Sri Lanka, presented to ENT clinic at National Hospital of Sri Lanka (NHSL) with slowly progressive swelling of his nose (Figure 1). He developed bilateral nasal swelling 2 months ago, which was initially right sided but progressively increased and became bilateral. The swelling later progressed and involved the forehead. He had a history of 1 episode of epistaxis and feeling of bilateral nasal obstruction. He also complained dull pain over the affected area. He could not recollect the history of local trauma. He was nondiabetic, nonalcoholic previously healthy male with no family history of congenital immunodeficiency syndromes. He was schooling at the time of presentation, and no occupational risk was identified.

Swelling of the nose of case.
He had presented to the local government hospital and undergone examination under anesthesia of nose 1 month back. A growth involving right inferior turbinate and right-side lateral nasal wall was detected, and a biopsy has been taken from right lateral nasal wall and sent for histology.
The histology of biopsy tissue revealed the inflammatory lesion destructing mucosa and did not find any evidence of fungal pathogens. The computed tomography (CT) obtained from the same time period found ill-defined enhancing lesion in right vestibule (Figure 2).
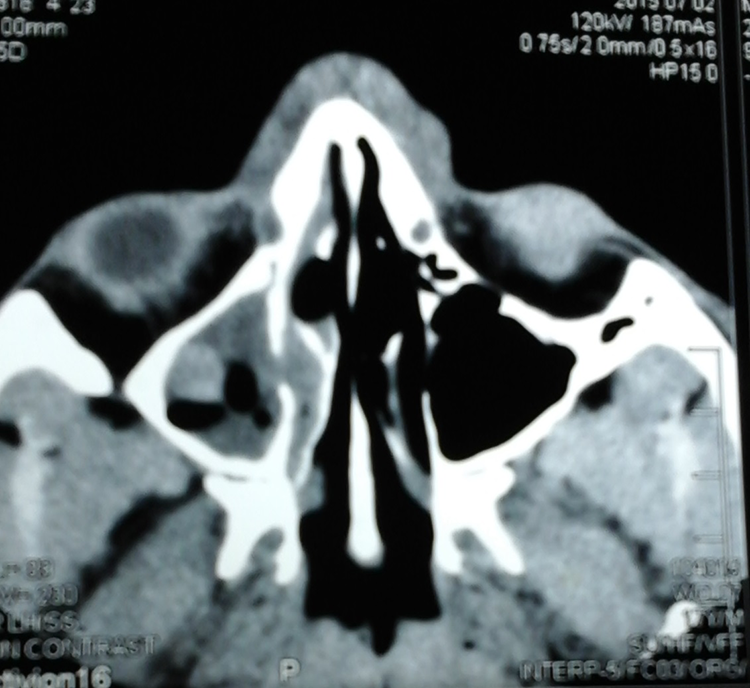
Ill-defined lesion of the computed tomography (CT).
He was subsequently referred to ENT clinic in NHSL, as his symptoms were not relieved and his nasal swelling progressed.
When he presented to the NHSL ENT clinic, he had nontender, nonerythematous, diffuse bilateral nasal swelling. The swelling has progressed to the forehead, but there was no evidence of local lymphadenopathy. The rest of the examination was unremarkable.
All of his blood investigations including erythrocyte sedimentation rate (ESR) were within normal ranges. He underwent endoscopy-assisted right nasal cavity lesion biopsy under general anesthesia, and abnormal nasal wall (inferior meatus) and abnormal friable tissue were seen with poring of pus. There was a growth involving right inferior turbinate. The left nasal cavity appeared normal. A biopsy was taken for histology and fungal studies.
We sent this biopsy specimen to Department of Mycology, and the direct smear with 10% KOH revealed broad, thin-walled, hyaline fungal filaments with very few septate. It was suggestive of fungi from Zygomycetes family, and we were informed over the phone to the responsible ward and requested for the broad-spectrum antifungal drugs. The biopsy specimen was inoculated on 4 agar slants of Sabouraud dextrose agar (SDA) with chloramphenicol, and 2 slants were incubated at 37°C and 2 at 26°C.
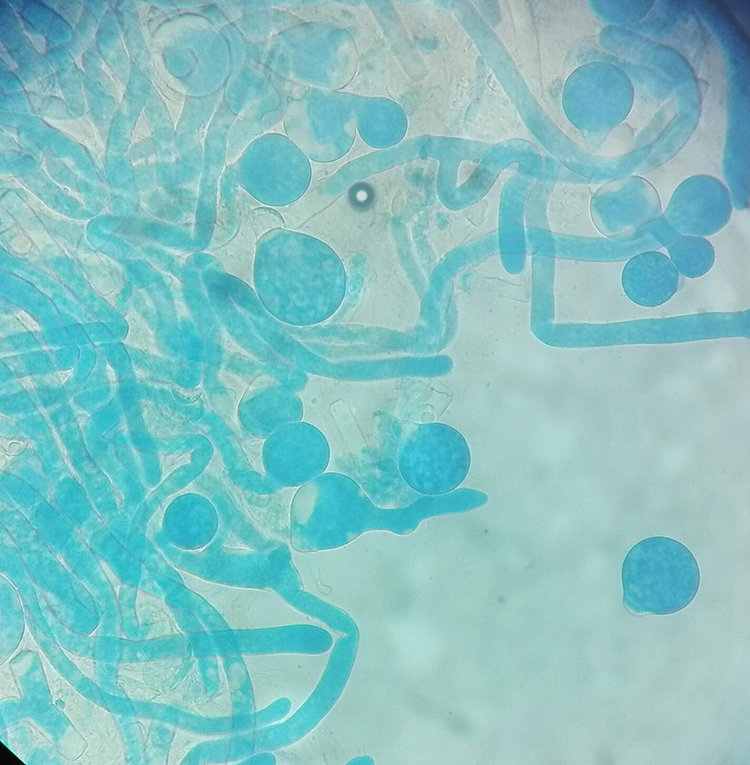
After 3 days of incubation, we could observe small white colonies on 2 agar slants of SDA with chloramphenicol at both 37°C and 26°C. These colonies became flat, cream-colored and waxy, slightly powdery, glabrous colonies with time. The opposite walls of the culture slants became cloudy within the next few days (Figure 3). Lactophenol cotton blue (LPCB) mount showed several conidiophores and terminal spherical conidia with villi. The fungal hypha was very thin and hyaline with infrequent septa (Figure 4). Based on these features, the fungus was identified as C coronatus.
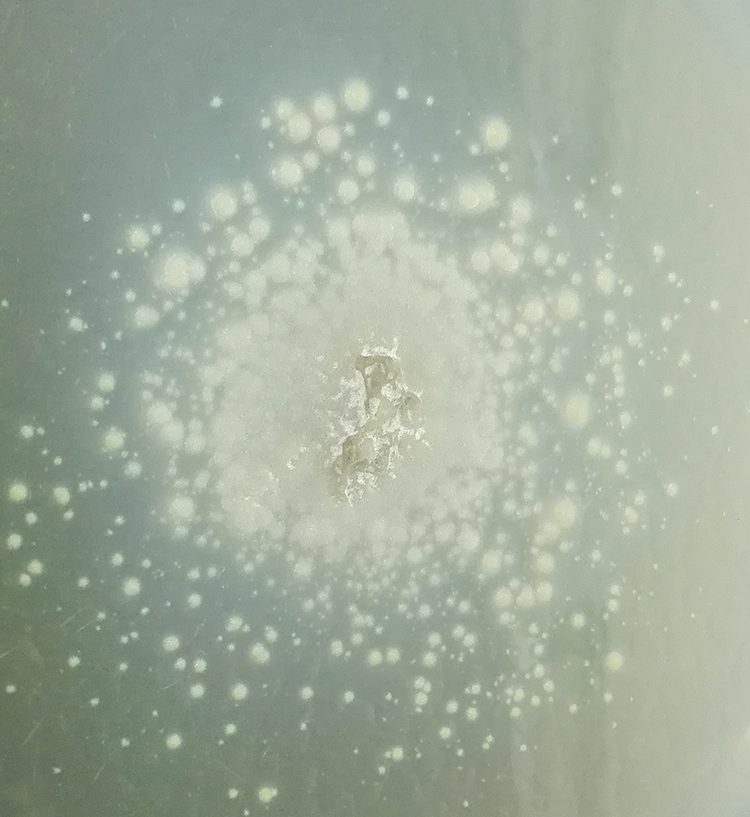
Waxy, slightly powdery colony of Conidiobolus.
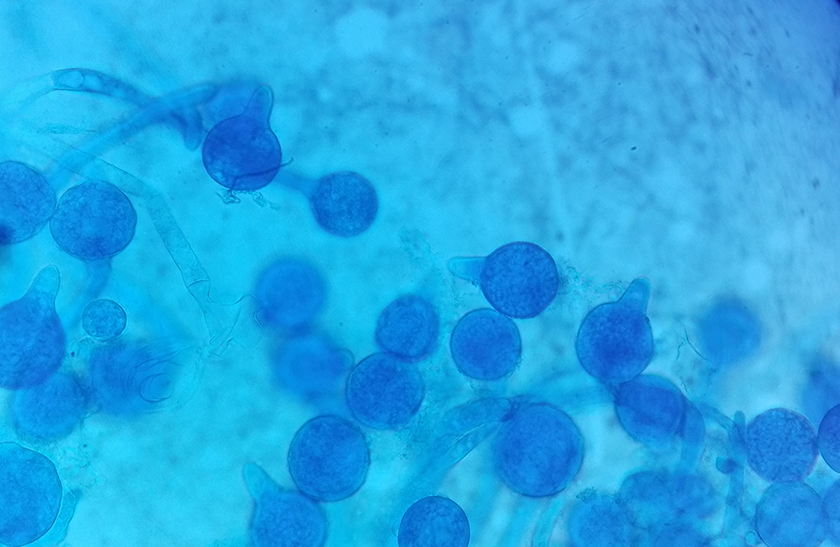
Microscopic appearance of the tease mount.
The patient was started with intravenous (IV) amphotericin B 1 mg/kg/d initially as the response to first information of the direct smear. It was later on changed to oral itraconazole 200 mg twice daily after the culture result was obtained. After 3 weeks of oral itraconazole treatment, the patient experienced remarkable clinical improvement as evidenced by regression of facial swelling and relief from symptoms. He was on the same dose of oral itraconazole for further 3 months while assessing the liver function tests. He was followed up at the ENT clinic with no ill effects of drugs or further recurrences.
Case 2
Case 2 was a 67-year-old, previously healthy male who complained of nasal blockage for 5 months duration. There was no significant past medical history of tuberculosis (TB), chronic sinusitis, or past surgery at the affected site. A lateral rhinotomy was done, and the biopsy report was suggestive of granulomatous infiltration with many eosinophils, with possibilities of parasitic infection, rhinoscleroma, TB, or fungal infection.
He was admitted to the hospital for further investigations. On admission, he was having left orbital pain and nasal block (Figure 5). Rest of the physical examination findings were unremarkable.

Nasal swelling of the second patient.
The basic investigations of full blood count, ESR, and chest X-ray were normal, and his random blood sugar was normal (88.1 mg/dL). His Mantoux test was negative. Since his condition was not improving, he was started with IV amphotericin B 39.1 mg in 5% dextrose empirically and planned for another biopsy. The biopsy sample was sent to Medical Research Institute for fungal studies.
The direct smear of the biopsy with 10% KOH was positive for broad, aseptate fungal filaments giving the clue of fungi of Zygomycetes. This was informed to the ward. The culture grew after 3 days giving small white colonies on agar slants of SDA with chloramphenicol at both 37°C and 26°C. These colonies grew in to flat, cream-colored, waxy colonies over time. The opposite walls of the culture slants became cloudy within the next few days. The LPCB mount showed several conidiophores and terminal spherical conidia with villi. The fungal hype was very thin and hyaline with infrequent septa. Based on these features, the fungus was identified as C coronatus.
It was informed to the ward, and IV amphotericin B was stopped and oral itraconazole twice daily was started. He was discharged while on oral itraconazole and was followed up at clinic with no further recurrences.
Case 3
A 39-year-old male who was previously diagnosed to have polycystic kidney disease and hypertension and was on antihypertensive drugs presented with left-sided nasal obstruction and on and off epistaxis for 1 month duration. This was accompanied with chronic headache. Irrespective of repeated treatment obtained from private sector, his symptoms persisted and got worsened. As a result, he was admitted to a local teaching hospital and was further investigated. The CT revealed the suspicious growth on left frontoethmoidal region. He had undergone a biopsy of the lesion and was then admitted to NHSL.
The initial presentation at NHSL revealed a disfigured facial appearance with severe bilateral periorbital swelling. The left side of periorbital swelling was extending to the left cheek. The overlying skin was intact. There was no regional lymphadenopathy (Figure 6). He had lost vision of his left eye. However, the rest of the physical examination was unremarkable.

Facial disfigurement of the third patient.
Based on his acute severe presentation and previous CT scan report, a clinical impression of suspected left frontoethmoidal malignant neoplasm was made.
The CT scan of the paranasal sinuses before treatment showed soft tissue swelling of the left nostril, retention cyst in the left maxillary sinus, and hypertrophy of left inferior turbinate.
He had to undergo left lateral rhinotomy and medial maxillectomy and frontal sinus exploration. Biopsy samples were taken and sent for histology and fungal studies.
The Department of Mycology received a biopsy from left-sided nasal cavity lesion of a 39-year-old male patient on November 19, 2015. The direct smear of the biopsy with 10% KOH revealed broad, thin-walled, nonseptate, nonpigmented fungal filaments that is suggestive of fungi from Zygomycete family. The ward was informed over the phone and requested for the broad-spectrum antifungals .The biopsy specimen was inoculated on 4 agar slants of SDA with chloramphenicol, and 2 slants were incubated at 37°C and 2 at 26°C.
After 5 days of incubation, we could observe small white colonies on 2 agar slants of SDA with chloramphenicol at 26°C. They turned into flat, cream-colored, and waxy, glabrous colonies with time. The opposite walls of the culture slants soon became covered with conidia giving a cloudy appearance (Figure 7). The LPCB mount showed several conidiophores and terminal spherical conidia with villi (Figure 8). Based on these features, the fungus was identified as C coronatus.
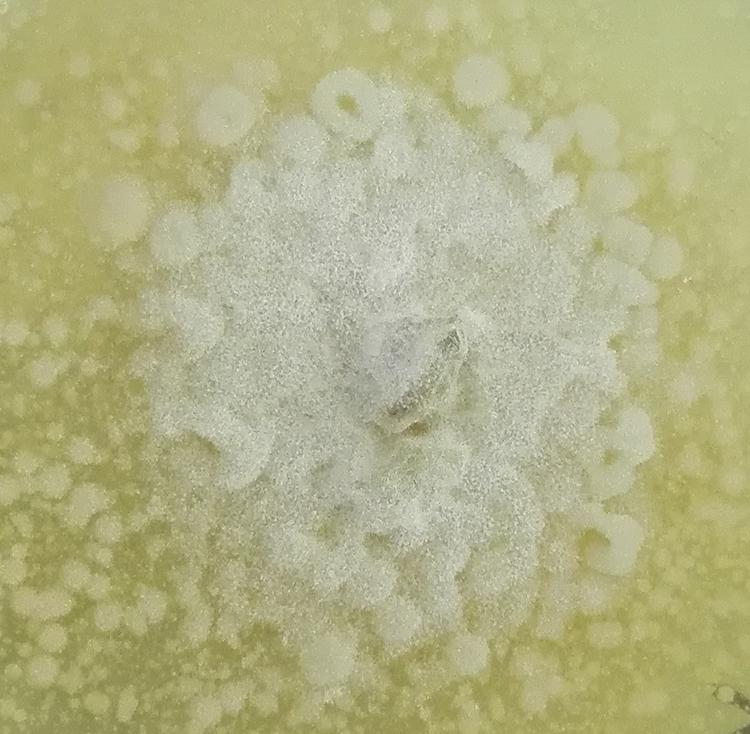
Macroscopic appearance of colony.
Microscopic appearance of colony.
A final diagnosis of rhinoentomophthoromycosis was made. He had been started with IV amphotericin B based on the direct smear results. With the identification of the culture, oral itraconazole was started 200 mg twice daily with oral Terbinafine 250 twice a day for 4 months. At the same time, the patient was treated with freshly prepared oral potassium iodide in a concentration of 1 g/mL.
His liver function tests and full blood count was monitored. Further, he was referred to an ophthalmologist to assess his vision, as he had lost vision in the left eye. Repeat CT scan of para nasal sinuses done at 3 weeks of treatment showed the resolution of the swelling.
His periorbital swelling and facial disfigurement disappeared gradually over 4 months of treatment, and the patient regained his normal facial appearance except small unhealed wound at the surgical site .
The biopsy obtained from the unhealed wound site grew Aspergillus species later. At the end of 4 months of oral itraconazole therapy, his repeat CT scan of para nasal sinuses and a nasal endoscopy was uneventful. He was on oral itraconazole 200 mg twice daily for a total of 5 months duration. The patient was under follow-up and is asymptomatic except for a nonhealed wound at the surgical site, which he needs to undergo a plastic surgery.
Discussion
Conidiobolomycosis is a rare subcutaneous mycosis that is associated with chronic granulomatous inflammation of upper respiratory mucosa and adjacent subcutaneous tissues. 1 It has been reported worldwide but mainly from tropical and subtropical countries such as West Africa, Central Africa, America, and countries in South East Asia including Sri Lanka. 1,2,5 This disease is caused by fungi of the genus Conidiobolus of order Entomophthorales in class zygomycetes. 1,4 Conidiobolus spp are saprobes distributed in decomposing plant matter, soil, and rotting vegetation in moist warm climates. 2,3 Conidiobolus spp has also been isolated from the gastrointestinal tracts and feces of lizards, frogs, reptiles, and other animals. 2,6 Out the 27 identified species, C coronatus, C incongruous, and C lamprauges are known to infect humans. 2,4,7
Although the exact mode of transmission has not been clearly established, the predilection of the organism to infect the head and face suggests that the inhalation of spores and introduction of them in to the nasal cavity by soiled hands could be the most probable routes of infection. 1,2,3
Adult males in the 20 to 50 years age-group, who engage in outdoor activities or outdoor occupations, are more affected. 1,2 All our 3 patients were male patients within this age-group. However, 2 of them denied of frequent outdoor activities.
This disease is frequently seen among immunocompetent and otherwise healthy individuals like our patients. 1 Localized chronic rhinofacial mycosis is the most common clinical presentation of human infection with Conidiobolus species. 1 All our patients had rhinofacial lesions, initially presented as progressive swelling over the nose, perinasal tissue, eyelids, or periorbital region. This is the most frequent initial presentation, and it will also appear as a swelling over the upper lip or over the malar regions of the face.6,7 The disease may spread to all adjacent structures, including the paranasal sinus, and to the subcutaneous tissue of the forehead and periorbital region. 1,2,3
Affected patient may experience chronic symptoms of epistaxis, nasal polyposis, nasal block, nasal discharge, and chronic sinusitis. 1,5 Our third patient had few episodes of epistaxis, and all 3 patients had feeling of nasal blockage.
Firm, painless subcutaneous nodules appear as the infection spreads, and these nodules are palpable through the skin. 2,6 These lesions are firmly attached to the underlying tissue sparing the bone, while overlying skin remains intact. 2,6 Most of the long-term untreated patients with conidiobolomycosis may present with severe facial disfigurement as seen in our third patient. 2
Involvement of nasolacrimal duct, orbit, and contiguous lymph nodes are relatively uncommon presentation of conidiobolomycosis. 3,5 Involvement of pharynx and larynx with extensive destruction result in dysphagia, laryngeal obstruction, and chronic lymphedema which are the other uncommon clinical presentations. 6 Although our first and second patients did not have evidence of involvement of nasolacrimal duct, orbit, and contiguous lymph nodes, the third patient had orbital involvement and he lost his vision too.
Distant dissemination is not a common feature of conidiobolomycosis; however, disseminated infection has been reported rarely. 1 Disseminated cases with fatal outcomes are seen among both immunocompetent and immunocompromised patients, such as patients with lymphocytic lymphoma and renal transplant recipient. 5 Cases of disseminated Conidiobolus infections with endocarditis, pericarditis, vasculitis, and pulmonary involvement have been reported. 5,6
In these patients, granulomatous reactions have been detected in lymph nodes, esophagus, liver, jejunum, pericardium, endocardium, lung, kidneys, skeletal muscles, and brain. 2,5,6 Disseminated patients with fatal outcomes have been clinically resembled to mucormycosis due to their acute presentation and angioinvasiveness. 6 When the characteristic clinical features of chronic subcutaneous rhinofacial mycoses present, biopsy of subcutaneous or submucosal tissue are required to establish the diagnosis. 6
The direct smear and fungal culture and histopathologic demonstration of the etiologic agent are required for the definitive diagnosis. 2 Direct smear with 10% potassium hydroxide of biopsy tissue from the lesion would reveal broad, nonseptate or infrequently septate, thin-walled fungal filaments. 2 The biopsy specimens from the affected site from all our patients were positive for broad, nonseptate or infrequently septate, thin-walled fungal filaments in direct smear.
We used standard mycology medium, including SDA with chloramphenicol to inoculate biopsy specimens. All these 3 cases had characteristic features Conidiobolus sp in their colony morphology at 3 to 5 days. The other standard mycology media, including SDA, potato dextrose, and cornmeal agars provide satisfactory growth of Conidiobolus spp. 2,6 They have relatively fast growth, and their growth is more rapid at 37°C. Colonies demonstrate white obverse view and pale reverse view initially. However, their surface turns into beige to brown with time. Conidiobolus spp demonstrates flat, waxy colonies with folds and become powdery with age. Forcibly discharged conidia can stick to the lid of the Petri dish giving cloudy appearance in older cultures. These expelled spores may land on adjacent medium producing characteristic satellite colonies. 6,8
The LCB mount of the colony demonstrated less septate broad, thin hayaline hyphae. The short, erect, unbranched conidiophores (sporangiophores) produce single-celled (one-spored) large conidia (25-45 µm in diameter). These conidia are round to pyriform in shape and have prominent papillae on the wall. These microscopic features are characteristics of this genus which help to come to the diagnosis. Additionally, conidium of C coronatus produces hair-like appendages called villae. However, unlike C coronatus, C incongruus does not produce villous sporangioles. 6
The histopathology of the biopsy specimen of conidiobolomycosis shows hyphal elements as short, broad fragments without or with infrequent septae. 2 These fungal filaments are ensheathed by amorphous eosinophilic material, and this is known as Splendore-Hoeppli phenomena. 2 The adjacent area contains granulation tissue that is rich in eosinophils. 2
The delayed diagnosis of the conidiobolomycosis results in difficulties in the management. 2 Two out of the 3 patients had complete cure with prolong antifungal treatment. Although 1 patient had good initial response with combination therapy, he is still having secondary infections.
The choice of the best therapeutic agent for conidiobolomycosis, its dosage, and duration remain unclear. 2 There is no single antifungal agent with reliable consistent antifungal activity toward conidiobolomycosis. 5 According to recent antifungal susceptibility studies, multidrug resistant Conidiobolus spp have been identified, and in vitro susceptibility testing may be helpful in guiding therapy. 8 For example, the geometric mean MIC values for Conidiobolus spp. obtained by the susceptibility testing performed by Guarro et al on Conidiobolus spp. isolates are as follows: itraconazole, 11.3 L µg/mL; ketoconazole, 20.7 L µg/mL; miconazole 11.3 L µg/mL; amphotericin B, 3.1 L µg/mL; fluconazole, 107.5 L µg/mL; and flucytosine, 234.6 L µg/mL. 5 Different antifungals like itraconazole, cotrimoxazole, ketoconazole, amphotericin B, and terbinafine are used in treatment with variable success. 5,6
According to reports, this condition could respond to oral itraconazole (200-400 mg/d), ketoconazole (200-400 mg/d), amphotericin-B, and clotrimazole.1,2 Itraconazole is an effective and relatively safe antifungal drug giving satisfactory results. 2 However, antifungal sensitivity for amphotericin B has demonstrated both sensitive and resistant patterns. 6 Clinical failure has been reported with amphotericin B, and it is usually not considered as first choice for treatment. 5,6
Favorable in vivo responses to combination therapy have been reported in the literature. 6,9 It is reported that the combination therapy with azoles and potassium iodide gives rapid and long-lasting results. 2 Both iraconazole (200-400 mg/d) and potassium iodide (40 mg/kg/d) seem reasonable first-line choices for conidiobolomycosis. 5
Since surgical resection may enhance the spread of infection, it is not usually recommended. 2 However, surgical debridement of paranasal sinuses followed by antifungal therapy has been proved to be effective in some case reports. 1,6 For example, in case 3, surgical debulking appeared to be a treatment success and helped with improvement in cosmetic outcome too. According to most case reports, cryotherapy has shown little success. 2
There is no recommended duration for the antifungal treatment. 2 However treatment must be continued for long periods until a negative mycological examination and a good clinical response is achieved. 2,5,6 Some authors suggest that treatment should be continued for at least 1 month after the lesions have cleared. 6 However, even after successful treatment, relapses are common with this chronic disfiguring disease. 2
Conclusion
Conidiobolomycosis is a chronic, localized, rhinofacial subcutaneous mycosis caused by fungi of genus Conidiobolus. It can cause severe facial disfigurement, and disseminated, fatal conidiobolomycosis cases have been reported rarely. There is no single antifungal agent with reliable, consistent antifungal activity against conidiobolomycosis, and it often requires long-term antifungal treatment. The awareness of existence of this clinical entity will lead to early and accurate diagnosis of the condition, reducing the disease-associated morbidity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.