
Abstract
Objectives:
To compare the 2 long-term medical strategies in chronic rhinosinusitis without nasal polyps (CRSnNP) and to identify the role of gastroesophageal reflux disease (GERD) and Helicobacter pylori as factors of treatment failure.
Material and Methods:
Fifty-seven patients with CRSnNP were randomized into 2 therapeutic groups. The first group was treated with 4 weeks of amoxicillin/clavulanate and a short course of oral steroids. The second group received 8 weeks of clarithromycin. Sinonasal Outcome Test-20 (SNOT-20) and Lund and Mackay scores were assessed at baseline and after treatment, and GERD Health-Related Quality of Life (GERD-HRQL) questionnaire was evaluated in all patients. Patients with a GERD-HRQL score >8 received esogastroscopy and H pylori detection. Patients were followed during a 10-year period for clinical course and GERD evolution. The 10-year evolution of patients was described in terms of recurrence, medical, and surgical treatments.
Results:
Thirty-seven patients completed the study; SNOT-20 and Lund and Mackay scores similarly improved in both groups. Amoxicillin/clavulanate group had significantly more adverse reactions than the clarithromycin group (P = .03). After the therapeutic course, 35% (amoxicillin/clavulanate) and 41% (clarithromycin) of patients needed functional endoscopic sinus surgery (FESS). During the long-term follow-up, 54% (amoxicillin/clavulanate) and 40% (clarithromycin) of patients had late CRSnNP recurrence; FESS was performed in less than 15% of cases of recurrence. Gastroesophageal reflux disease complaint’s severity was associated with late recurrence of CRSnNP.
Conclusion:
Amoxicillin/clavulanate and clarithromycin would be competitive treatments for CRSnNP. Gastroesophageal reflux disease seems to be a negative factor for treatment response and recurrence.
Keywords
Introduction
Chronic rhinosinusitis (CRS) is the most prevalent chronic illness in adults aged <45 years, affecting nearly 5% to 15% of the European population and 12% to 16% of the US population. 1,2 Chronic rhinosinusitis has a great economic impact on society in terms of direct and indirect costs, which are estimated to be from $10 to $20 billion per year in the United States. 2 -4 From a clinical perspective, CRS involves the presence of 2 or more symptoms, including nasal obstruction and anterior or posterior nasal discharge for at least 12 weeks. Facial pain/pressure and dysosmia may be associated with these main complaints. 4 Clinically, CRS can be subdivided into CRS with nasal polyps and CRS without nasal polyps (CRSnNP); CRSnNP is related to a ciliary dysfunction resulting in secretion stasis and bacterial buildup, which exacerbate inflammation. 4 The ostiomeatal complex plays a key role in the pathogenesis of CRSnNP since its obstruction results in reduction of sinus ventilation, stasis of bacterial and mucopurulent secretions, and worsening of the mucosal thickening. The cofactors contributing to the mucosal inflammation and the development of CRSnNP include anatomical factors, immunoallergic reactions, tobacco smoke, immune deficiency, and gastroesophageal reflux disease (GERD). 5,6 The relationship between GERD and CRSnNP has long been controversial as well as the relation between H pylori infection and CRSnNP, although some evidences support an involvement of GERD in the development of CRSnNP. 7,8 Moreover, a few studies observed that GERD could contribute to the resistance of some patients with CRSnNP to conventional medical treatments. 9 -11 However, there are no data exploring the long-term evolution of patients treated for CRSnNP according to the presence of GERD and H pylori.
Currently, the most effective treatment for CRSnNP has not been fully identified. Indeed, the few prospective trials that have studied different medical therapeutic schemes in CRS have reported mixed results. 12 -16 Subramanian et al have shown that intensive medical treatments consisting of 1 month of antibiotics (14 different antibiotics alone or in combination), a short course of oral steroids and nasal steroids are associated with clinical and radiological improvements in approximately 90% of cases. 12 Moreover, with regard to the immunomodulatory effect of macrolides, other authors have used clarithromycin or roxithromycin without oral steroids for the treatment of CRSnNP and have reported interesting results. 14 -16 Despite these findings, a large number of physicians usually use amoxicillin/clavulanate associated with oral corticosteroids and recommend macrolides for patients with CRSnNP only after other treatments have failed. 17 However, to date, there is a lack of prospective randomized studies that are aimed at comparing these 2 main long-term antibiotherapies.
The objectives of this study were to compare 2 long-term medical strategies in treating CRSnNP with a short- to long-term follow-up and to assess the impact of GERD and H pylori infection in both the therapeutic response to medical treatment and recurrence.
Materials and Methods
Ethical Considerations
The protocol of the study (including long-term follow-up) has been approved by the CHU Saint-Pierre ethics committee (B07620072452).
Patient Recruitment
From September 2007 to September 2008, we prospectively recruited 57 outpatients with CRS-related symptoms at the Department of Otolaryngology, Head and Neck Surgery of CHU Saint-Pierre, Brussels, Belgium. The CRS diagnosis was based on the definition of the European Position Paper of Rhinosinusitis and Nasal Polyps 2007 (EPOS 2007), in which CRS is defined as inflammation of the nose and the paranasal sinuses characterized by 2 or more symptoms; one of which should be either nasal blockage/obstruction/congestion or nasal discharge (anterior/posterior nasal drip); ±facial pain/pressure; ±reduction or loss of smell; and either endoscopic signs of polyps and/or mucopurulent discharge primarily from the middle meatus; and/or edema/mucosal obstruction primarily in the middle meatus; and/or computed tomography (CT) changes showing mucosal changes within the ostiomeatal complex and/or sinuses. 5 Patients with the following criteria were excluded: history of cystic fibrosis, tobacco smoke, immune deficiency, allergic fungal sinusitis, nasal polyposis, age younger than 18 years, pregnancy or breastfeeding, and allergy or adverse interactions to penicillin or macrolides. Of the 57 patients, 37 completed the study, and 20 were excluded for many reasons, including absence from medical appointments at the end of the treatment or during the follow-up period (N = 12), absence of any CRS radiographic lesions on the sinus CT, odontogenic CRS, CRS with nasal polyposis, and stopping of treatment during the treatment period. The remaining 37 patients were followed for 10 years after the completed treatment.
Study Protocol, Randomization, and Treatment
Patients were randomized into 2 groups according to the proposed treatment. Permuted block randomization method was applied to generate randomization codes. Consort guidelines for reporting randomized controlled trials (RCTs) were followed. The first group received amoxicillin/clavulanate (875 mg, twice daily for 4 weeks) with degressive oral steroids (methylprednisolone, 32 mg daily for 5 days followed by 16 mg daily for 5 days), intranasal steroids (mometasone furoate, twice daily), and saline solution (6 times daily) for 8 weeks. The second group received 8 weeks of clarithromycin (500 mg daily for 2 weeks followed by 250 mg daily for 6 weeks) with the same topical intranasal treatment used for group 1. The positive response to treatment was defined by an improvement of patient’s symptoms and CT-scan findings (total Lund and Mackay score ≤1).
A surgical procedure (functional endoscopic sinus surgery [FESS]) was proposed to patients with uncontrolled/recurrent complaints supported by a Lund and Mackay score >1 at the end of the treatment period. Depending of the impaired sinus, FESS included maxillary sinus meatotomy or anterior or posterior ethmoidectomy. Frontal meatal antrostomy and sphenoidotomy were made for patients with frontal or sphenoid recurrent rhinosinusitis, respectively. Recurrence was defined as the occurrence of clinical CRS including symptoms and signs (EPOS 2007) in a context of CT-scan findings (Lund and Mackay score ≥1). Late recurrences during the 10-year follow-up period were treated with short-term antibiotics (7 days), intranasal corticosteroids, and saline solution for 4 weeks. In cases of resistance to medical treatment, FESS was proposed. Time to relapse was defined as the time interval after antibiotic treatment at which a recurrence of symptoms necessitated the reinstitution of antibiotics and/or oral steroids. Figure 1 illustrates the flow chart of the study.
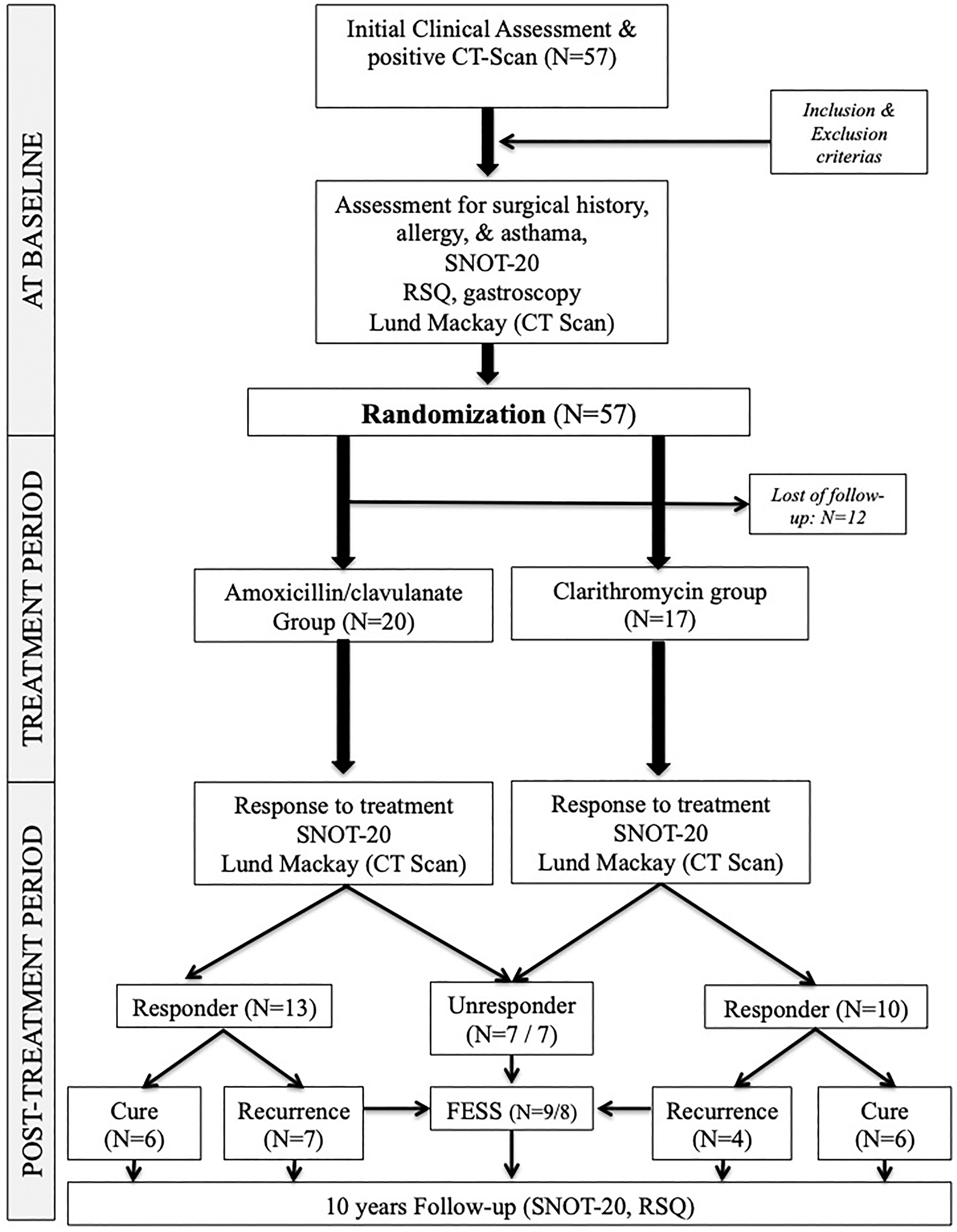
Flow chart of the study. FESS indicates functional endoscopic sinus surgery; RSQ, reflux symptoms questionnaire; SNOT-20, 20-item sinonasal outcome test.
Clinical Evaluations and Subjective and Objective Assessments
Sinonasal complaints and allergies
The CRS-related symptoms of patients were assessed with the Sinonasal Outcome Test-20 (SNOT-20) questionnaire 18 at baseline (t0), at the end of the treatment (t1), and 10 years after the initial diagnosis (t2), irrespective of the realization of FESS. At baseline, allergy was evaluated in all patients with skin prick tests. In cases of allergy, a long-term adequate treatment (antihistamine and lifestyle recommendations) was administered. We did not perform sublingual immunotherapy in this study.
Sinonasal imaging
The CT-scan findings were characterized at baseline (t0) and after the treatment period (t1) using the Lund-Mackay CT-scoring system. 19
Gastroesophageal reflux disease
Because GERD is a factor of resistance to treatment, 9 -11 we assessed the occurrence of GERD symptoms at baseline in both groups; and, irrespective to the type of antibiotic, we studied the response to treatment throughout the long-term follow-up regarding the GERD status. Symptoms of GERD were rated in all patients with the GERD Health-Related Quality of Life (GERD-HRQL) questionnaire 20 at baseline (t0), along and at the end of the study (t2). The GERD-HRQL questionnaire is a validated 16-item scale that is rated from 0 (no symptom) to 80 (maximal disability). Symptoms include both gastroesophageal and extraesophageal manifestations of GERD, including (among others) heartburn, regurgitation, odynophagia, throat pain, dysphagia, and abdominal complaints. A total score ≥8 is suggestive of GERD. 21 In the present study and according to recommendations, 21 patients with GERD HRQL score ≥8 received additional examinations including esogastroscopy and gastric biopsies to detect H pylori. With regard to this procedure, we studied the relationship between GERD (symptoms and esogastroscopy), H pylori infection, and some CRSnNP findings including SNOT-20 (t0, t1, t2), Lund and Mackay score (t0, t1), immediate or late recurrence, and FESS.
Statistical Analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences for Windows (SPSS v22.0; IBM Corp, New York). No prior power analysis was performed. The following statistical tests were used: Wilcoxon signed-rank test (pre/post comparisons of SNOT-20; GERD-HRQL; and Lund-Mackay scores), Mann-Whitney test (comparison between groups), and Spearman correlation test (correlations between GERD and CRSnNP characteristics). A level of significance of 0.05 was adopted.
Results
Patient Characteristics
Thirty-seven patients completed the study. Twenty patients were excluded including 12 who were lost to follow-up. The epidemiological characteristics (ie, age, gender, clinical cofactors, adverse reactions, and treatment efficiency) of patients according to the therapeutic group are available in Table 1. No significant difference was found between the 2 groups regarding the baseline clinical data for any of the following items: age, gender, allergy, asthma, surgical history, esophagitis, H pylori infection, and pretherapeutic SNOT-20, GERD-HRQL, and Lund-Mackay scores.
Characteristics of Patients According to the Therapeutic Group.
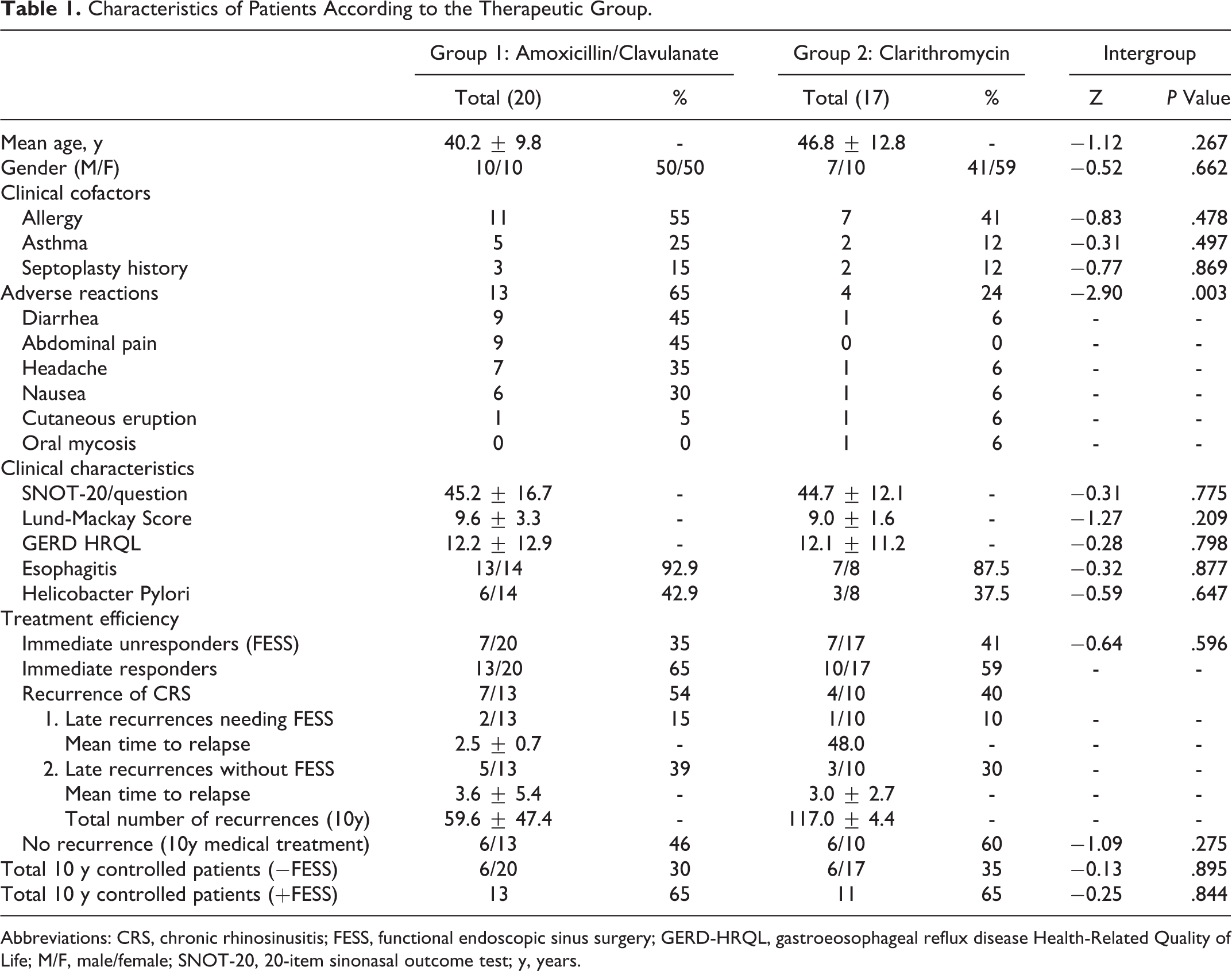
Abbreviations: CRS, chronic rhinosinusitis; FESS, functional endoscopic sinus surgery; GERD-HRQL, gastroeosophageal reflux disease Health-Related Quality of Life; M/F, male/female; SNOT-20, 20-item sinonasal outcome test; y, years.
Short-Term Evaluations of Medical Treatments
The mean values of the SNOT-20 and Lund-Mackay scores significantly decreased from baseline (t0) to post-treatment (t1) in both groups (Tables 2 and 3). According to the Mann-Whitney test, we did not find a significant difference between groups at t1 for both SNOT-20 and Lund-Mackay scores. The treatment response rates of groups 1 and 2 were 65% and 59%, respectively; the difference was not statistically significant. With regard to these data, 35% of patients in group 1 and 41% of patients in group 2 were considered as immediate nonresponder patients and benefited from FESS. However, patients of group 1 (amoxicillin/clavulanate) had a significant higher rate of adverse reactions compared to patients of group 2 (clarithromycin group), including diarrhea, nausea, headache, cutaneous reaction, and abdominal pain.
Pre- and Posttreatment Clinical and Radiological Assessments in Patients With CRS Treated With Amoxicillin/Clavulanate.
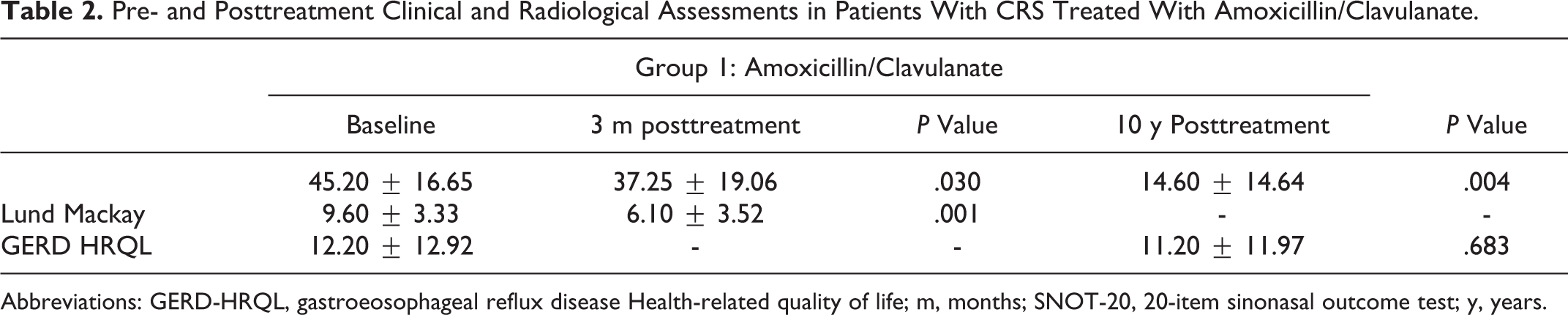
Abbreviations: GERD-HRQL, gastroeosophageal reflux disease Health-related quality of life; m, months; SNOT-20, 20-item sinonasal outcome test; y, years.
Pre- and Posttreatment Clinical and Radiological Assessments in Patients With CRS Treated With Clarithromycin.
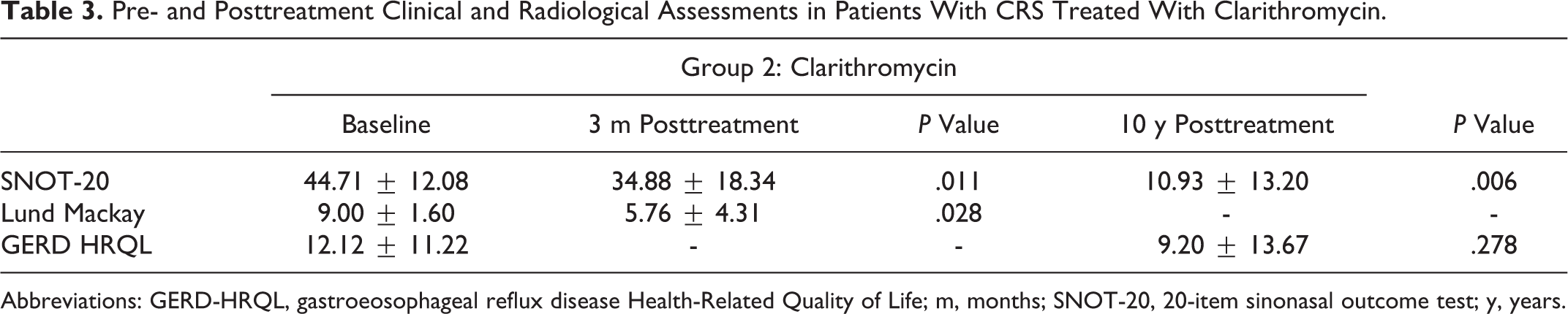
Abbreviations: GERD-HRQL, gastroeosophageal reflux disease Health-Related Quality of Life; m, months; SNOT-20, 20-item sinonasal outcome test; y, years.
Long-Term Evaluations of Medical Treatments
The mean SNOT-20 values significantly improved from t1 to t2 in both groups, without any significant difference between groups (Figure 2). Because the immediate and late success rates of both medical treatments are comparable, the analysis of long-term evolution was made on the entire cohort. However, details of each group are available in Table 1.
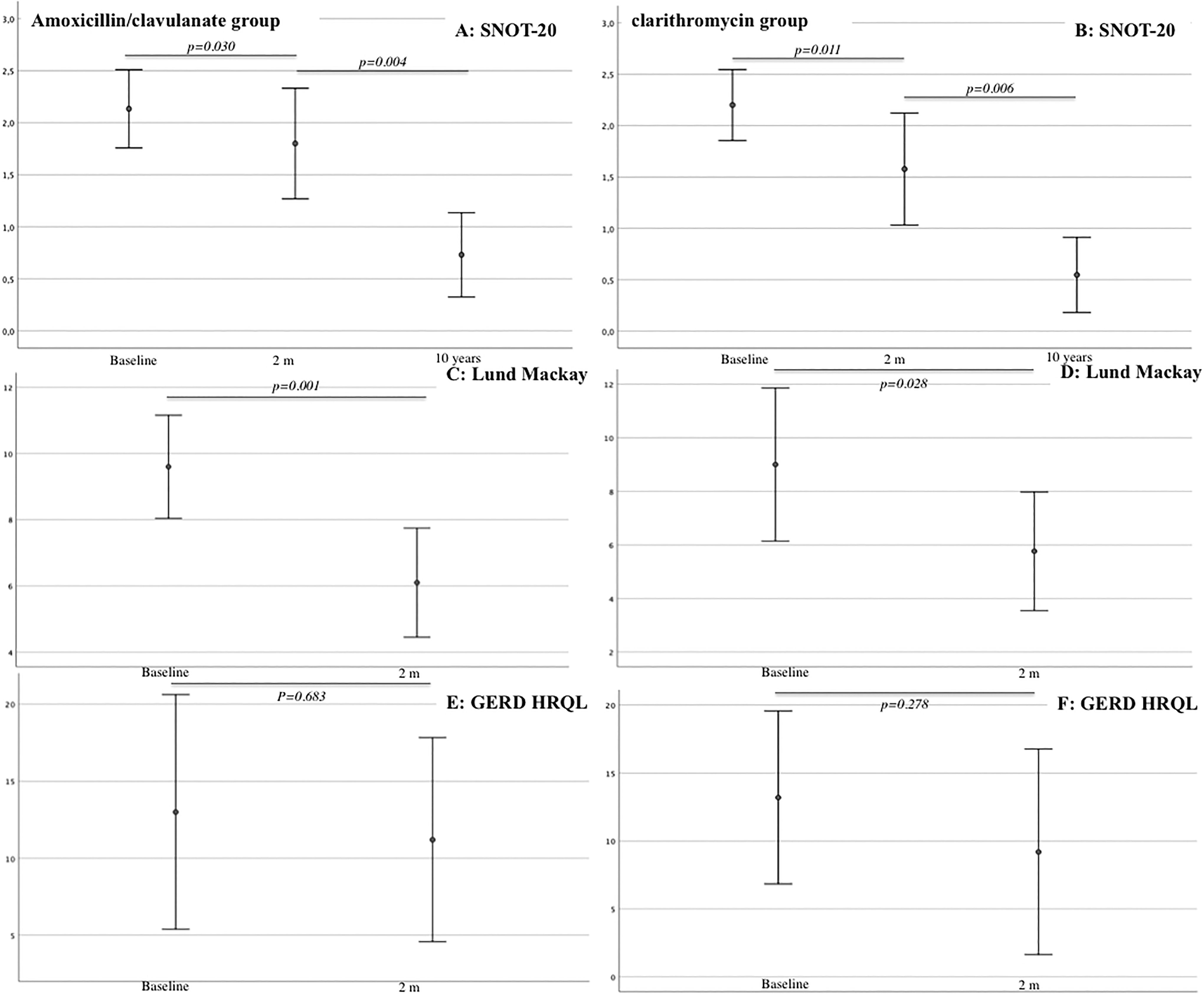
Illustration of objective and subjective evolutions of CRS and GERD assessments according to the group. GERD-HRQL indicates gastroeosophageal reflux disease Health-Related Quality of Life; m, months; SNOT-20, 20-item sinonasal outcome test; y, years.
Overall, among the 23 immediate responder patients, 3 required FESS for recurrent CRSnNP (13%), 8 patients had late recurrence episodes responding to medical treatments (35%), and 12 patients were free of disease 10 years after the initial diagnosis (52%). In summary, excluding FESS, the clinical and radiological findings of 46% of patients of group 1 and 60% of patients of group 2 were well-controlled over the long term (Table 1; P = .275), and irrespective of the medical treatment, 38% of patients needed immediate or late FESS (N = 14/37). Two patients in each group had >1 FESS.
Evaluation of GERD
The GERD-HRQL questionnaire was completed by patients at t0 and t2. At baseline, the mean value of GERD-HRQL of group 1 was 12.2 ± 12.9 and 11.2 ± 12.0 at t2. The mean value of GERD-HRQL of group 2 was 12.1 ± 11.2 at baseline and 9.2 ± 13.7 at t2. There was no significant difference from baseline to t2 in both groups (Tables 2 and 3).
Among the patients with a GERD-HRQL score ≥8 (N = 23/37), 91% (N = 21/23) had esophagitis ranging from grade A to C (12 cases of grade A, 5 cases of grade B, and 1 case of grade C). Patients with esophagitis were treated by once daily pantoprazole (20 mg) for 3 months. Diet and behavioral changes were proposed to these patients as a long-term treatment and they were followed in gastroenterology department. In case of recurrence(s) of GERD symptoms, they received a new therapeutic line (once daily pantoprazole and diet for 3 months). Of 23 gastric biopsies, 9 histological specimens were positive for H pylori (Table 1). The H pylori was treated with pantoprazole (40 mg/d) and the antibiotics prescribed for the treatment of CRSnNP. Ten years after the diagnosis, of the 23 patients with initial GERD, 9 patients needed long-term treatment with proton pump inhibitors (39.1%) because of recurrent GERD complaints. Among the 14 patients without GERD-related symptoms at t0, 4 had GERD diagnosed during the 10-year follow-up period with GERD-HRQL and positive esophagitis (28.6%).
Association Between GERD and CRS Characteristics
At diagnosis, our correlation analysis found significant correlations between GERD-HRQL and SNOT-20 scores (r s= 0.569, P = .010). According to Spearman analysis, the GERD-HRQL score severity at baseline was significantly associated with the late CRSnNP recurrence requiring FESS (r s= 0.749, P = .002). The presence of H pylori infection was associated with the posttreatment SNOT-20 (t1, r s= 0.525, P = .012) and the realization of immediate FESS (r s = 0.585, P = .036, Table 4).
Correlation Analysis Between GERD and CRS Characteristics.
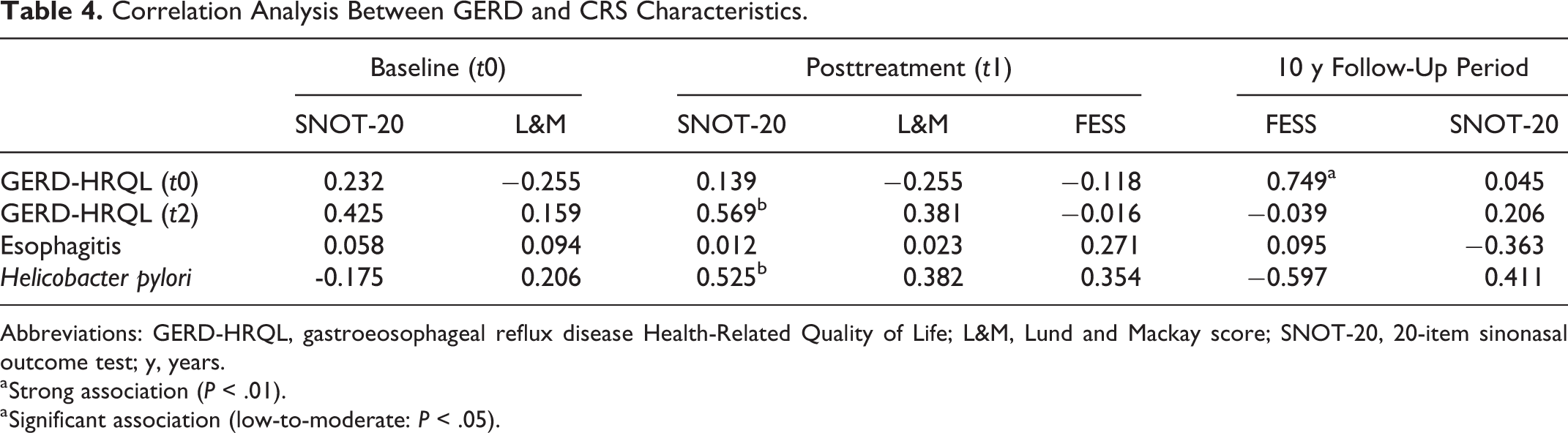
Abbreviations: GERD-HRQL, gastroeosophageal reflux disease Health-Related Quality of Life; L&M, Lund and Mackay score; SNOT-20, 20-item sinonasal outcome test; y, years.
a Strong association (P < .01).
a Significant association (low-to-moderate: P < .05).
Discussion
To the best of our knowledge, this is the first RCT to compare the short- to long-term effects of a macrolide versus amoxicillin/clavulanate in patients with CRSnNP. Initially, the 2007 European Position Paper did not systematically suggest oral steroids but proposed a long course of macrolides with an intranasal saline rinse and topical steroids in moderate and severe CRS. 5 This position was supported by several studies that demonstrated the immunomodulatory effect of macrolides in addition to their antibiotic effect, but a controversy persists about the therapeutic superiority of macrolides to amoxicillin/clavulanate treatment associated with methylprednisolone. 13 -16
In the first part of this study, we compared the efficacy of a treatment based on amoxicillin/clavulanate and methylprednisolone with the use of clarithromycin. In the short-term follow-up, our results clearly suggest that these 2 long-term medical treatments are quite competitive, exhibiting significant improvements in clinical and radiological findings and a similar immediate surgical rate for recurrent CRSnNP. To date, although there were many studies comparing these 2 antibiotic regimens in the management of acute rhinosinusitis, 22 -24 no study has been specifically conducted on CRSnNP, limiting our literature comparison. On the other hand, some trials have studied the effectiveness of both macrolides and amoxicillin/clavulanate treatments in CRSnNP independently of one another. Thus, in a double-blinded placebo-controlled trial, Sabino et al found that a CRS treatment based on the combination of 2 weeks of amoxycillin/clavulanate, nasal irrigations, and intranasal corticosteroids was associated with a significant improvement in the SNOT-22 score at 12 weeks and a success rate from 45% to 50%. 25 The comparison with our study can be biased because the therapeutic period of that investigation was shorter than that of our study (2 vs 8 weeks). In addition, the researchers included patients with CRS and nasal polyps, and the success rate criteria were based only on the endoscopic clinical findings. In a retrospective study of 40 patients, Subramanian et al studied the effectiveness of 4 weeks of antibiotic(s) associated with a short course of oral steroids, 8 weeks of nasal irrigations, and intranasal corticosteroids. Using mainly amoxicillin/clavulanate as the antibiotic treatment, these authors reported that 65% of patients had sustained symptomatic benefits beyond 8 weeks after initial treatment, corroborating our results. 12 However, for 17 patients, the authors combined 2 or more antibiotics, including a macrolide, which can have an impact on the clinical course regarding the immunomodulatory effect of these antibiotics. In addition, a large number of studies were published concerning the efficiency of a low dose of macrolides for CRS treatment. Among those that studied patients with CRSnNP, the use of macrolide for 8 or 12 weeks seemed to improve the SNOT-20 score 12 weeks after the initiation of treatment. 16,26 Finally, in the randomized study of Zeng et al, the patients treated with clarithromycin for 12 weeks reported a significant improvement on a visual analog scale of subjective symptoms after 4 weeks of treatment. 27 Interestingly, these authors reported a similar improvement in the control group where patients received only an intranasal corticosteroid spray. None of these 3 trials studied the evolution of the CT-scan findings along the therapeutic course. Overall, even if we focus our comparison on group data, it is still difficult to compare our findings with the current literature with regard to the discrepancies in the therapeutic regimens, outcomes, and inclusion criteria of the clinical populations. In light of our results, however, we suggest the use of long-term clarithromycin therapy as the choice for CRS treatment on the basis of the high prevalence of adverse effects in the amoxicillin/clavulanate group and the published, well-demonstrated low rate of adverse effects of macrolide treatment. 17 However, in the future, it could be interesting to assess both the efficiency and the adverse effects of a shorter period of amoxicillin/clavulanate in comparison with long-term macrolides. It is probable that our high rate of adverse effects is due to the antibiotic intake for such a long period (4 weeks) but we cannot exclude the impact of the corticosteroid intake in the amoxicillin/clavulanate group.
In the second part of this study, we evaluated the evolution of patients over a 10-year follow-up period. To our knowledge, this study is the first to prospectively provide such a long follow-up of patients initially treated for CRSnNP. In the current literature, the long-term follow-up studies mainly focus on CRS with nasal polyposis or CRS treated by surgery but not specifically on CRSnNP. 28 -30 In summary, we observed that 54% and 40% of responder patients in the amoxicillin/clavulanate and clarithromycin groups, respectively, had early or late recurrence of CRS and a few needed delayed FESS. Among the total number of patients included in the study, the initial medical treatment of 30% and 35% of patients in the amoxicillin/clavulanate and clarithromycin groups was sufficient to significantly control the clinical and radiological findings. These data qualify the initial success rates of 65% (amoxicillin/clavulanate) and 59% (clarithromycin) that were observed at the end of the treatment and strengthen the need to inform patients about the risk of recurrence after the completion of medical treatment. Moreover, our findings have the merit of highlighting the high number of (well-treated) recurrences of CRS over the long-term follow-up period but the low rate of recurrence requiring FESS to control the clinical and radiological findings of the patient.
The third part of this study aimed to investigate the impact of GERD and H pylori infection on CRSnNP. On the one hand, our study revealed positive correlations between the severity of GERD complaints, SNOT-20 scores, and late recurrence of CRSnNP requiring FESS. On the other hand, we observed significant associations between H pylori infection, SNOT-20 severity at the end of the treatment, and the need for immediate FESS.
The association between GERD, extraesophageal reflux (laryngopharyngeal reflux, LPR), and CRSnNP has long been suspected in both adults and children. 7,31,32 Our results corroborate those of other trials that suggested a key role of GERD in the recurrence of CRSnNP. Indeed, it has been recently demonstrated that compared to healthy volunteers, patients with recurrent CRSnNP have more LPR complaints, esophageal reflux events, and impaired pH-metry findings. 33 These findings and our observations can be explained by the irritative potential of the back flow of gastric contents into the upper aerodigestive tract (including nasal) mucosa. Thus, pepsin and other gastroduodenal enzymes may maintain the inflammatory reaction of the mucosa, 34 reducing the efficiency of anti-inflammatory effect of macrolide or methylprednisolone and leading to the persistence of inflammation, symptoms, and CRS. 32 First, it is important to keep in mind that patients with GERD complaints have a higher probability of also experiencing gaseous gastric reflux episodes (LPR) that lead to irritation of the upper aerodigestive mucosa. Second, patients with GERD and LPR have not necessary esophagitis, which may explain our lack of correlation between esophagitis severity and recurrence items.
Finally, the association between H pylori and CRS has been suggested by many authors but is still unclear. 35 As reported in a recent review, 7 some studies have identified H pylori in both stomach and nasal mucosa of patients with CRS that could explain our findings. Thus, it could be possible that the chronic nasal inflammatory reaction of H pylori would be associated with high SNOT-20 score posttreatment but this hypothesis remains theoretical and needs future researches.
This study has several weaknesses. First, the low number of patients, which is mainly related to the duration of the follow-up period, may reduce the statistical power of the study and may limit the generalization of results. No prior power analysis was performed. Second, according to the anti-inflammatory effect of macrolides, we only used methylprednisolone in the amoxicillin/clavulanate group, which may have biased the clinical and radiological comparisons between groups. However, currently, oral corticosteroids used as an adjunct therapy to antibiotics or intranasal corticosteroids may improve symptom severity, polyp size, and CT-scan findings, but the quality of the evidence supporting their systematic utilization is still very low. 36 Third, we did not use pH-impedance metry to confirm the presence of LPR. The addition of this examination would have improved the diagnosis; but in our country, it is still expensive, not reimbursed by the health-care system, and less used by otolaryngologists regarding high false-positive and false-negative rates, interpretation difficulties, inconsistency between pH findings, signs, and symptoms. 37,38 Finally, with regard to the involvement of H pylori in recurrent CRS, an analysis of the bacteria in nasal mucosa of patients with recurrent CRS would have been useful.
Conclusion
Amoxicillin/clavulanate and clarithromycin treatments could be competitive therapeutic regimens in terms of clinical and radiological improvements in CRSnNP over both the short and long terms. Amoxicillin/clavulanate has, however, more side effects than clarithromycin. Helicobacter pylori infection and the presence of severe GERD complaints at baseline seem to be associated with high SNOT-20 score posttreatment (H pylori); recurrence of CRSnP, resistance to medical treatment, and the related need for early or late FESS. The control of GERD and H pylori infection along the long-term follow-up of patients is highly recommended.
Footnotes
Acknowledgments
The authors thank American Journal Expert for the proofreading of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.