
Abstract

Desmoid-type fibromatosis is a locally aggressive, nonmetastasizing, well-differentiated, unencapsulated monoclonal myofibroblastic proliferation with a tendency for local invasion and recurrence. The tumor is intermediate between a fibroma and fibrosarcoma. Without a well documented etiology, trauma, surgery, and mutations in the CTNNB1 gene have all been implicated.
About 15% of all desmoid-type fibromatosis develops within the head and neck, with maxillary sinus and mandible most frequently affected. Young males are affected slightly more often than females, although all ages can be affected. Symptoms are nonspecific, with nasal obstruction, epistaxis, and a mass most common. Complete surgical excision is the treatment of choice, although margins are often positive, associated with recurrences, while targeted receptor tyrosine kinase inhibition shows promise.
The lesion presents as a tan-white, rubbery firm mass, often with infiltrative borders. Histologically, the neoplastic cells expand into the adjacent tissues, showing a low to moderate cellularity, arranged in broad fascicles of bland-looking spindle cells arranged in a uniform direction (“purposeful”; Figure 1). Elongated blood vessels are frequently observed running parallel to the fiber direction. The spindle cells have a myofibroblastic appearance, with a low nuclear to cytoplasmic ratio and uniformly bland ovoid nuclei with indistinct nucleoli (Figure 2). Collagenized background stroma may be seen, focally assuming a myxoid appearance. By immunohistochemistry, there is a characteristic strong, nuclear β-catenin reaction (Figure 2), while actins may also be focally noted. Somatic mutations in the β-catenin (CTNNB1) gene on chromosome 3p21 are detected in most cases. Other lesions in the differential diagnosis which should be excluded include: solitary fibrous tumor (STAT6 positive), glomangiopericytoma (peritheliomatous hyalinization, patternless proliferation, extravasated erythrocytes, and inflammatory cells), perineurioma (EMA, claudin-1, GLUT1 positive), ossifying fibroma, hypertrophic scar, and even chondromyxoid fibroma.
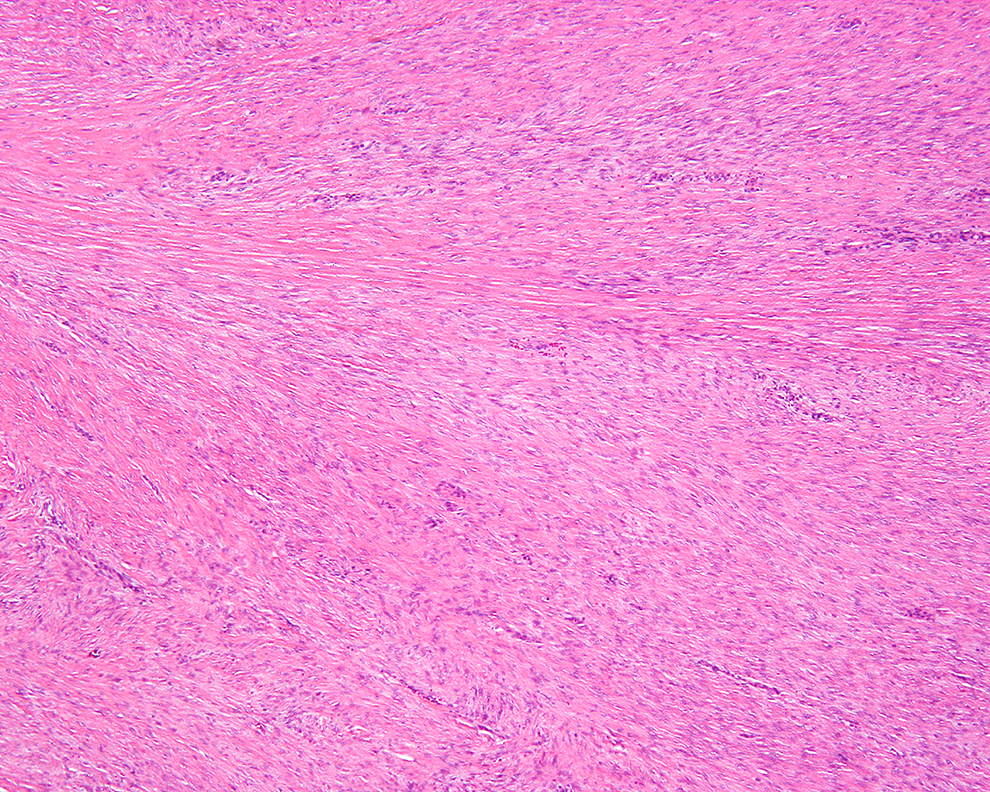
Fascicles of neoplastic fibroblastic cells arranged in a purposeful direction.
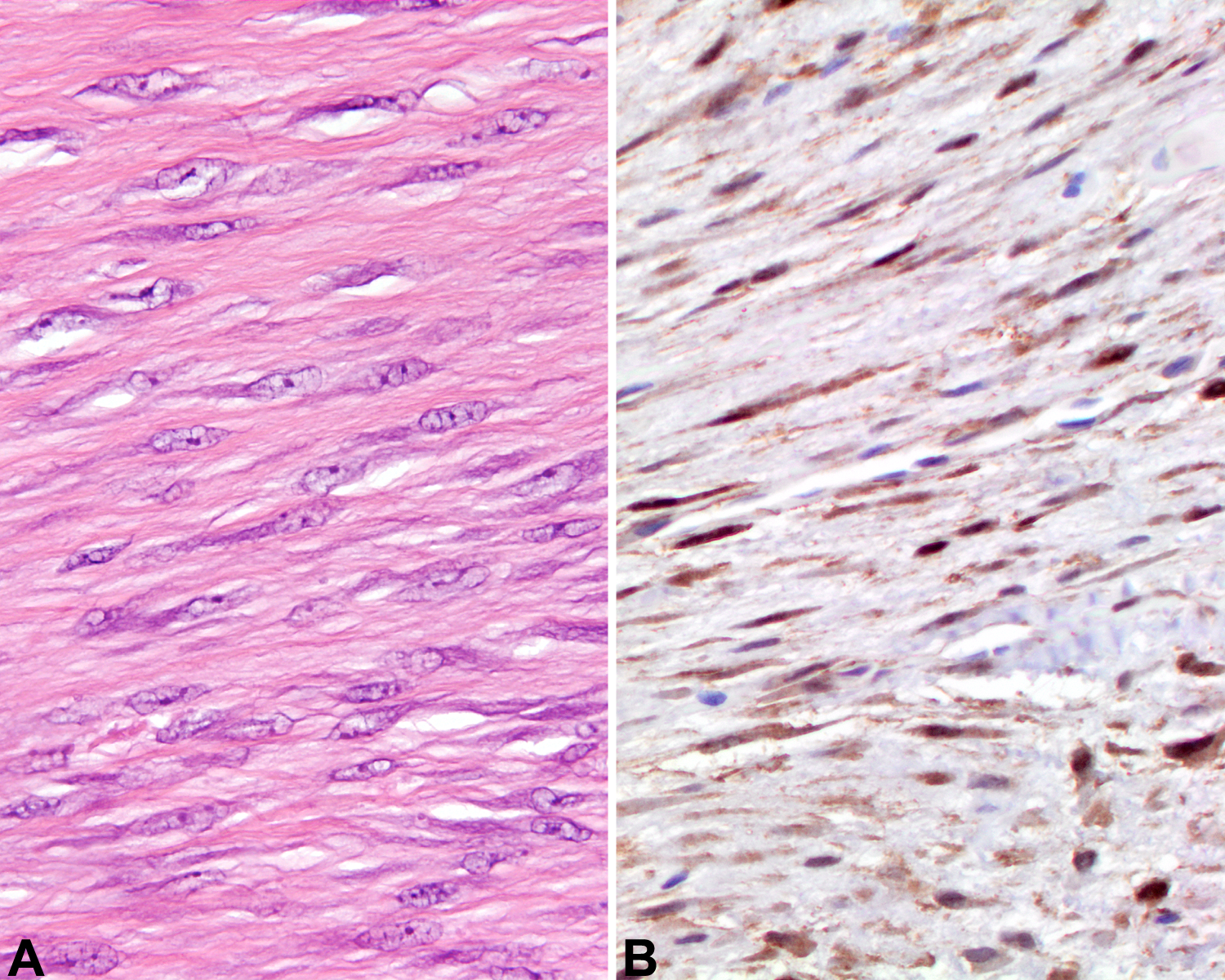
A, Moderately cellular fibroblastic proliferation without pleomorphism. B, The neoplastic cells show a strong nuclear β-catenin immunohistochemical reaction.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.