
Abstract
Objectives:
We evaluated olfactory functions in patients with obstructive sleep apnea (OSA).
Methods:
The cranial magnetic resonance images of 58 adult patients (36 males and 22 females) aged 27 to 79 years were retrieved from the hospital picture archiving and communication system (PACS) system. There were 29 patients with OSA (17 males and 12 females), diagnosed according to the polysomnography results. A control group consisted of 29 healthy patients without OSA. Olfactory bulb (OB) volume and olfactory sulcus (OS) depth measurements were performed. Nasal septal deviation (SD) was also evaluated and recorded as no SD, deviation to the right, and deviation to the left in all groups.
Results:
Olfactory bulb volumes of the OSA group were significantly lower than those of the control group (P < .05), whereas OS depth values were not different (P > .05). There was a positive correlation between the right and left OB volumes and right and left OS depth values (P < .05). In older patients with OSA and in female patients with OSA, OB volumes decreased bilaterally (P < .05). Olfactory sulcus depth of the right side was lower in the female patients with OSA compared to the male patients with OSA (P < .05). There were no significant correlations between apnea–hypopnea index and OB volumes and OS depth values in the OSA group (P > .05)
Conclusion:
In patients with OSA, OB volumes decreased bilaterally. It may be related to intermittent nocturnal hypoxia/reoxygenation episodes, which may be a trigger for upper airway inflammation; and proinflammatory mediators maybe harmful on olfactory neuroepithelium and olfactory impairment may occur.
Keywords
Introduction
Obstructive sleep apnea (OSA) is a breathing disorder during sleep. Obstructive sleep apnea is related to risk factors, such as neurological, cardiac, and morbidities at the perioperative period. 1 The apnea–hypopnea index (AHI) indicates the severity of OSA: normal (AHI < 5/h), mild (AHI ≥ 5 and <15), moderate (AHI ≥ 15 and <30), or severe (AHI ≥ 30). 2,3
Obstructive sleep apnea is characterized by excessive daytime sleepiness, impaired concentration or memory. There were recurrent episodes of apnea or hypopnea, disruptive snoring. Nocturnal hypoxemia, recurrent awakenings, unrefreshing sleep, and daytime fatigue were also seen. Obesity, age, male sex, and heritable factors are risk factors for OSA. 4,5 Obstructive sleep apnea is associated with reduced basal and functional capillarity rarefaction, and the additional risk of impaired peripheral perfusion. 6 In patients with OSA, chronic hypoxemia occurs. 7
Heinzer et al 8 reported that moderate-to-severe sleep-disordered breathing (≥15 events per hour) incidence was 49.7% in males and 23.4% in females. As OSA incidence in the population is higher, we aimed to evaluate olfactory functions in patients with OSA. We measured olfactory bulb (OB) volume and olfactory sulcus (OS) depth on cranial magnetic resonance imaging (MRI) in patients with OSA.
Materials and Methods
This retrospective study was conducted in Kahramanmaras Sutcu Imam University, Faculty of Medicine, Radiology Department according to the principles of the Declaration of Helsinki. Magnetic resonance imaging scans were retrieved from the database of the Kahramanmaras Sutcu Imam University, Faculty of Medicine Radiology Department. Approval for the study was taken from the Clinical Researches Ethics Committee of Kahramanmaras Sutcu Imam University Faculty of Medicine (Date: February 6, 2019, Number: 12, Meeting No: 2019/02).
Patients
This study was performed retrospectively. The cranial MRI images of 58 (36 males and 22 females) adult patients aged 27 to 79 years were retrieved from the hospital picture archiving and communication system (PACS) system up to the current date. There were 29 (17 males and 12 females) patients with OSA, diagnosed according to the polysomnography results (group 1). Their mean AHI was 35.72 ± 20.43 events/h (ranged from 10-80 events/h) and they have not undergone the treatment such as surgery or continuous positive airway pressure. The mean age of the OSA group was 52.51 ± 10.38 years.
A control group consisted of 29 (19 males and 10 females) healthy patients without OSA and their cranial MRI results were normal. Their data were selected from the records in the hospital PACS system as age-matched screening from present to past. The mean age of the control group was 53.00 ± 10.42 years.
In both the OSA and control groups, MRI evaluation was performed mainly because of headache. Exclusion criteria for the study and control groups were marked facial deformity, sinonasal tumors, infections or polyposis, a history of trauma or surgery, multiple sclerosis, cerebrospinal fluid leak, Parkinson disease, or epilepsy. 9
Cranial MRI Measurements
The MRI examinations were performed using 1.5T MRI with a cranial coil (Philips Ingenia 1.5T, Eindhoven 2015, the Netherlands); T2-weighted images in the coronal plane (repetition time [milliseconds]/time echo [milliseconds]: 4833/100, field of view: 220 × 183 mm and matrix 356 × 209 mm) were obtained using 5.5-mm slice thickness and a 1-mm intersection gap and 22 coronal sections were obtained. Measurement results were obtained from coronal T2-weighted images for the standard OB volume and OS depth. 10,11
Olfactory bulb volume measurement was taken on the coronal T2-weighted images. From anterior to posterior screening, “on the image where the OB was seen clearly, the surface of the OB was measured manually by an electronic cursor as mm2, and volume was calculated by multiplying this value by the slice thickness as mm3”(Figure 1). 10,11
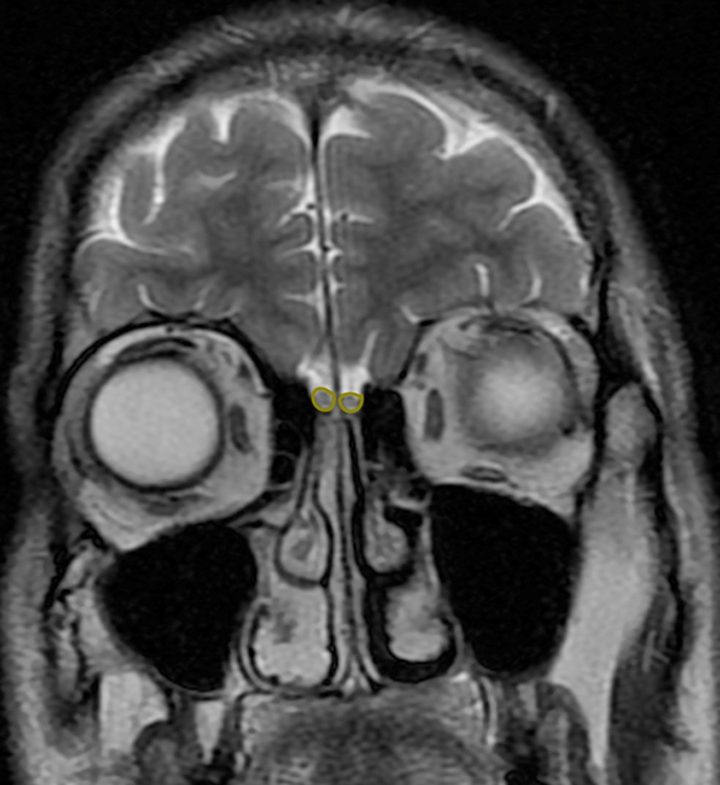
On T2-weighted coronal cranial MRI of the 43-year-old male patient, olfactory bulb (OB) volume is shown. The patient has OSA with AHI = 12 events/h. AHI indicates apnea–hypopnea index; MRI, magnetic resonance imaging; OSA, obstructive sleep apnea.
Olfactory sulcus depth measurement was taken on the coronal T2-weighted images, “a virtual tangent line was drawn from the inferior orbital gyrus to the gyrus recti in the posterior plane of the orbita. A new perpendicular line was drawn from this tangent line to the deepest point of the OS. The length of this line” gives the OS depth in mm (Figure 2). 10,11
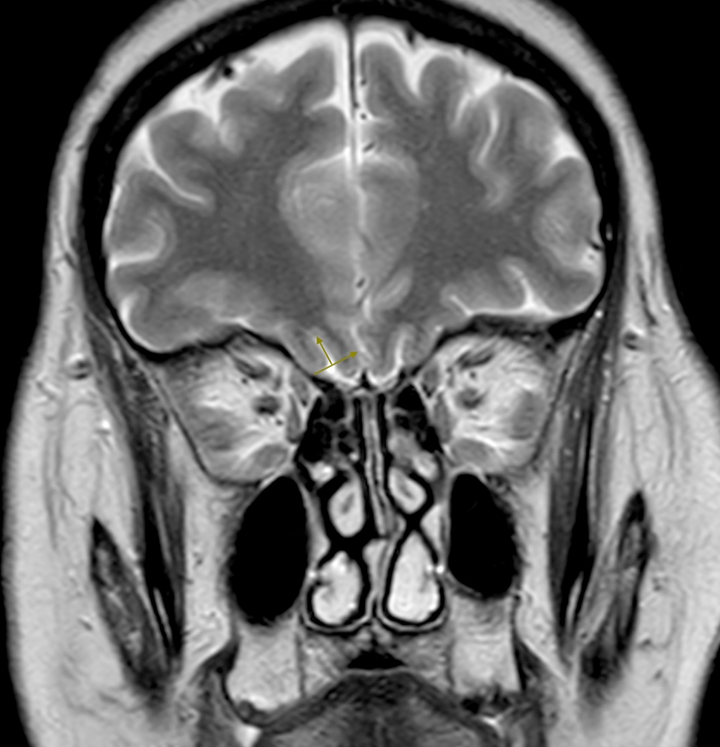
On T2-weighted coronal cranial MRI of the 62-year-old female patient, olfactory sulcus (OS) depth is shown. The patient has OSA with AHI = 50 events/h. AHI indicates apnea–hypopnea index; MRI, magnetic resonance imaging; OSA, obstructive sleep apnea.
Nasal septal deviation (SD) was also evaluated and recorded as no SD, deviation to the right, and deviation to the left in all groups.
Statistical Analysis
The data obtained in the study were analyzed using SPSS for Windows version 16.0 software (SPSS, INC, an IBM Company, Chicago, Illinois). Initially, we used the Kolmogorov-Smirnov test. If the P value was <.05, nonparametric tests were used. If the P value was >0.05, parametric tests were used.
The independent samples t test, paired samples t test, χ2 test, Pearson correlation test, and Spearman correlation rho efficient tests were used. A value of P < .05 was considered statistically significant.
Results
The difference between gender distribution of the OSA and control groups was not statistically significant (P = .588, χ2 = 0.293).
Measurement results for OB volume and OS depth are shown in Table 1. Olfactory bulb volumes of the OSA group (group 1) were significantly lower than those of the control group (group 2) bilaterally (P < .05). There were no significant differences between OS depth values of the OSA and control groups (P < .05; Table 1).
Measurement Results for Olfactory Bulb Volume and Olfactory Sulcus Depth.
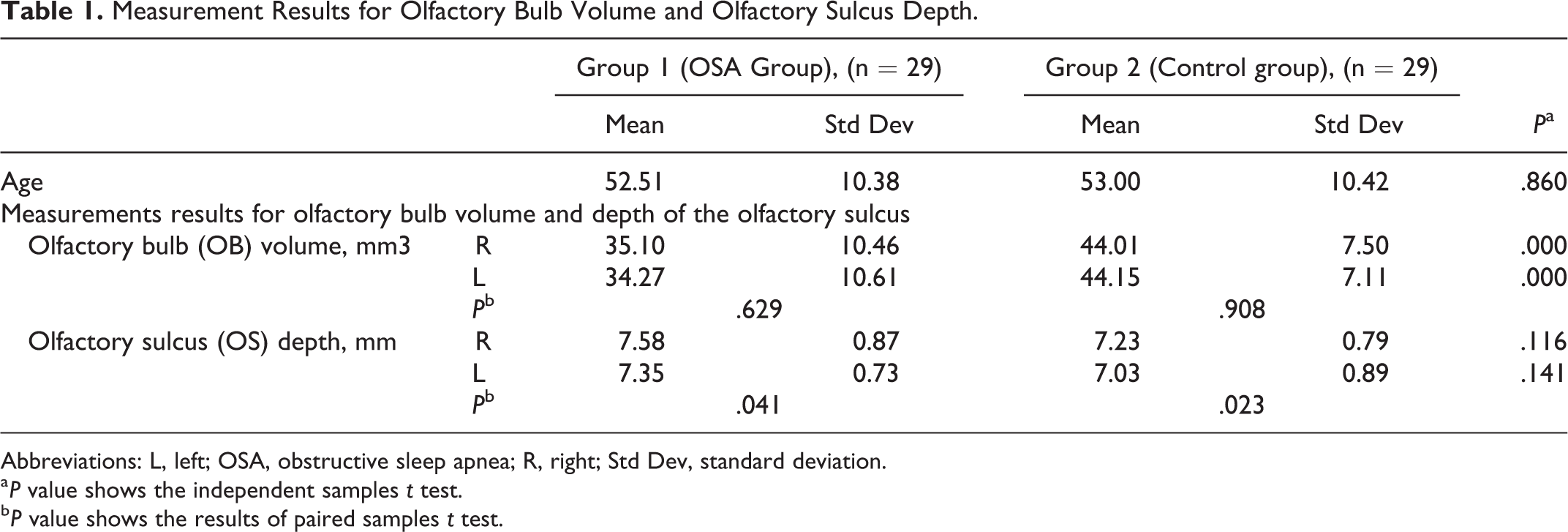
Abbreviations: L, left; OSA, obstructive sleep apnea; R, right; Std Dev, standard deviation.
a P value shows the independent samples t test.
b P value shows the results of paired samples t test.
In the OSA and control groups separately, left OS depth values were significantly lower than right OS depth values (P < .05). Olfactory bulb volumes were not different between the right and left sides of both groups (P > .05; Table 1).
Measurement results for OB volume and OS depth according to the SD (absent or present) in the OSA group are shown in Table 2. Olfactory bulb volume and OS depth values were not found as significantly different between SD present and absent groups bilaterally (P > .05; Table 2).
Measurement Results for Olfactory Bulb Volume and Olfactory Sulcus Depth According to the Septal Deviation (Absent or Present) in the OSA Group.
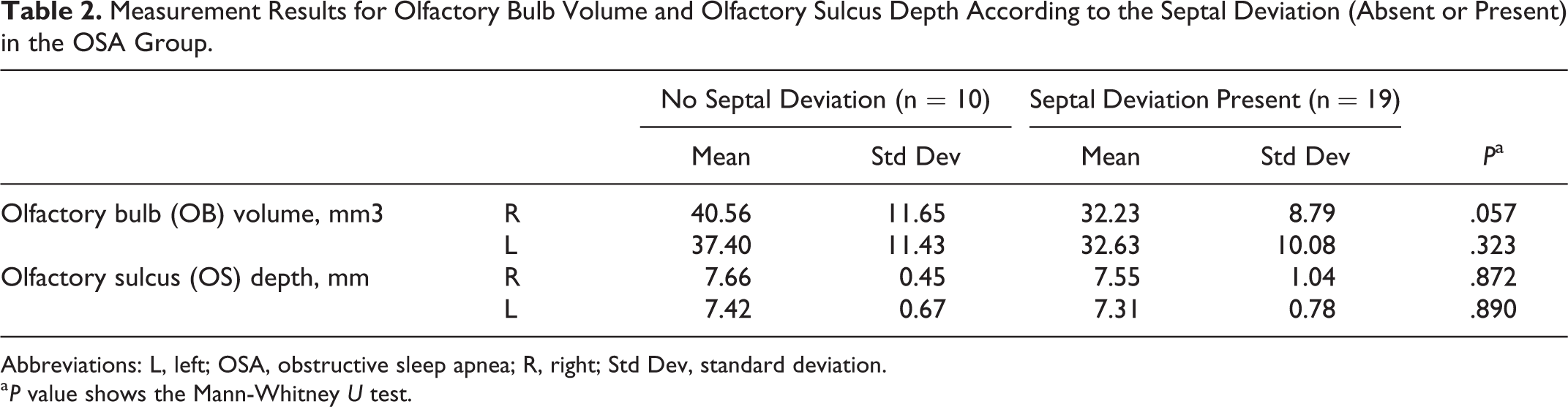
Abbreviations: L, left; OSA, obstructive sleep apnea; R, right; Std Dev, standard deviation.
a P value shows the Mann-Whitney U test.
Correlation test results in the OSA group are shown in Table 3.
Correlation Test Results in the OSA Group.
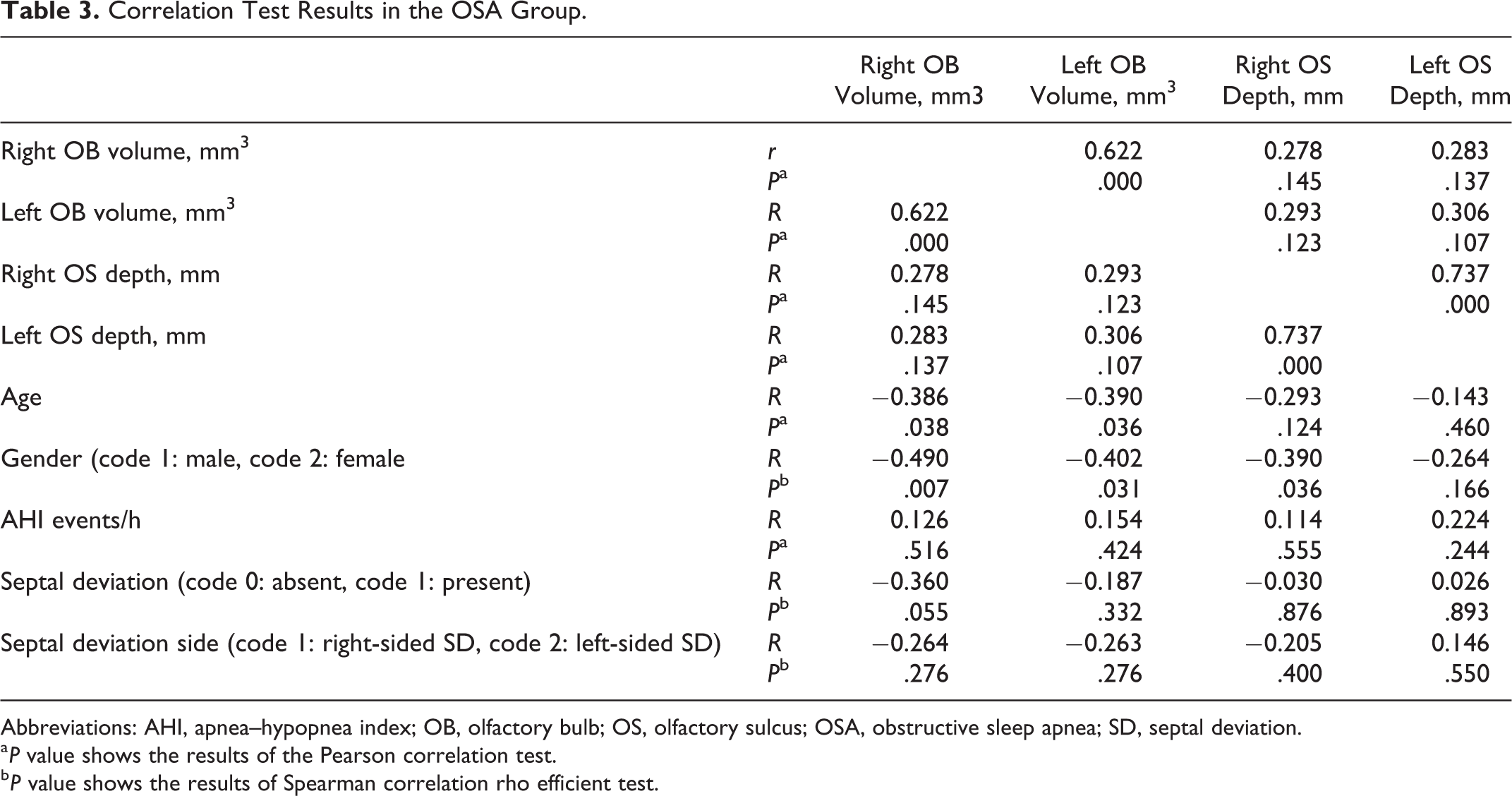
Abbreviations: AHI, apnea–hypopnea index; OB, olfactory bulb; OS, olfactory sulcus; OSA, obstructive sleep apnea; SD, septal deviation.
a P value shows the results of the Pearson correlation test.
b P value shows the results of Spearman correlation rho efficient test.
– There was a positive correlation between the right and left OB volumes and right and left OS depth values (P < .05).
– In older patients with OSA, OB volumes decreased bilaterally (P < .05).
– In female patients with OSA, OB volumes (right and left) and right OS depth values were lower than those of the male patients with OSA (P < .05).
Discussion
Obstructive sleep apnea is associated with apnea and reduction of airflow (hypopnea) during sleep. 12 -14 In patients with OSA, cardiovascular and cerebral mortality and morbidity were increased. 15 -17 In moderately severe OSA (AHI > 15), a higher incidence of stroke was reported. 17,18 Olfactory bulb volume measurement on MRI shows the olfactory functions. 19,20 Therefore, we investigated olfactory functions of patients with OSA by measuring OB volume and OS depth on MRI. Olfactory bulb volumes of the OSA group were significantly lower than those of the control group, whereas OS depth values were not different. There was a positive correlation between the right and left OB volumes and right and left OS depth values. In older patients with OSA and in female patients with OSA, OB volumes decreased bilaterally. Olfactory sulcus depth of the right side was lower in the female patients with OSA compared to the male patients with OSA.
Salihoğlu et al 21 investigated the effects of OSA on the olfactory functions (odor threshold, odor discrimination, and odor identification tests). They also measured the OB volumes. Their results showed that there was a negative correlation between AHI and odor threshold scores and odor discrimination scores. Apnea–hypopnea index also had a negative correlation with odor identification scores and OB volumes (right and left side). In the present study, we cannot find a significant correlation between AHI and OB volumes and OS depth values in the OSA group, whereas in the OSA group, OB volume values were significantly lower than those in the control group.
Cell neurogenesis and hippocampus, frontal cortex, and grey matter density also reduced in patients with OSA. 22,23 Magliulo, et al 24 investigated olfactory dysfunction in patients with OSA. Sniffin’ Sticks method was used to evaluate olfactory performance. In 36.6% of the 60 patients, olfactory dysfunction was detected. There was a positive correlation between AHI and olfactory dysfunction. They concluded that the severity of the disease determined with the AHI results was related to the degree of the olfactory dysfunction.
In patients with OSA, intermittent nocturnal hypoxia/reoxygenation episodes may be a trigger for upper airway inflammation; and proinflammatory markers (ie, interleukin 8, tumor necrosis factor α, or C-reactive protein) increase. 25 -27 The increase of these mediators might be harmful on olfactory neuroepithelium 24 and olfactory impairment may occur.
In patients with OSA, concurrent nasal obstruction was most often occurred. 28,29 Nasal obstruction causes increase of upstream airflow resistance and pharynx became vulnerable to collapse. 24 Nasal obstruction is also associated with olfactory disorders because the number of odourants entering the nasal cavity during the breathing is reduced. 30 -33 In Fu et al’s study, 34 there was a correlation between nasal obstruction and lower threshold, discrimination, and identification (TDI) scores in patients with OSA. They concluded that nasal structure affects olfactory functions due to the probable alterations in nasal airflow.
In the present study, OB volume and OS depth values of patients with OSA were not different between SD present and absent groups. The difference between our study and Fu et al’s study 34 may be related to the degree of the nasal obstruction. Complete nasal obstruction or more anteriorly located nasal SD near to the nasal valve (ie, Mladina type 2 nasal SD) 35 may reduce the transfer of the nasal odorants to the olfactory epithelium; and OB volume decrease may be more prominent in these patients. One of the limitations of our study is that we did not evaluate the classification of the nasal SD as complete obstruction or not; and in the future, we will plan to evaluate the nasal obstruction degree and investigate the OB volume and OS depth in these patients. The main strength of our study is to evaluate OB volume and OS depth in the MRI of the patients with OSA.
Conclusion
In patients with OSA, OB volumes decrease bilaterally. It may be related to intermittent nocturnal hypoxia/reoxygenation episodes, which may be a trigger for upper airway inflammation; and pro-inflammatory mediators maybe harmful on olfactory neuroepithelium and olfactory impairment may occur.
Footnotes
Authors’ Note
Adil Doğan and Hamza Şahin contributed to planning, designing, data collection, and literature survey. Nuray Bayar Muluk contributed to planning, designing, literature survey, statistical analysis, and writing. This study is retrospective. Ethics committee approval was obtained from the Clinical Researches Ethics Committee of Kahramanmaras Sutcu Imam University Faculty of Medicine was also taken (Date: February 6, 2019, Number: 12, Meeting No: 2019/02).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.