
Abstract
Introduction
Obstructive sleep apnea (OSA) is accompanied by arousal that often disrupts sleep continuity and leads to disturbance in sleep architecture.1,2 Clinically, the sleep architecture consists of 2 periods: the non-rapid eye movement (NREM) period and the rapid eye movement (REM) period. The NREM period is subdivided into 3 stages (N1, N2, and N3), and the REM period is characterized by rapid eye movements, muscle atonia, and desynchronized electroencephalography (EEG). Both NREM and REM periods have a dramatic impact on many aspects of physiology and behavior. 3 Previous studies indicated that there is a relationship between OSA and REM. On the one hand, OSA is associated with a reduction in REM. The more severe the OSA, the shorter the REM sleep duration. 4 On the other hand, episodes of apnea or hypopnea during REM sleep are longer and are associated with a more profound drop in oxygen saturation than non-REM sleep, which is also defined as REM-related OSA. 5 Meanwhile, the coexistence of OSA with laryngopharyngeal reflux (LPR) is high, usually up to 55% to 64.3%.2,6 In addition, many studies demonstrated that there is a connection between LPR and REM sleep duration. Zhang et al. 7 studied rats with LPR and found that the LPR symptoms gradually reduced as the REM sleep duration decreased when the rats were in the supine position. However, it is unclear how the change in REM sleep duration in patients with OSA affects LPR symptoms. Therefore, the aim of this study is to explore the association between REM sleep duration and LPR in patients with OSA.
Patients and Methods
Patients
In all, 99 patients, who were admitted to the Department of Otolaryngology between November 2017 to February 2023 and diagnosed as OSA by polysomnography (PSG), were enrolled in this study. Patients’ selection criteria were as follows: (1) meeting OSA diagnostic criteria published by the American Academy of Sleep Medicine (AASM) 8 ; (2) having a history of OSA > 3 months; (3) having no history of taking acid-inhibitory drugs; (4) having no history of esophageal or gastrointestinal surgery; and (5) having no serious cardiovascular diseases or liver-kidney diseases. The study protocol was approved by the Medical Ethics Committee of our hospital with the number Y (2023) 080.
Polysomnography
Alice 5 PSG system (Phillips Respironics, USA) was used for monitoring sleep in all patients. Sleep stages and respiratory events were analyzed by professional technologists based on the criteria of AASM, and OSA was defined as AHI ≥ 5 events/h. Sleep-related parameters included the apnea-hypopnea index (AHI), lowest oxygen saturation (LSO2), and REM sleep duration.
Reflux Symptom Index
All 99 OSA patients filled in the reflux symptom index (RSI) questionnaire under the guidance of the same doctor. The RSI questionnaire included hoarseness or a problem with the voice, throat clearing, excess throat mucus or postnasal drip, difficulty swallowing, coughing after eating or lying down, breathing difficulties or choking episodes, troublesome or annoying cough, sensation of something sticking in the throat or a lump in the throat, and heartburn, chest pain, indigestion, or stomach acid coming up. A score of RSI > 13 was considered positive for LPR, 9 and a higher score indicated more severe LPR.
Study Design
According to the length of REM sleep duration, patients were divided into 2 groups. The patient characteristics and parameters, including sex, age, body mass index (BMI), AHI, LSO2, and RSI scores, were compared between the 2 groups to analyze the effect of REM sleep duration on other parameters. After that, we observed the relationships between RSI scores, AHI, LSO2, BMI, age, sex, and REM sleep duration. If other parameters were correlated with REM sleep duration except for RSI scores, it suggested that the correlation between REM sleep duration and RSI scores might be influenced by other parameters. To exclude the influence of other parameters, we observed the relationship between REM sleep duration and RSI scores while controlling for other parameters. Finally, we observed the factors that may affect LPR in all the parameters that have been collected.
Statistical Analysis
Statistical analysis was carried out using SPSS software version 26.0 (IBM, Chicago, IL, USA). First, a normality test (Shapiro-Wilk test) was performed for all parameters except for sex. The data of normal distribution were expressed by mean ± SD. The data of non-normal distribution were expressed by M (P25, P75). Second, patient characteristics were compared between the 2 groups using the X2 test, Mann-Whitney U-test, or unpaired t-test. Pearson correlation or Spearman’s rank correlation analysis was used to clarify the correlations between RSI scores, AHI, BMI, LSO2, age, sex, and REM sleep duration. Partial correlation analysis was used to analyze the correlations between REM sleep duration and RSI scores separately while controlling for other parameters. Finally, a multiple linear regression analysis was performed with RSI scores as the dependent variable and other parameters as the independent variables to analyze the factors affecting LPR. Statistical significance was set at P < .05.
Results
Among the 99 patients, there were 89 males and 10 females, with a median age of 37 years and ranging from 20 to 67 years. The median BMI was 28.4 kg/m2, ranging from 20.3 to 41.67 kg/m2. The median AHI was 57.30 times per hour, ranging from 5.6 to 112.7 times per hour. The median LSO2 was 77.0%, ranging from 16% to 91%. The median REM sleep duration was 49 min, ranging from 0 to 133 min. The median RSI score was 9, ranging from 0 to 32 (Table 1).
Characteristics of Patients.
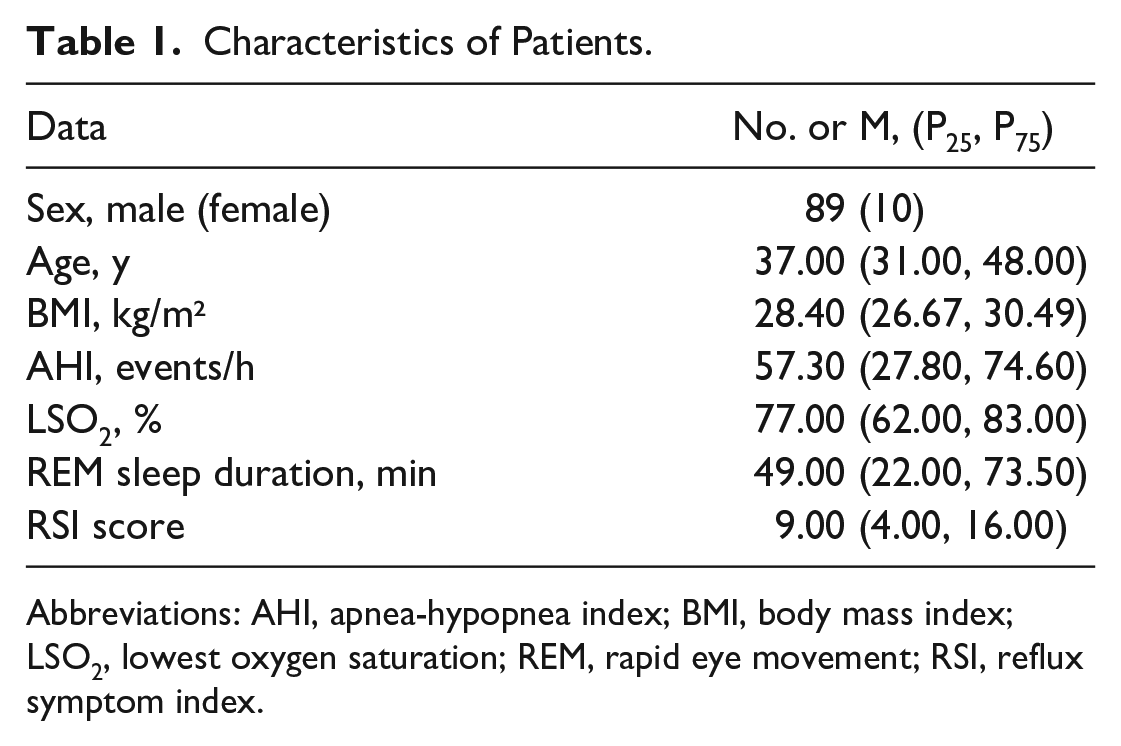
Abbreviations: AHI, apnea-hypopnea index; BMI, body mass index; LSO2, lowest oxygen saturation; REM, rapid eye movement; RSI, reflux symptom index.
According to the median REM sleep duration, 99 patients were divided into the REM sleep duration <49 min group (n = 50) and the REM sleep duration >49 min group (n = 49). The differences in sex, age, BMI, AHI, LSO2, and RSI scores were compared between the 2 groups. The results showed that there were significant differences in AHI (P = .008) and BMI (P = .039) between the 2 groups, and there were no significant differences in sex, age, LSO2, and RSI scores (Table 2). Therefore, the relationship between REM sleep duration and RSI scores might be influenced by AHI and BMI.
Comparison of Patient Characteristics and Parameters Between the REM Sleep Duration <49 min Group and the REM Sleep Duration >49 min Group.
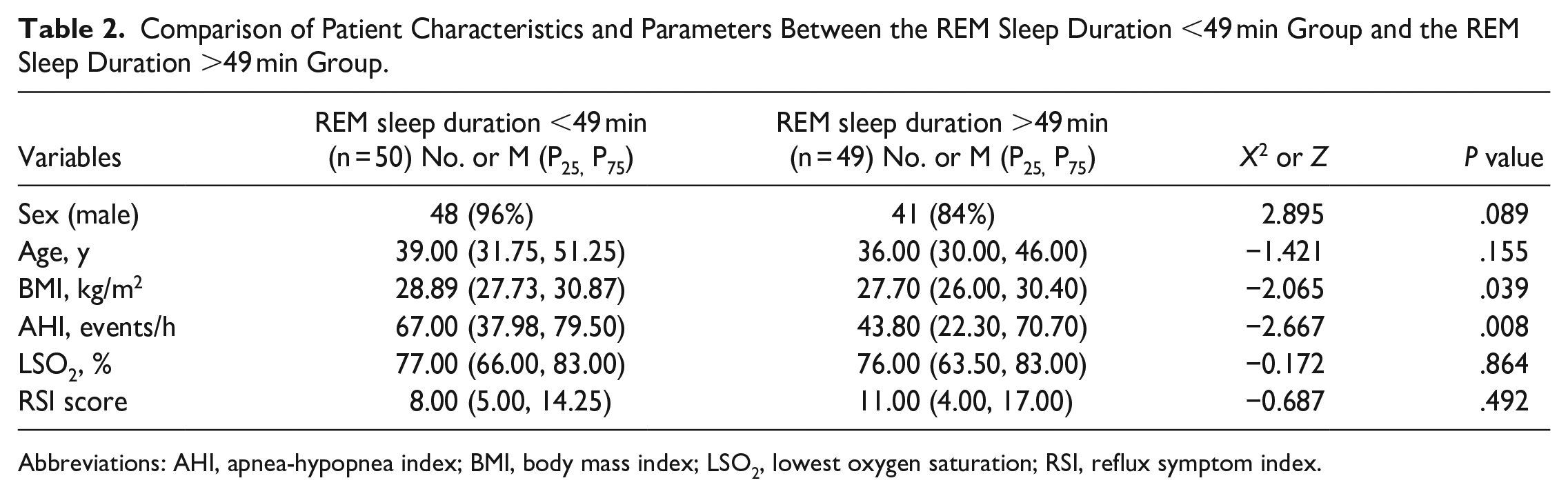
Abbreviations: AHI, apnea-hypopnea index; BMI, body mass index; LSO2, lowest oxygen saturation; RSI, reflux symptom index.
After that, the correlations between RSI scores, AHI, BMI, LSO2, age, sex, and REM sleep duration were analyzed. The results showed that REM sleep duration was negatively correlated with AHI and BMI (r = −0.375, P = .000; r = −0.292, P = .003) but was not correlated with RSI scores, LSO2, age, or sex (Table 3). It demonstrated again that the correlations between REM sleep duration and LPR might be affected by AHI and BMI. Therefore, a partial correlation analysis between REM sleep duration and LPR was performed to explore the true association between REM sleep duration and RSI scores while controlling for AHI, BMI, LSO2, age, and sex. The result showed a positive correlation between REM sleep duration and RSI scores (r = 0.236, P = 0.022) (Table 4). This indicated that the shorter the REM sleep duration, the milder the LPR symptoms. Finally, multiple linear regression analysis showed that only REM sleep duration was independently associated with RSI scores (β = .273, P = .022) among all parameters (Table 5). Therefore, REM sleep duration was a factor influencing LPR.
Correlations Between RSI Score and REM Sleep Duration.
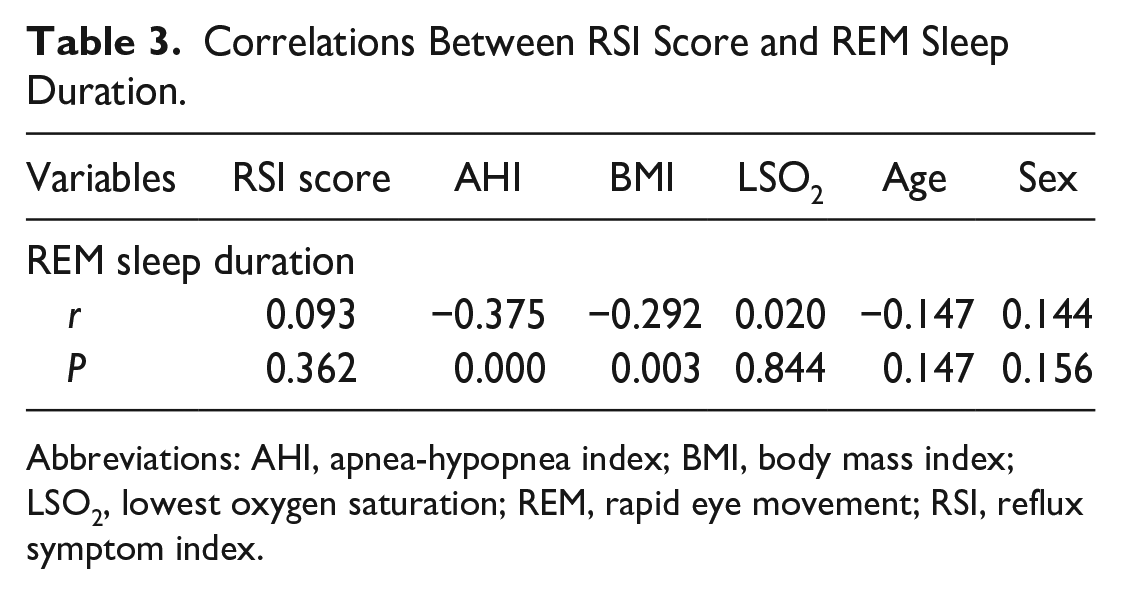
Abbreviations: AHI, apnea-hypopnea index; BMI, body mass index; LSO2, lowest oxygen saturation; REM, rapid eye movement; RSI, reflux symptom index.
Correlations Between RSI Score and REM Sleep Duration While Controlling for AHI, BMI, LSO2, Age, and Sex.
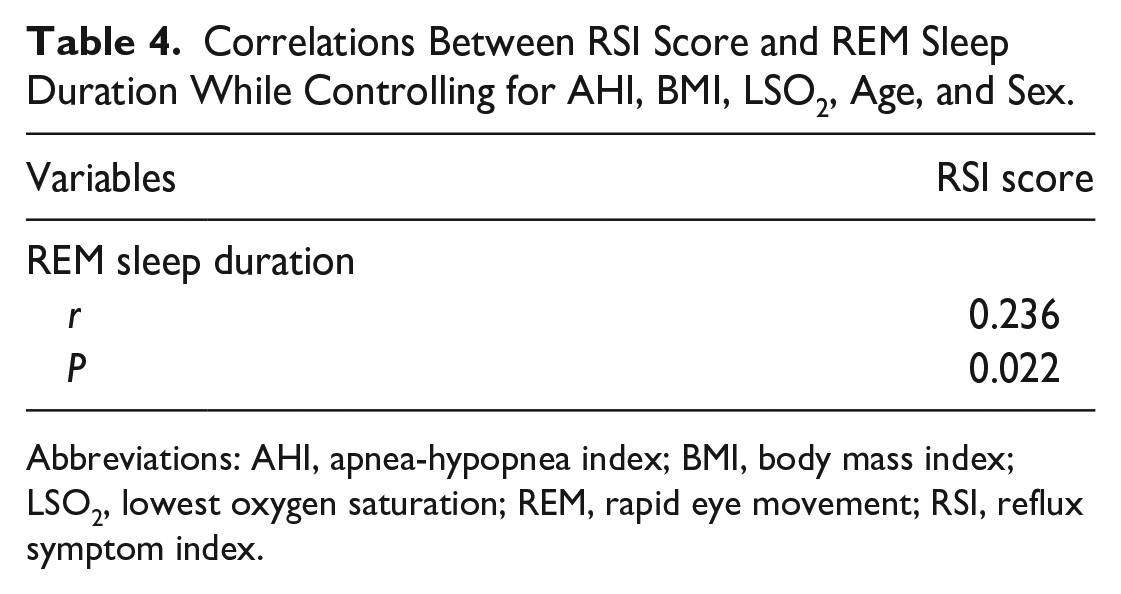
Abbreviations: AHI, apnea-hypopnea index; BMI, body mass index; LSO2, lowest oxygen saturation; REM, rapid eye movement; RSI, reflux symptom index.
Multiple Linear Regression of LPR and Parameters.
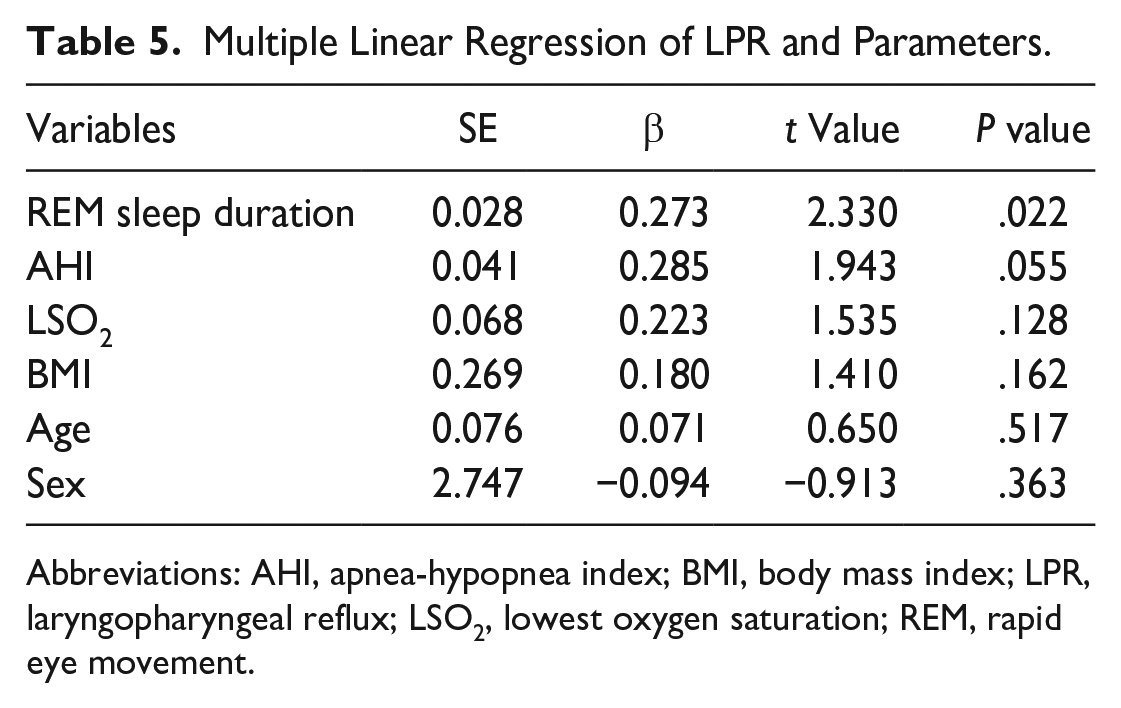
Abbreviations: AHI, apnea-hypopnea index; BMI, body mass index; LPR, laryngopharyngeal reflux; LSO2, lowest oxygen saturation; REM, rapid eye movement.
Discussion
REM sleep is known to have a wide range of neurodevelopmental and cognitive enhancing benefits,10,11 usually occupying 20% to 25% of nighttime sleep in healthy human adults. 12 Furthermore, OSA is now widely recognized as one of the major causes of the reduction in REM sleep. 13 The mechanism may be that there are increased chances of collapse and obstruction of the upper airway in patients with OSA, which, in turn, leads to disruption of REM. Naiman et al. 14 indicated that the severity of OSA is strongly correlated with REM sleep, and it is not unusual to find a total absence of REM sleep in patients with severe OSA. In addition, the treatment of OSA can result in an intense rebound of previously suppressed REM sleep duration. Peregrim et al. 15 indicated that AHI is significantly higher in REM sleep than in NREM sleep in patients with OSA. Therefore, OSA and REM sleep may influence each other and have a close relationship.
Furthermore, many scholars discussed the relationship between OSA and LPR. Previous studies demonstrated that LPR is common in OSA patients, and LPR symptoms are significantly worse in patients with severe OSA.16,17 However, many recent studies demonstrated that there is no relationship between OSA and LPR. Thereinto, Wang et al. 18 demonstrated that there are no significant differences in LPR episodes and pH values between simple snorers and OSA patients, so OSA does not correlate with a higher incidence of LPR episodes. Campanholo et al. 19 found in 701 patients that the presence of LPR is associated with older age, smoking, excessive daytime sleepiness, and worse quality of life and sleep but is not associated with OSA. Tamin et al. 20 found that there are no significant differences in the signs and symptoms of LPR between OSA patients and healthy adults. Therefore, the relationship between OSA and LPR remains controversial. Nevertheless, a high coexistence between OSA and LPR has been confirmed. Studies have shown that OSA and LPR, respectively, affect 2% to 4% and 20% to 40% of adults,21,22 whereby the coexistence of OSA and LPR ranges from 55% to 64.3%.16,23
However, there is little research on the relationship between REM sleep and LPR. Zhang et al. 7 found in a preliminary study in rats that chronic REM sleep deprivation can reduce LPR symptoms in the supine position. The authors speculated that the reduction in LPR symptoms may be due to the dilution of intraesophageal reflux by glandular secretions. The frequent LPR leads to higher secretion from the submucosal glands of the pharynx, and reflux may be diluted by a large number of secretions existing in rats’ pharynx in the supine position. However, there are anatomical and pathophysiological differences between humans and rats. It is unclear whether changes in the REM sleep duration in OSA patients will have similar effects on LPR as in rats.
To assess the effect of REM sleep on LPR in patients with OSA, we divided the OSA patients into 2 groups in our study according to the REM sleep duration. First, we compared the differences in patient characteristics and related parameters between the 2 groups, and the results showed that they were statistically significant in AHI and BMI. This suggested that AHI and BMI were higher in patients with shorter REM sleep duration. However, there was no significant difference in RSI scores between the 2 groups. Second, we analyzed the correlation between REM sleep duration and other parameters, and the results showed that the shorter the REM sleep duration, the higher the AHI and BMI. These results validated that the relationship between REM sleep duration and LPR might be affected by other parameters. To exclude the effects of other parameters, we analyzed the correlation between REM sleep duration and RSI scores while controlling for AHI, BMI, LSO2, age, and sex. The result showed that the REM sleep duration was positively correlated with the RSI scores, which indicated that the longer the REM sleep duration, the more severe the LPR symptoms. Finally, the multivariable analysis showed that only the REM sleep duration was a risk factor for LPR.
Our result was in line with the experimental result that was observed by Zhang et al. 7 in rats in the supine position. This result indicated that the decrease in REM sleep duration could lead to a reduction in LPR symptoms. In addition, several previous studies could also explain our findings. Kahrilas et al. 24 found that REM sleep promotes the development of gastro-esophago-pharyngeal reflux because during REM sleep, the upper esophageal sphincter (UES) is relaxed, and the upper esophageal sphincter pressure (UESP) is significantly lower compared to stage 1 sleep and wakefulness, which, in turn, leads to a tendency for gastric contents to reflux into the esophagus. There was an absence of reflex enhancement of UESP after reflux. Lang et al. 25 demonstrated that both short-term and long-term esophageal acid exposure decreases sensitivity to activation of esophago-upper esophageal sphincter contractile response (EUCR), which led to a delayed contraction of the UES and exacerbated gastric contents reflux. These may be based on the relationship between REM sleep, autonomic dysfunction, and LPR. Previous studies have shown that both the series of pathophysiological responses produced by OSA and the specificity of neuromodulation during REM sleep can have an impact on autonomic nervous system function, leading to autonomic dysfunction.26,27 The autonomic dysfunction can cause abnormal regulation of gastric peristalsis and UES and lower esophageal sphincter functions, making LPR a risk factor for LPR disease. 28 Overall, we speculated that there may be a positive feedback mechanism in OSA patients. When REM sleep duration decreases, the UES contracts and UESP increases. This phenomenon results in gastric contents being less likely to reflux into the esophagus, which, in turn, reduces the LPR symptoms. The reduction of acid exposure increases the sensitivity of EUCR activation so that the symptoms of LPR are further reduced. Conversely, when REM sleep duration gradually increases, the UES relaxes and the UESP reduces. This phenomenon results in gastric contents being more likely to reflux into the esophagus, which, in turn, leads to the development of LPR. The acid exposure due to LPR, in turn, decreases the sensitivity of EUCR activation so that the symptoms of LPR are worse.
Besides, we found a correlation between OSA and REM sleep duration, and the more severe the OSA, the shorter the REM sleep duration. This result demonstrated that patients with long-term OSA had a reduction in REM sleep duration. Simultaneously, the result of our multifactorial analysis showed that AHI was not a beneficial factor to LPR. This finding was in line with many studies in recent years, which indicated that there was no correlation between OSA and LPR. In addition, our study also found an association between REM sleep duration and BMI. The shorter the REM sleep duration, the higher the BMI. This observation may have clinical significance. Previous laboratory studies and epidemiological studies suggested that short sleep duration may be an important risk factor for obesity. Van Cauter et al. 29 indicated that sleep loss may be a novel risk factor for obesity. The increased risk of obesity is possibly linked to the effect of sleep loss on hormones that play a major role in the central control of appetite and energy expenditure. Reduced leptin and increased ghrelin levels correlate with increases in subjective hunger when individuals are sleep restricted which, in turn, leads to obesity. Furthermore, Mavanji et al. 30 found that typical sleep disturbances, such as reduced REM sleep time, were observed in obese individuals. Therefore, we speculated that the reduction in REM sleep may be an important cause of obesity, and improving sleep quality may provide a beneficial aid in reducing obesity.
Overall, the change in REM sleep duration in OSA patients could influence the occurrence of LPR. Therefore, the LPR symptoms were aggravated when the REM sleep duration was longer, which indicated that LPR may mainly appear during REM sleep in OSA patients. Clinically, the effect of REM sleep duration should be considered during the evaluation of LPR. The symptoms of LPR may be improved by adjusting the REM sleep duration appropriately. In the future, we will further investigate the occurrence of LPR during NREM in OSA patients and the relationship between REM sleep duration and LPR in healthy individuals, to explore the characteristics of LPR during different sleep structures (NREM sleep and REM sleep) and their pathophysiological mechanisms.
Our study has certain limitations. First, there was no healthy control group in our study. Second, the RSI is only a subjective scale for the diagnosis of LPR, and we expect to use more standardized LPR monitoring methods to diagnose LPR symptoms in OSA patients in the future.
Conclusion
In conclusion, REM sleep has a wider range of functions. In OSA patients, the LPR symptoms gradually decreased as the REM sleep duration decreased. This indicated that we should pay attention to the physiological and pathological mechanisms of LPR in REM sleep, and more experiments need to be done in the future to elucidate the association between them.
Footnotes
Author Contributions
Dahai Wu, and Zhe Wang: the conception and design of the study, and drafting the article or revising it critically for important intellectual content; Chengcheng Zuo, and Jie Qin: acquisition of data, or analysis and interpretation of data; Shuhua Li: final approval of the version to be submitted.
Data Availability Statements
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Ethics Committee of the Medical Ethics Committee of General Hospital of Northern Theater Command [Y (2023) 080].
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Ethics Committee of the Medical Ethics Committee of General Hospital of Northern Theater Command.
Statement of Informed Consent
Informed consent for patient information to be published in this article was not obtained because of its retrospective study design.