
Abstract
The relationship between objective vestibular tests and subjective vestibular tests is a controversial topic. In this study, to contribute to this issue, the vestibulo-ocular reflex features and their relationship with balance perception at long-term follow-up in vestibular neurectomy (VN) and total labyrentectomy patients were evaluated. Prospectively, 19 VN and 18 labyrinthectomy patients were enrolled in this study. Patients underwent video head impulse test (VHIT) as objective vestibular test and dizziness handicap inventory (DHI) as subjective vestibular test when they attended to their control visit follow-up between March and September 2017. Lateral canal corrective saccades were classified as organized pattern and deorganized (scattered) pattern. In our results, the saccade pattern analysis (between organized and deorganized saccades) regarding the DHI scores gave P value as .039 for covert saccade pattern and .050 for overt saccade pattern. Therefore, we conclude that the presence of saccades, their patterns, and amplitudes provide extra information at assessing the results of the VHIT test, and the organized pattern of saccades is related to a stable vestibular system and better balance perception.
Keywords
Introduction
In cases of refractory Meniere disease (MD), the success rates of vestibular neurectomy (VN) and total labyrinthectomy (TL) procedures are much higher than the other options for vertigo control. Vestibular neurectomy is preferred as a hearing protection option in those with good hearing and its success rate is approximately 90%. Total labyrinthectomy is performed in patients with poor hearing and has reported success rates of approximately 95%. 1 -3 In MD, these procedures provide a stabilized vestibular system by eliminating fluctuating vestibular signals. However, these 2 operations cause unilateral inner ear dysfunctions in patients, therefore having negative effects on the vestibulo-ocular reflex (VOR) and global balance. Patients perceive severe disequilibrium in the early postoperative period due to the immediate decrease in vestibular inputs, but in most patients, long-term vestibular compensation substantially eliminates this signs of dizziness. 4 However, owing to the complexity and multifactorial feature of compensation, 5 dizziness may not be entirely resolved and some patients may have difficulties in daily activities from this residual imbalance perception, which can be assessed with the dizziness handicap inventory (DHI).
Vestibulo-ocular reflex is an important reflex which aims to provide stable vision during rapid head movements. This is accomplished with an eye movement moving at the same speed but in the direction opposite to that of the head. In cases of vestibular hypofunction, this compensatory eye movement is delayed, so to maintain vision fixation on the target, corrective eye movements occur which are called saccades. The saccades that occur during head movement are known as covert and those that occur following the head movement, as overt saccades. 6
The use of the video head impulse test (VHIT) in a clinical setting has increased due to the advantages of the detailed information it provides about VOR. Video head impulse test has been reported to have similar results to those of the scleral search coil test, which is regarded as the gold standard in the evaluation of VOR. 7 The normal range of the VOR gain parameter in healthy populations has been investigated in many studies and has been found to range between 0.83 and 1.21. 8 Video head impulse test allows the recording of eye movements on a high resolution camera and can even detect covert saccades not visible to the naked eye, thereby providing detailed information about saccades and their features. The advantages of the VHIT test include absence of dizziness and nausea during the evaluation, relatively rapid applicability of the test, assessment of the semicircular canals at high frequencies (5-7 Hz) that simulate everyday rapid head movements, and the opportunity to evaluate all canals separately. 7,9
Since some studies have concluded that VOR gain is an incomplete measure of gaze stabilization ability, 6 it has been suggested that careful analyses of saccades could give information about vestibular compensation in unilateral vestibular dysfunctions. 7 Although some researchers have found a weak relationship between objective tests and subjective vestibular tests, 9,10 others have shown that the saccade pattern changes after vestibulopathy from the acute to the chronic period, 11 and these patterns have been found to be related to the perception of dizziness. 12 It has also been shown that vestibular rehabilitation (VR) decreases the abnormality on VHIT and the dizziness perceived by patients. 13 Therefore, the aim of this study was to determine objective indicators for the level of dizziness handicap through the evaluation of saccadic features in the VHIT results of long-term follow-up of patients with vestibular deafferentation. To achieve this, VHIT was applied to patients to objectively detect VOR and the DHI was administered to patients to evaluate dizziness perception.
Materials and Methods
This study was conducted at Gazi University Otolaryngology Department, Ankara, Turkey, and was approved by the university Clinical Research Ethics Committee in March 2017. All the patients provided written informed consent to participate in this study.
Patients with vestibular deafferentation who underwent a follow-up examination between March and September 2017 at least 1 year postoperative since surgery were included in the study. None of the patients underwent supportive VR after the surgery. Video head impulse test and DHI were applied in the follow-up examination. A total of 20 VN and 18 TL patients were enrolled. After exclusion of 1 patient from the VN group because of MD detected in the contralateral ear, a total of 37 patients were included for analysis.
The previous VHIT results of 1 patient from each group (1 VN patient who was excluded due to contralateral MD and 1 TL patient who had previously undergone VN) were reviewed retrospectively from the medical records, and these results are also shown in this study.
Video Head Impulse Test
For the VHIT administered to all patients, the ICS impulse system was used (VHIT, GN Otometrics, Taastrup, Denmark). The test was carried out by a doctoral level audiologist under the supervision of a neuro-otologist. Patients wore a light (ie, ∼60 g) pair of goggles fitted tightly around the head. On the right side of the goggles, there was a small mounted high-speed video camera (250 Hz) and a semisilvered mirror for recording. The eye was illuminated by a diode-emitting low-level infrared light. A small sensor on the goggles also measured the head movement speed. The patient was seated on a chair approximately 100 cm from the wall where the target stickers were located. After the calibration, the test was initiated. The audiologist held the patient’s head parallel to the semicircular canal planes, which rotated both rapidly and unpredictably at 10° to 20°. In a complete test, 20 randomized head movements were accepted from the system for each canal. As there were no patients with underlying spontaneous nystagmus, the ICS impulse feature related to this was not used.
The VHIT outcomes were assessed by a doctoral level audiologist and a neuro-otologist, both experienced in the vestibular field. The following parameters were examined separately for each of the 6 semicircular canals; VOR gain, presence of saccades, amplitude of saccades, and patterns of saccades.
Vestibulo-ocular reflex gain: OTOsuite (version 4.10) vestibular computer software automatically calculates the average of high velocity VOR gain. Each gain was calculated from the ratio of the area under the curve (AUC) for the eye movement to the AUC for the head movement. Head velocity was also determined for each stimulus for each canal.
Presence and amplitude of covert/overt saccades: Saccades are defined as significant acceleration peaks that occur before the end of the head movement (covert saccades) and that occur after the end of the head movement (overt saccades). As there is a wide range of corrective saccades in VHIT, the millisecond of head impulse finalization was determined to differentiate overt and covert saccades. All the accepted saccades during the test were included in the analysis. The software provides all values (ie, amplitude) for each saccade. The averaged values of saccades amplitude were included in the analysis for each patient.
Organized form of covert and overt saccades: If there was an overlap and occurred at close milliseconds, those saccades were classified as “organized”; if not, they were classified as being “scattered,” as defined in the literature. 12
Dizziness Handicap Index Inventory
The Turkish version of the DHI 14,15 was administered to all patients by the neuro-otologist prior to VHIT. This inventory is used to determine changes in the quality of life of patients with dizziness and comprises 25 statements to be answered as yes, sometimes, or no, scored as 4, 2, and 0, respectively. Thus, the total DHI score scale is in the range of 100 (maximum self-reported dizziness handicap) to 0 (minimum dizziness handicap). High scores indicate complaints of dizziness at a level that disrupts everyday life.
Quantitative Variables and Statistical Analysis
Data obtained in the study were analyzed statistically using SPSS version 24 software (SPSS, Chicago, Illinois). Separate analyses were made of the VOR gain, presence of covert and overt saccades, and saccadic amplitude on the operated and nonoperated sides of all the patients in the VN and TL groups. The mean DHI scores for each group and the percentages of the presence of saccades for each canal (anterior, lateral, posterior) were also included in the analyses.
The patients were classified as the organized group or scattered group according to the saccadic features in the VHIT test for the analyses of the relationship between saccadic patterns and DHI scores. The analyses of the saccadic pattern and correlation with DHI scores were made using the lateral canal results.
The Mann-Whitney U test was used for the comparisons of numerical data and the Pearson χ2 test for categorical data. In all the statistical analyses, a value of P < .05 was considered statistically significant.
Results
Evaluation was made of 37 (19 VN, 18 TL) patients, aged 18 to 66 years. The demographic data of both groups are shown in Table 1. The operation groups were similar in respect of mean age (P = .85) and time since the operation to the time that the tests were conducted (P = .45).
Study Patients’ Demographic Results.
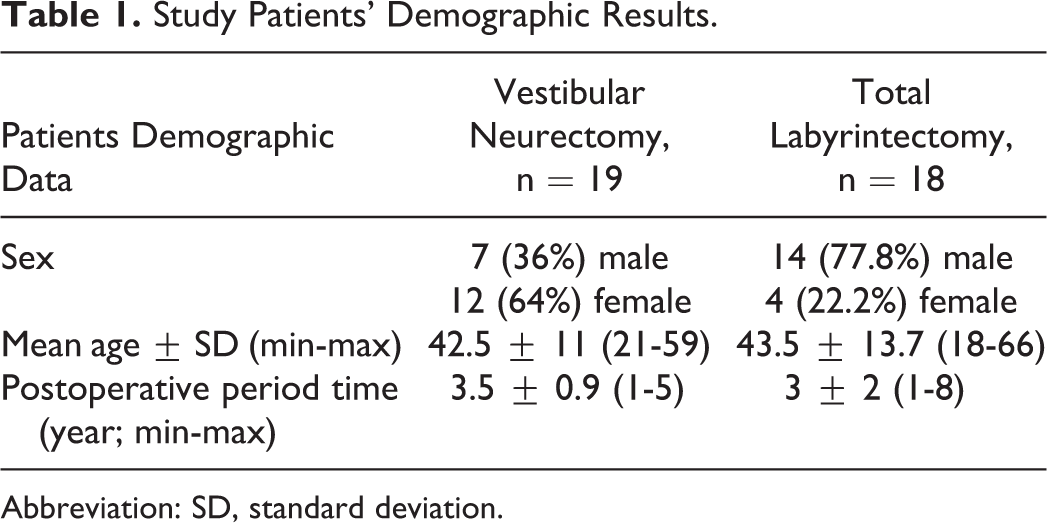
Abbreviation: SD, standard deviation.
The VHIT was performed on all patients. During the test, mean head impulse velocity values in the anterior canal, lateral canal, and posterior canal for all patients were 149 ± 11, 198 ± 4, and 152 ± 10, respectively. The VOR gain results and amplitude data of the saccades are shown in Table 2. In the VN group, a comparative amplitude analysis (between the operated and contralateral sides) of the covert and overt saccades revealed P values of .006 and .001, respectively. In the TL group, a comparative amplitude analysis (between the operated and contralateral sides) of covert and overt saccades revealed P values of .02 and .001, respectively. The side with higher amplitude indicated the vestibulopathy side and was determined to be significant for deciding the hypofunction side with amplitude.
Vestibulo-Ocular Reflex Gain and Amplitude Results of Both Groups and Side in All Canals.
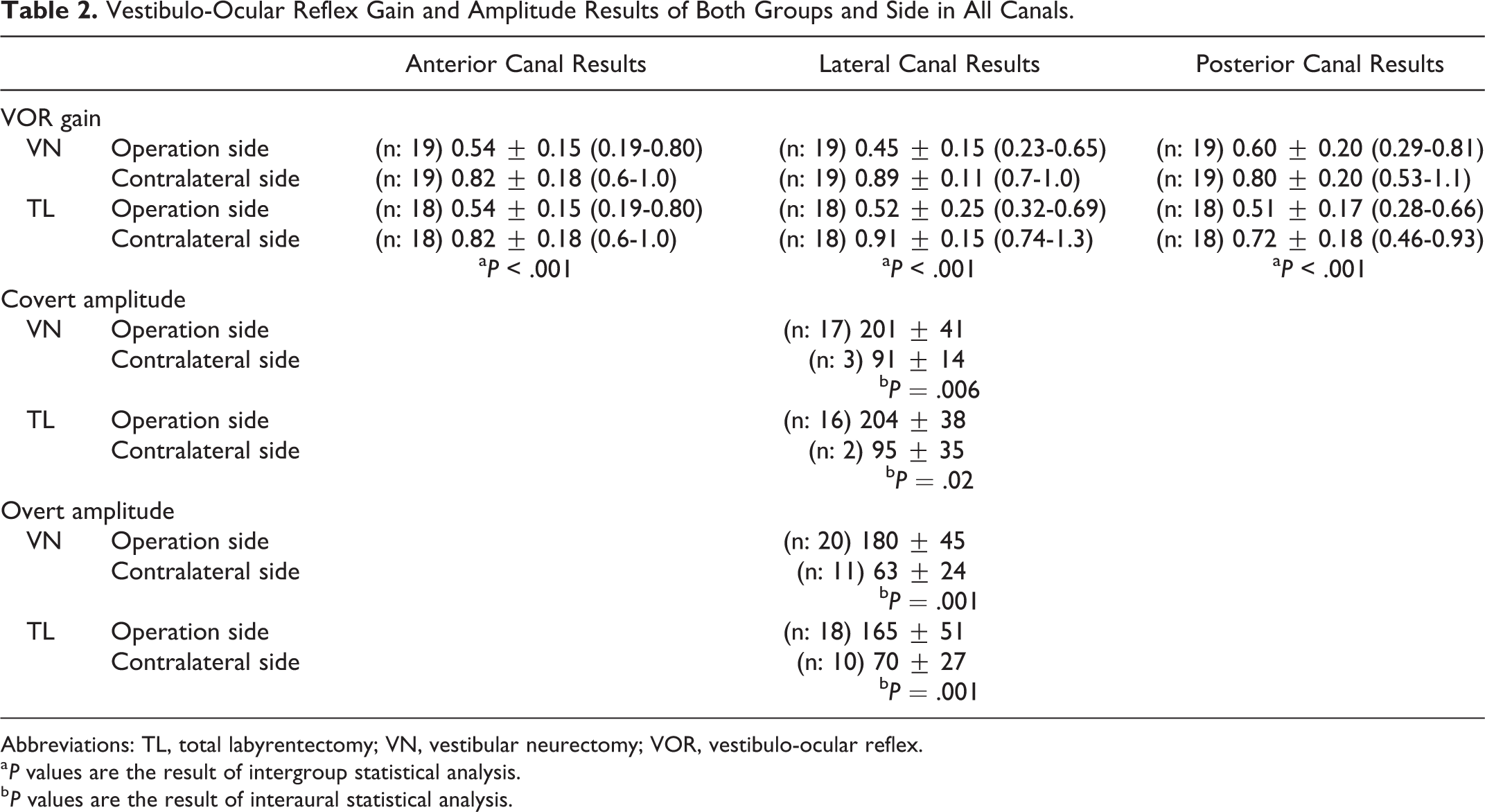
Abbreviations: TL, total labyrentectomy; VN, vestibular neurectomy; VOR, vestibulo-ocular reflex.
a P values are the result of intergroup statistical analysis.
b P values are the result of interaural statistical analysis.
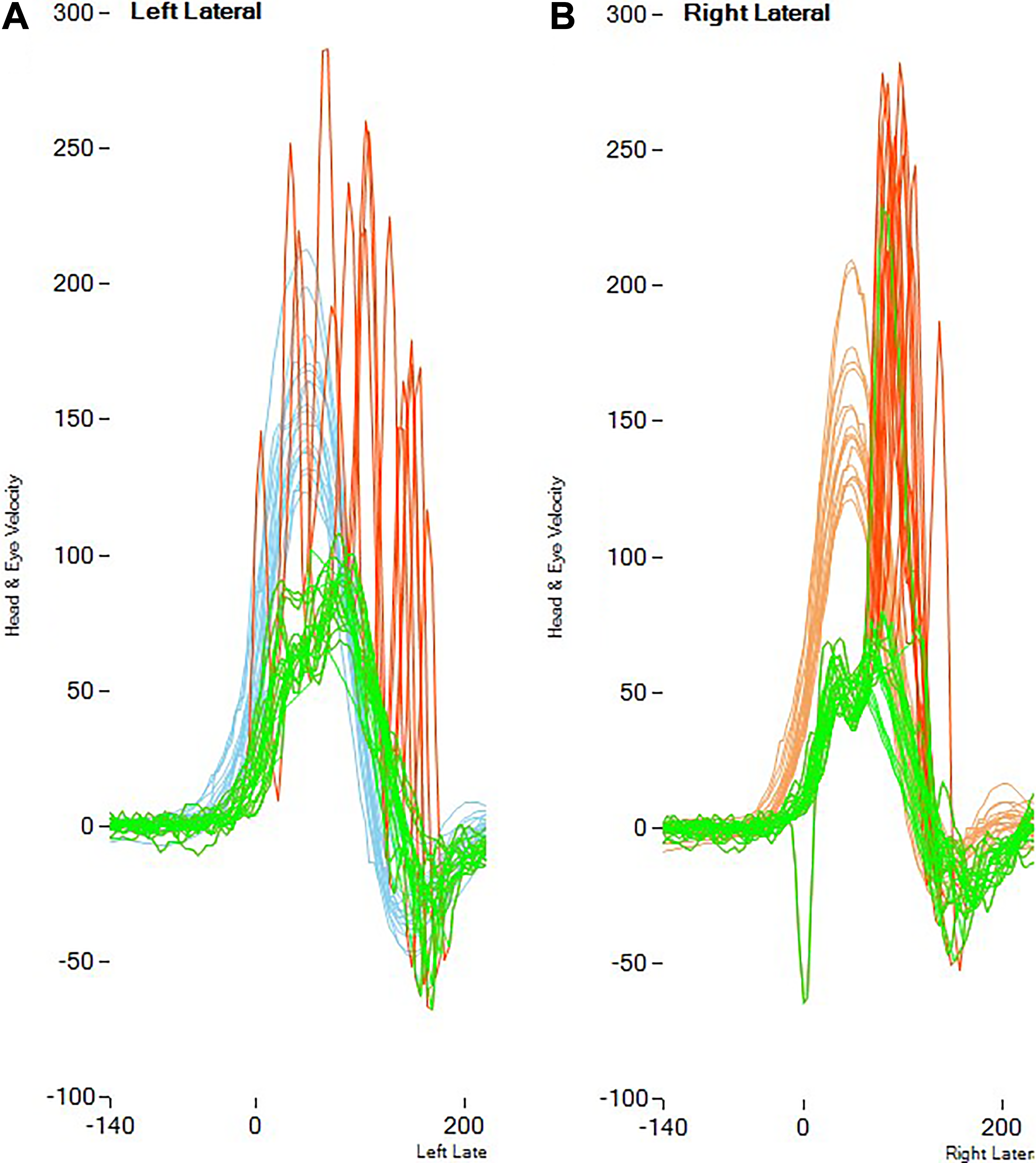
The percentages and P values of the presence and pattern of saccade (Figure 1) for each semicircular canal on the operated and contralateral sides for both groups are presented in Table 3. In respect of covert and over saccade presence, higher values were determined in the lateral canal compared to the anterior and posterior canals (P < .001). Irrespective of the type of surgery, covert saccades in the lateral canal on the operated side were determined in 33 patients and in 29 of these, the covert saccades were in an organized pattern. In the lateral canal, overt saccades on the operated side were determined in 37 patients and in 26 of these, the overt saccades were in an organized pattern. The mean age of the organized and scattered pattern groups of covert saccades were 39.45 years (range: 18-66 years) and 37.75 years (range: 31-44 years), respectively (P = .576). The mean age of the organized and scattered pattern groups of overt saccades were 41.23 years (range: 18-66 years) and 37.91 years (range: 19-52 years), respectively (P = .366).
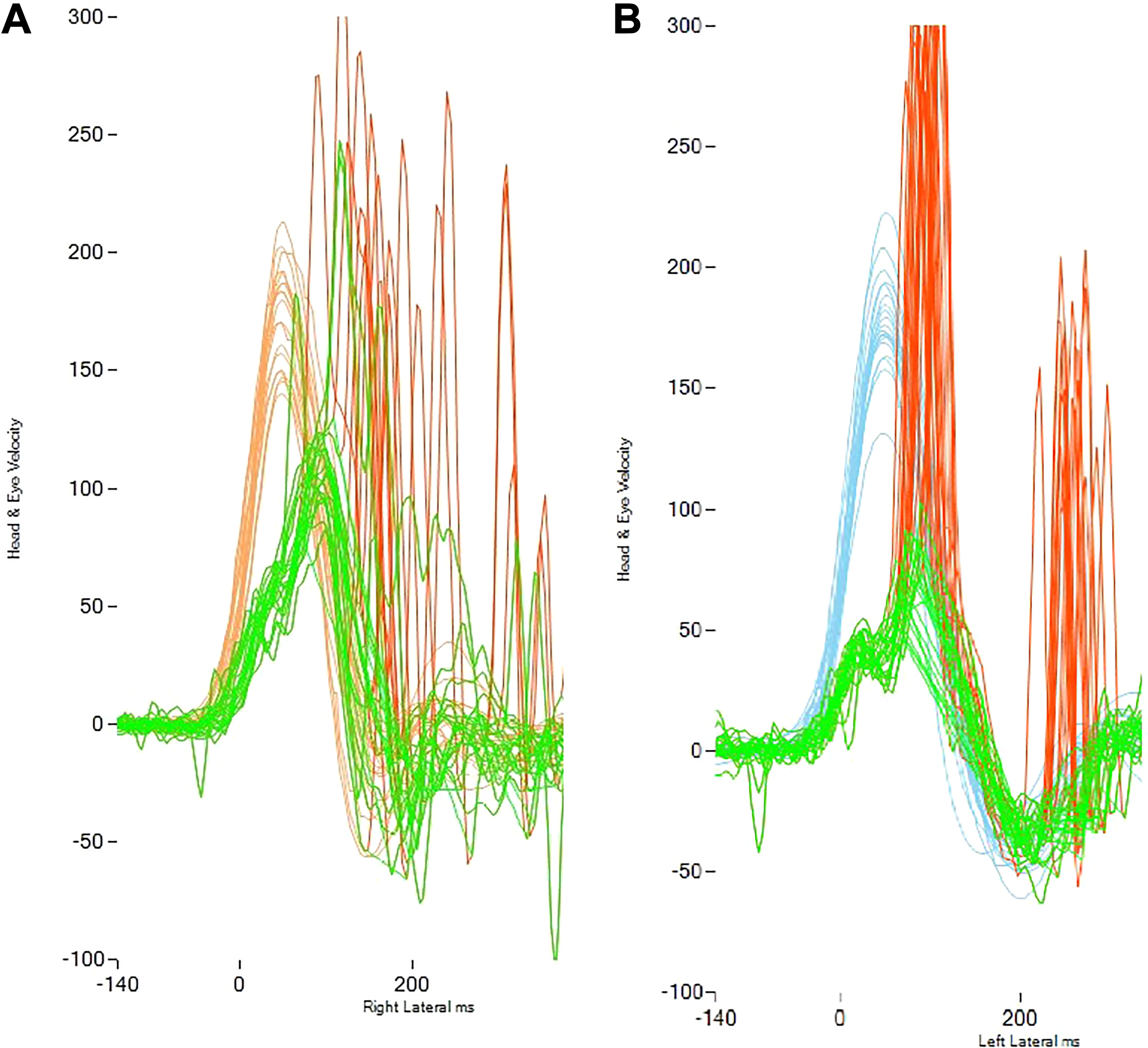
Organization patterns of saccades: (A) scattered saccade pattern; (B) organized covert and overt saccades.
Percentage of Saccade Presence and Organized Pattern for Each Semicircular Canal in Operation Sides and Contralateral at Both Operation Groups.
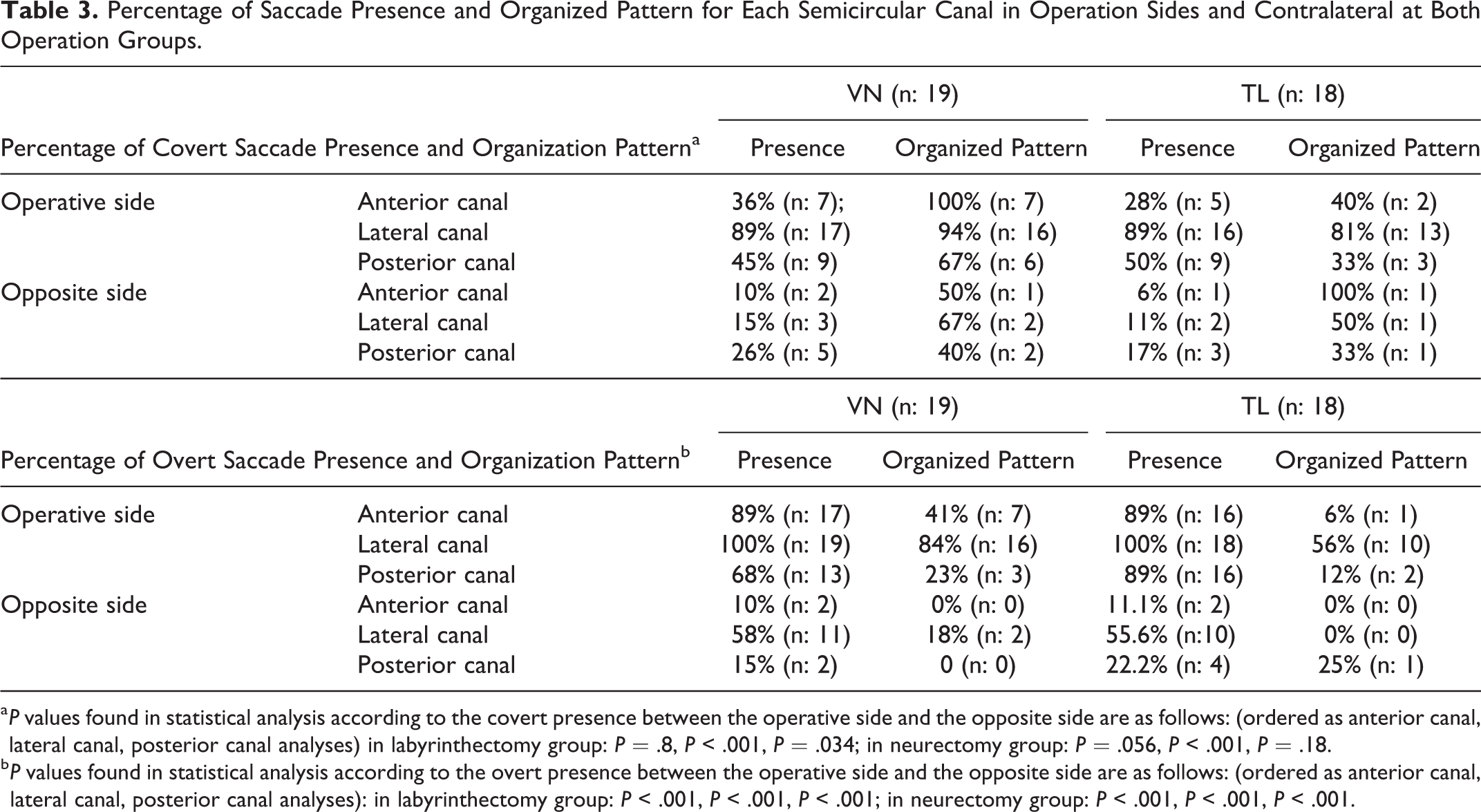
a P values found in statistical analysis according to the covert presence between the operative side and the opposite side are as follows: (ordered as anterior canal, lateral canal, posterior canal analyses) in labyrinthectomy group: P = .8, P < .001, P = .034; in neurectomy group: P = .056, P < .001, P = .18.
b P values found in statistical analysis according to the overt presence between the operative side and the opposite side are as follows: (ordered as anterior canal, lateral canal, posterior canal analyses): in labyrinthectomy group: P < .001, P < .001, P < .001; in neurectomy group: P < .001, P < .001, P < .001.
The DHI was administered to all patients. The median ± interquartile range (minimum–maximum) of DHI score in the VN and TL operation groups were 6 ± 12 (0-28) and 6 ± 18 (0-50), respectively. The values for the DHI scores for both groups are shown in Figure 2. No statistically significant difference was determined between the 2 operation groups in respect of DHI score (P = .892).
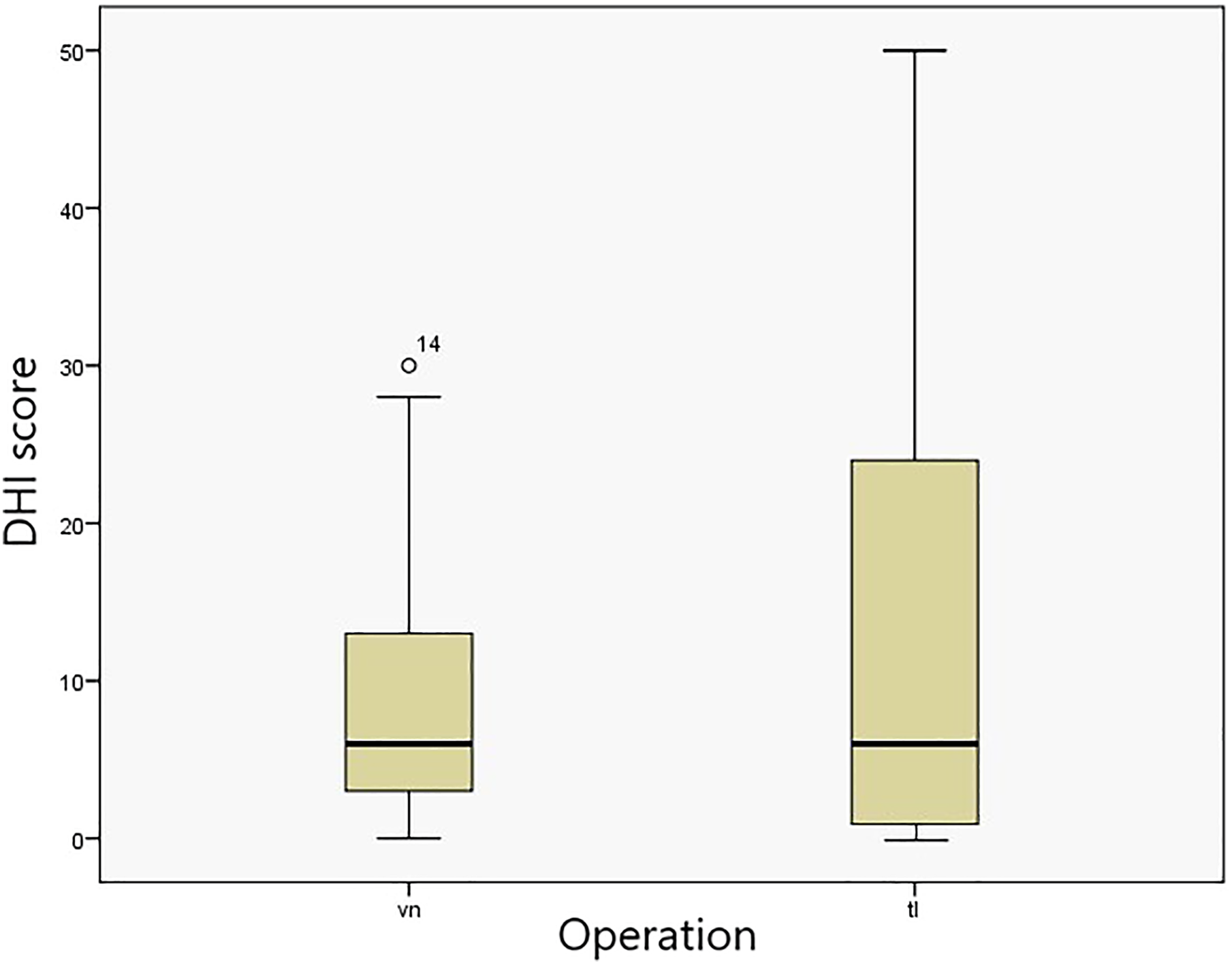
Dizziness handicap inventory (DHI) scores for vestibular neurectomy and total labyrinthectomy groups.
The DHI scores for the organized and scattered saccade pattern groups are shown in Figure 3. The median ± interquartile range (minimum–maximum) DHI scores in the organized pattern and scattered pattern groups were 6 ± 15 (0-26) and 29 ± 37 (2-50) for covert saccade pattern and 6 ± 8 (0-20) and 16 ± 26 (0-50) for overt saccade pattern, respectively. The saccade pattern analysis (between organized and scattered saccades) in respect of the DHI scores revealed a P value of .039 for covert saccade pattern and .050 for overt saccade pattern, which were determined as statistically significant. The scattered pattern for covert saccade was related to a worse DHI score. A scattered pattern of overt saccade was related to a higher DHI score but not at a level of statistical significance. The saccade pattern analysis (between organized and scattered saccades) in respect of age for both saccades did not show statistical significance (Figure 4). Thus, no correlation was determined between pattern and age (covert P = .576; overt, P = .366).
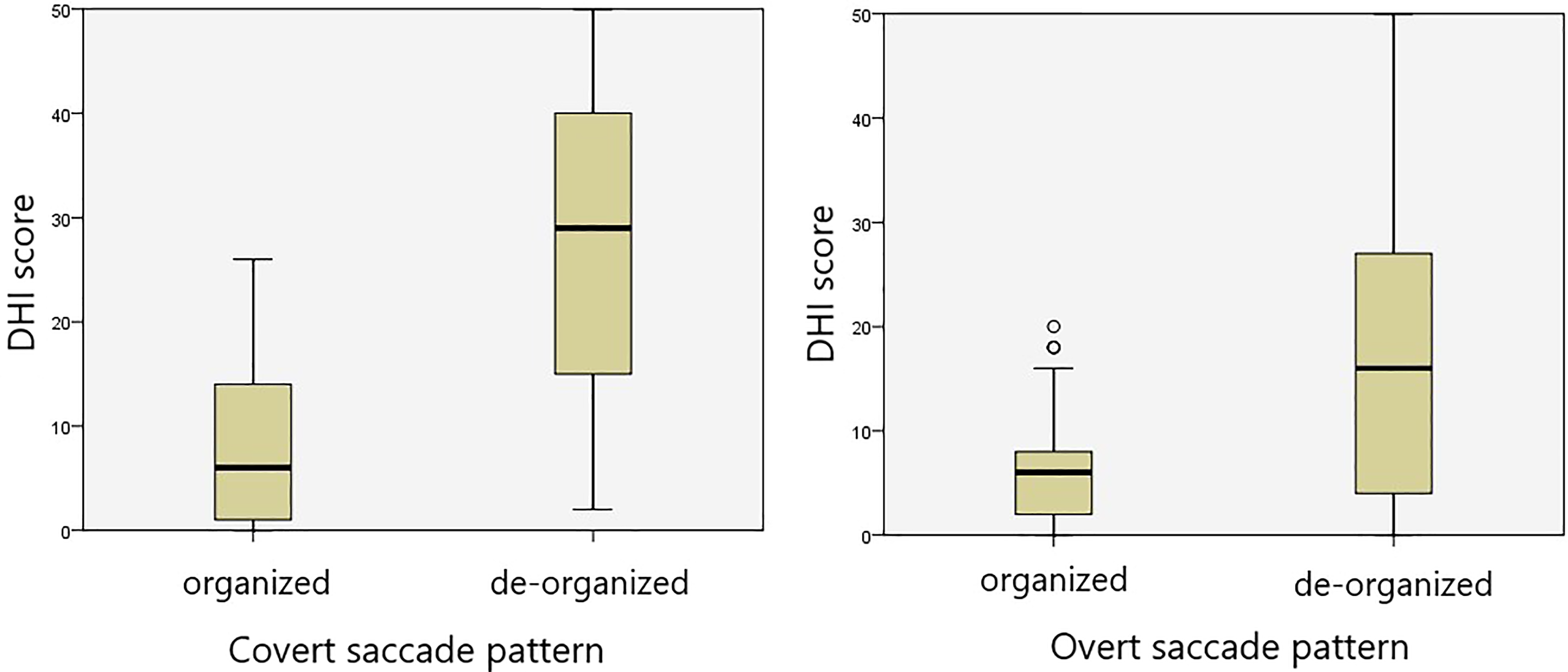
Dizziness handicap inventory (DHI) scores of organized and scattered saccade patterns on the operated side lateral canal results.
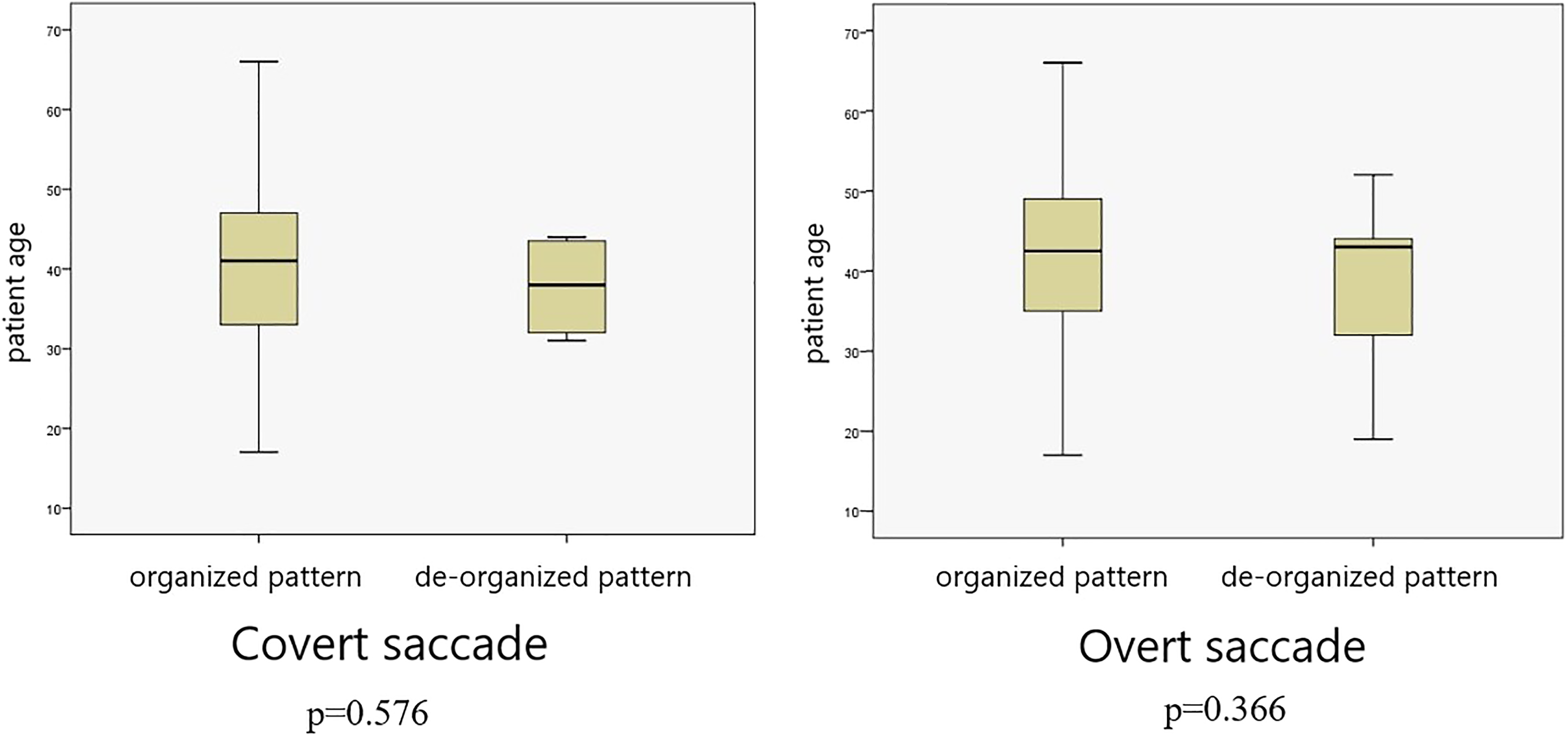
Ages of patients with organized and scattered saccade pattern on the operated side lateral canal results.
In the retrospective examination of the results of the 2 excluded patients, the patient who underwent VN and later TL because of failure of vertigo control (patient revealed positive results from the Dix-Hallpike test and modified Kobrak test on the neurectomy side) has showed a scattered pattern after VN surgery, but after the TL surgery, the first month and first year VHIT results showed that the saccades had become organized over time (Figure 5). In the records of the VN patient who was excluded from the study because of contralateral MD, there was seen to be an organized pattern of saccade on the VN operated side and a scattered saccade pattern in the contralateral ear (Figure 6).
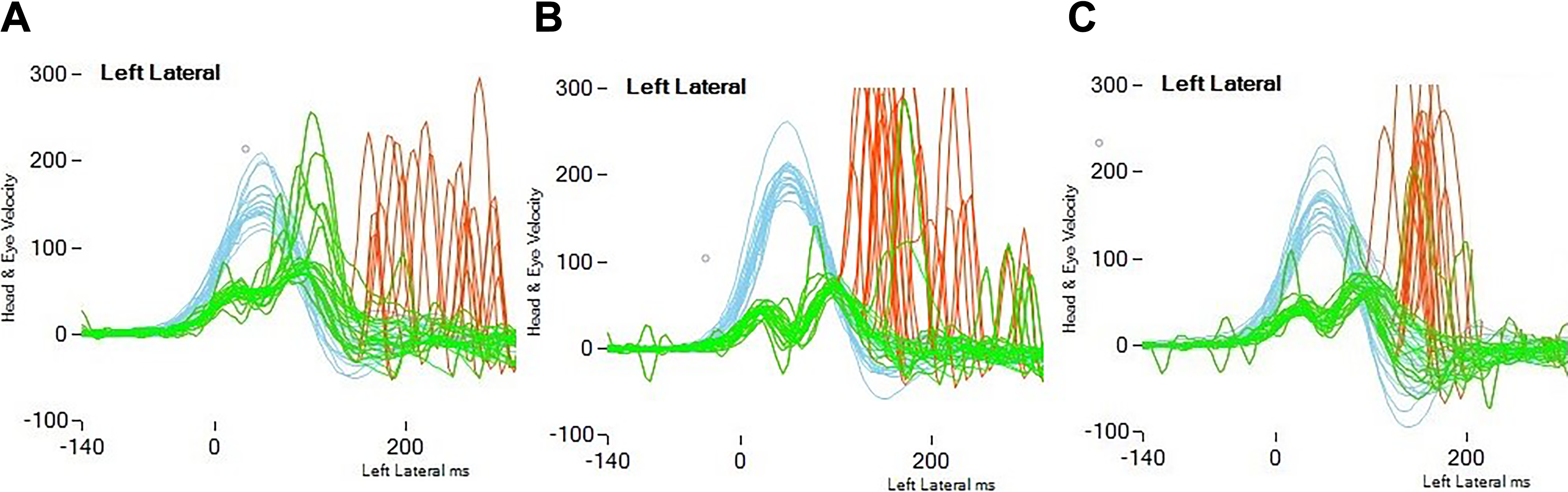
Saccadic pattern transformation in the VHIT tests of the patient who underwent VN procedure first followed by TL due to incomplete vertigo control (A) after VN procedure, (B) 1 month after TL procedure, and (C) 1 year after TL procedure. TL indicates total labyrinthectomy; VHIT, video head impulse test; VN, vestibular neurectomy.
Video head impulse test (VHIT) findings of the patient who underwent VN procedure and developed MD in the contralateral side. A, Scattered pattern on the contralateral side; (B) organized pattern on the operative side. MD indicates Meniere disease; VN, vestibular neurectomy.
Discussion
Patients with MD who do not respond to medical treatment experience very severe dizziness attacks, and ablative surgeries have very high success rates for patients to be able to resume daily life. Vestibular compensation starts in the first days after surgery and ensures the tolerability of the vestibular input deficiency in the patients. 16 However, this varies from patient to patient and some patients may complain about the feeling of imbalance in the long term. Since vestibular compensation is a multifactorial process, this residual imbalance perception can stem from many different reasons. In places where VR facilities are limited, if decompensation of vestibular deafferentated patients with a greater sense of imbalance can be determined with an objective parameter, it may be easier to select suitable candidates for VR. The results of the present study showed that in the long-term follow-up of patients with vestibular deafferentation, a lack of organization in corrective saccade patterns in the VHIT test reflects a higher sensation of imbalance. The results of this study support those of a previous study that investigated long-term compensation after vestibular schwannoma surgery. 12
There is a controversy regarding the long-term effect of differentiation procedures on vestibular compensation. In histological studies, it is assumed that regeneration is preserved in labyrinthectomies with the protection of ganglion cells. 17 From this standpoint, some researchers have suggested that spontaneous neural activity may contribute to central compensation, while others have stated that it may lead to vertigo control failure. 18 In the present study, although the difference in DHI scores between the 2 operation groups was not statistically significant, the interquartile range was broader in the TL group. From Figure 2, it can be seen that some TL patients perceived balance problems more than VN patients. However, in VN, it is more difficult to distinguish the vestibular nerve from the cochlear nerve. Even at the internal acoustic meatus level, some studies have shown that some vestibular nerve fibers progress through the cochlear nerve sheath. 19 This may explain why vestibular neurectomies are less effective than labyrinthectomies in respect of ensuring vertigo control. In a study by Leveque et al 20 on whether complete differentiation was achieved or not after VN, failure was determined in only 1 of 24 patients who had both anterior and posterior canal responses. In parallel with these findings, only 1 of the current study of VN patients required TL to overcome dizziness.
In spite of its low sensitivity, VHIT provides additional information and complements other vestibular tests. 9 It has been reported that saccade presence is associated with a 40% reduction in VOR gain and that saccade characterization in patients with vestibular pathologies with normal VOR gain could potentially provide additional information. 21 Considering this phenomenon, it was found in the current study that more data can be obtained by reading the corrective saccades and their features in VHIT. In some previous studies, a weak relationship has been seen between objective tests and subjective vestibular tests, which could be due to methodological differences. 9,10 In those studies, rotation chair, electronystagmography, and caloric test were used or even if VHIT was used, corrective saccade patterns were not evaluated. In contrast, in another study, significant findings were found between saccade patterns and DHI scores, 12 which was compatible with the current study results. Video head impulse test was used in the present study as it was hypothesized that VHIT results could better reflect the patient’s perception of dizziness because VHIT measures the frequency range (1-6 Hz) equal to the movements in daily life. Therefore, VHIT might be the correct tool in the vestibular battery for the follow-up of patients with vestibular deafferentation.
All patients included in the current study, as expected and reported in the literature, showed significant decreases in VOR reflex gain on the operated side. Corrective saccades were observed during and after the head movement to eliminate this deficiency. These saccades were more obviously detected in the lateral canal as seen in Table 2. Vestibulopathy can be considered to have been better revealed because of the higher acceleration of the head impulses in the lateral canal. 22 Therefore, it can be suggested that saccadic evaluations should be read from the results of the lateral canal. In the current study, presence of both covert and overt saccades showed significance in the statistical analyses between the operated side and the contralateral side. Additionally, the percentages of organized pattern were high in both operation groups as shown in Table 2. The same findings were also observed in the saccadic pattern transformation in the VHIT tests (Figure 5) of the patient who underwent VN first, followed by TL due to incomplete vertigo control. The saccades, which were more scattered after VN, started to get closer in the post-TL first month and were seen to be organized in the postoperative first year. This was thought to be associated with vestibular compensation resulting from a stable vestibular system. In addition, in another VN patient who was excluded from the study because of contralateral MD development, the VHIT findings revealed an organized pattern on the operated side and a scattered pattern on the contralateral side (Figure 6). In this context, if the patterns of saccades are taken into consideration in patients with complaints of dizziness, the findings could be related to a stable vestibular system and the feeling of imbalance. It has been shown that saccades formed when there is no VOR gain changed over time and overt saccades shifted to become covert saccades after the acute phase follow-up. 13,16,23 Therefore, it has been stated that covert saccade could be associated with compensation. 11,22,24 Perhaps, as in the current study of patients, with the presence or transformation to covert saccade, the pattern of approximation to each other might reflect vestibular compensation. Although this was not determined to be statistically significant, it has been objectively reflected in a previous study which showed that the “PR” index (representing the scattering pattern) reduced in patients with acute unilateral vestibulopathy after VR. 13 In the long-term results of the current study of patients with vestibular deafferentation, the percentages of the organized pattern were found to be very high.
The reason for the approximation of saccades has not been clearly identified. In a study which demonstrated the relationship between the difference in patterns and the imbalance felt, the cause of deorganization was correlated with older age and less preoperative vestibular deficit. 12 In addition, there are studies that have revealed an increase in the feeling of imbalance and presence of saccade at an older age. 6 However, in the current study, there was no finding to support this conclusion and no difference was observed between the ages of the organized and scattered groups (P > .05). Despite a lack of objective data, this can be considered to be related to the mobility or sedentary lifestyle of the patient, and the decrease in the number of overt saccades in patients undergoing VR supports this idea. 13 Based on this, a patient with scattered saccades and complaints of dizziness may be a true candidate for VR. Therefore, VHIT can be recommended as a valuable tool for postoperative follow-up of vestibular differentiation patients to be able to select suitable VR candidates.
It has been reported that vestibular hypofunction can be detected when saccade amplitude and the corrective saccade frequency are compared. 22,25,26 The amplitude of saccades has also been found to increase with ageing, 6 while VR has been shown to decrease the amplitude of saccades. 13 As a secondary outcome of this study, findings were obtained that support this consideration; namely, in the statistical analysis between the operated and contralateral sides, saccade presence, and amplitudes, there was determined to be strong significance (P < .05) for the lateral canals in both covert and overt saccade amplitudes. Therefore, in addition to VOR gain, the presence of saccades and interaural comparison of saccade amplitudes can be used to detect the vestibulopathy side.
There were some limitations to this study. First, it was not possible to present the organized or scattered saccade patterns objectively, but this should be possible in the future with new systems and software. Second, as our institution has no regular VR service, the activity and compensation levels of the patients after vestibular differentiation were not homogenous, but this provided the opportunity to compare imbalance perception and its relation with VHIT results. Finally, despite the high number of VN and TL operations performed, some patients did not attend follow-up appointments, so the patient number in the study was relatively low. Despite these limitations, the study was an opportunity to research and discuss VHIT changes in long-term vestibular deafferentated patients and the results can guide more effective use of limited VR facilities.
In conclusion, when evaluating VHIT results, besides VOR gains, the presence of covert and overt saccades and their patterns must also be considered. This assessment will be more meaningful when made on lateral canal results. The scattered pattern of saccades in VHIT is together with higher DHI scores in patients with vestibular deafferentation.
Footnotes
Authors’ Note
This study was presented at the 39th Turkish Congress of Otolaryngology-Head and Neck as an oral presentation, Antalya/Turkey, October 8-12, 2017. This material has never been published and is not currently under evaluation in any other peer-reviewed publication.
Acknowledgments
The corresponding author thanks John P. Carrey for his contribution to the design of the study through the advice given in respect of researching saccadic features, during observership at Johns Hopkins University ENT Department. The authors also thank K. Murat Özcan for valuable contributions to the critical editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.