
Abstract
Objectives:
The aim of this study is to investigate the scutum–cochleariform process (CP) and scutum–promontorium distances according to the mastoid pneumatization condition.
Methods:
Two hundred temporal multidetector computed tomography scans (90 males and 110 females) were evaluated retrospectively. The scutum-CP and scutum–promontorium distances were measured. Facial canal dehiscence (FCD) in the tympanic segment and mastoid pneumatization were also evaluated.
Results:
The distances between scutum-CP and scutum–promontorium were not different between males and females and between right and left sides. Facial canal dehiscence in the tympanic segment was detected: 5.6% (right) and 7.8% (left) in males and 5.5% (right) and 10.0% (left) in females. Grade 4 (100%) pneumatization was detected mainly in 55.6% to 57.8% of the patients in both genders. Grade 0 (0%) pneumatization (sclerosis) was detected in 22.2% to 28.2% of both males and females. In more pneumatized mastoids, the scutum-CP and scutum–promontorium distances increased. In sclerotic mastoids, the scutum-CP and scutum–promontorium distances decreased. Facial canal dehiscence rates were not related to the mastoid pneumatization levels.
Conclusion:
Cochleariform process is an important landmark to localize the tympanic segment of the facial canal. In sclerosed mastoids, scutum-CP and scutum–promontorium distances decreased. There was no relationship between FCD rates and mastoid pneumatization levels. It may be due to the development of FCD that occurs during the intrauterine period. In endoscopic and classic ear surgeries, mastoid pneumatization must be evaluated preoperatively to avoid facial nerve injuries.
Keywords
Introduction
Incidence of iatrogenic facial nerve injury has been reported as 0.6% to 3.6% for primary surgery and 4% to 10% for revision surgery. 1 For perioperative detection of facial canal dehiscence (FCD), specificity and sensitivity of the imaging systems are not high. 2 Therefore, surgeons must evaluate FCD preoperatively and also must know the anatomy of the facial canal very well.
The tympanic segment of the facial canal passes from behind of cochleariform process (CP) and through oval window and advances toward posteroinferior direction. 3 The ratio of FCD varies between 8% and 57% in the literature. Often, in the tympanic segment, it is detected. 4,5 The CP houses the tendon of the tensor tympani. The tendon crosses the middle ear at a 90° angle to the muscle, where it attaches to the neck of the malleus. The CP acts as a fulcrum for this pulley-like action. 6
Scutum is known as the lateral epitympanic wall, and the defect of scutum is considered an indicator of chronic otitis, with cholesteatoma in most of the cases. 7
The aim of this study is to investigate the scutum-CP and scutum–promontorium distances according to the mastoid pneumatization condition. The study was based on temporal multidetector computed tomography (MDCT) images in the database of the Kırıkkale University Faculty of Medicine Radiology Department.
Material and Methods
This retrospective study was conducted in Kırıkkale University Faculty of Medicine according to the principles of the Declaration of Helsinki. Temporal MDCT images were obtained from the database of the Kırıkkale University Faculty of Medicine Radiology Department. Ethics committee approval was obtained from Adana City Training and Research Hospital, Clinical Researches Ethics Committee (date: December 19, 2018, number: 357).
Patients
Two hundred temporal MDCT scans were reviewed. Mean age of the patients was 43.8 ± 15.2 years (ranged from 15.0 to 84.0 years); 45.0% (n = 90) of cases were male and the remaining 55.0% (n = 110) were female.
Inclusion criteria are as follows: Patients who underwent temporal MDCT due to vertigo or otologic complaints. Patients who have had temporal MDCT due to any of the otologic complaints (tinnitus, etc) and whose result is evaluated as normal.
Exclusion criteria are as follows: Patients with previous trauma or surgery history. Those having movement or metal (surgical, prosthesis) artifacts, causing low diagnostic quality. Those with CT results that reported as having temporal mass unilaterally/bilaterally.
This study is retrospective. Ethics committee approval was obtained. There is no need to take informed consent because the data were evaluated retrospectively.
Multidetector Computed Tomography
All scans were obtained from routine temporal bone images in supine position, and no contrast and sedation was used for the procedure. The images were acquired with a 64-slice CT (MSCT; Philips Medical System, Brilliance 64, Best, the Netherlands). All scans were obtained using the following parameters: tube voltage: 120 kV; effective mAs: 350; slice thickness 0.67 mm; the scan field of view of 180 mm, and image matrix of 768 × 768. All images were transferred to a commercially available workstation. First, images were taken at the axial plane and then coronal and sagittal reconstructions of raw data were performed. Later investigations were carried out on this 3-dimensional image. 8
Measurements
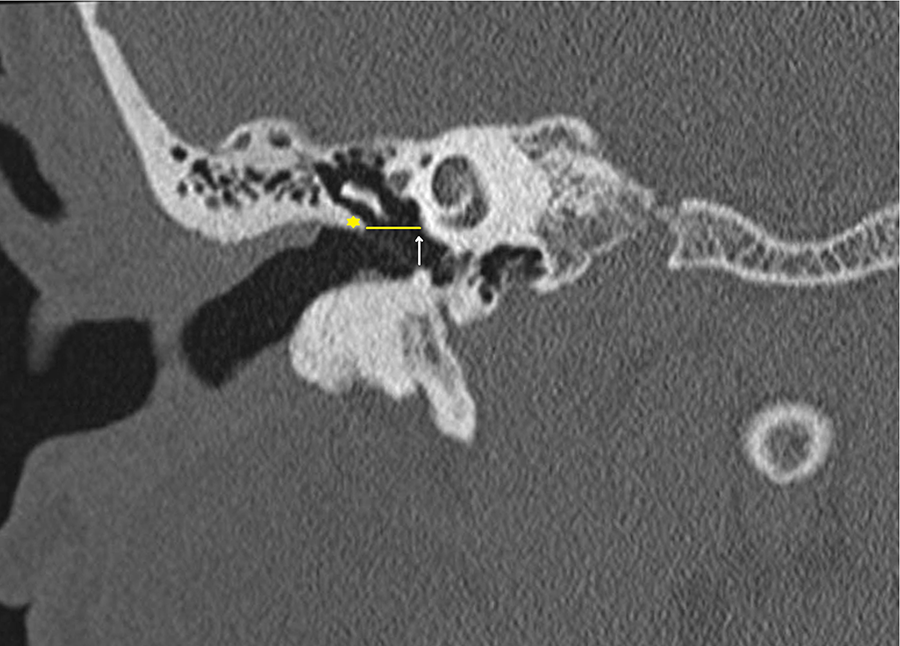
In the coronal temporal MDCT views, the scutum-CP distance was measured (in millimeters; Figure 1). In the coronal temporal MDCT views, the scutum–promontorium distance was measured (in millimeters; Figure 2). In the axial temporal MDCT views, FCD in the tympanic segment was evaluated as present or absent (Figure 3). The mastoid pneumatization was also evaluated as follows (Figure 4):

On coronal temporal multidetector computed tomography, the scutum-CP distance was shown (scutum: yellow star, CP: white arrow, scutum-CP distance: yellow line). CP indicates cochleariform process.
On coronal temporal multidetector computed tomography, scutum–promontorium distance was shown (scutum: yellow star, promontorium: white arrow, scutum-promontorium distance: yellow line).
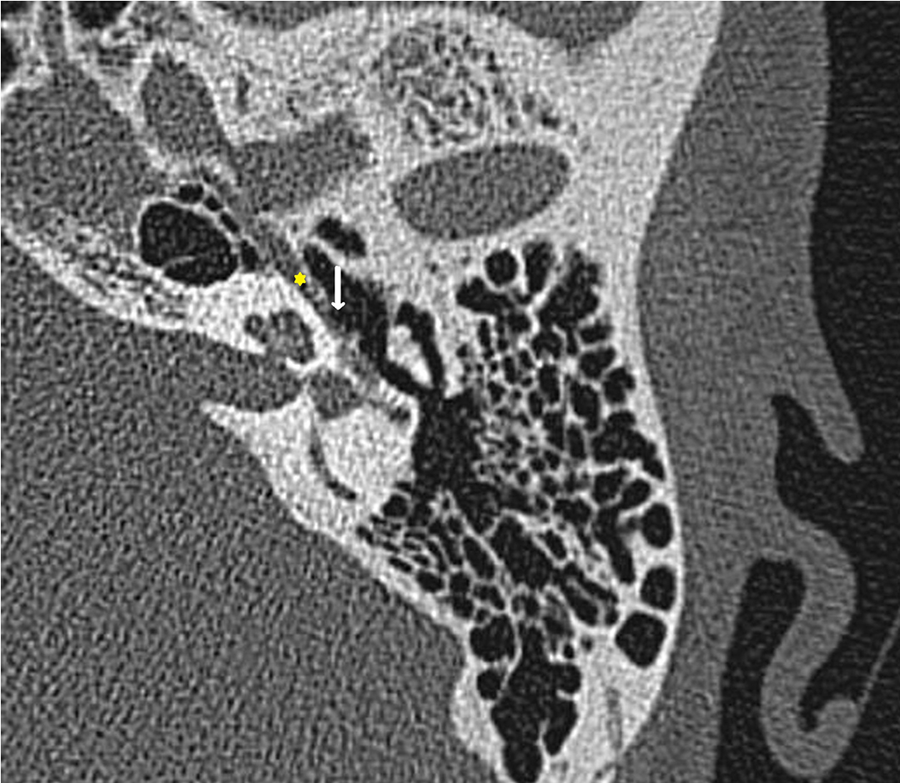
On axial temporal multidetector computed tomography, dehiscence (white arrow) in the facial canal tympanic segment (yellow star) was shown.
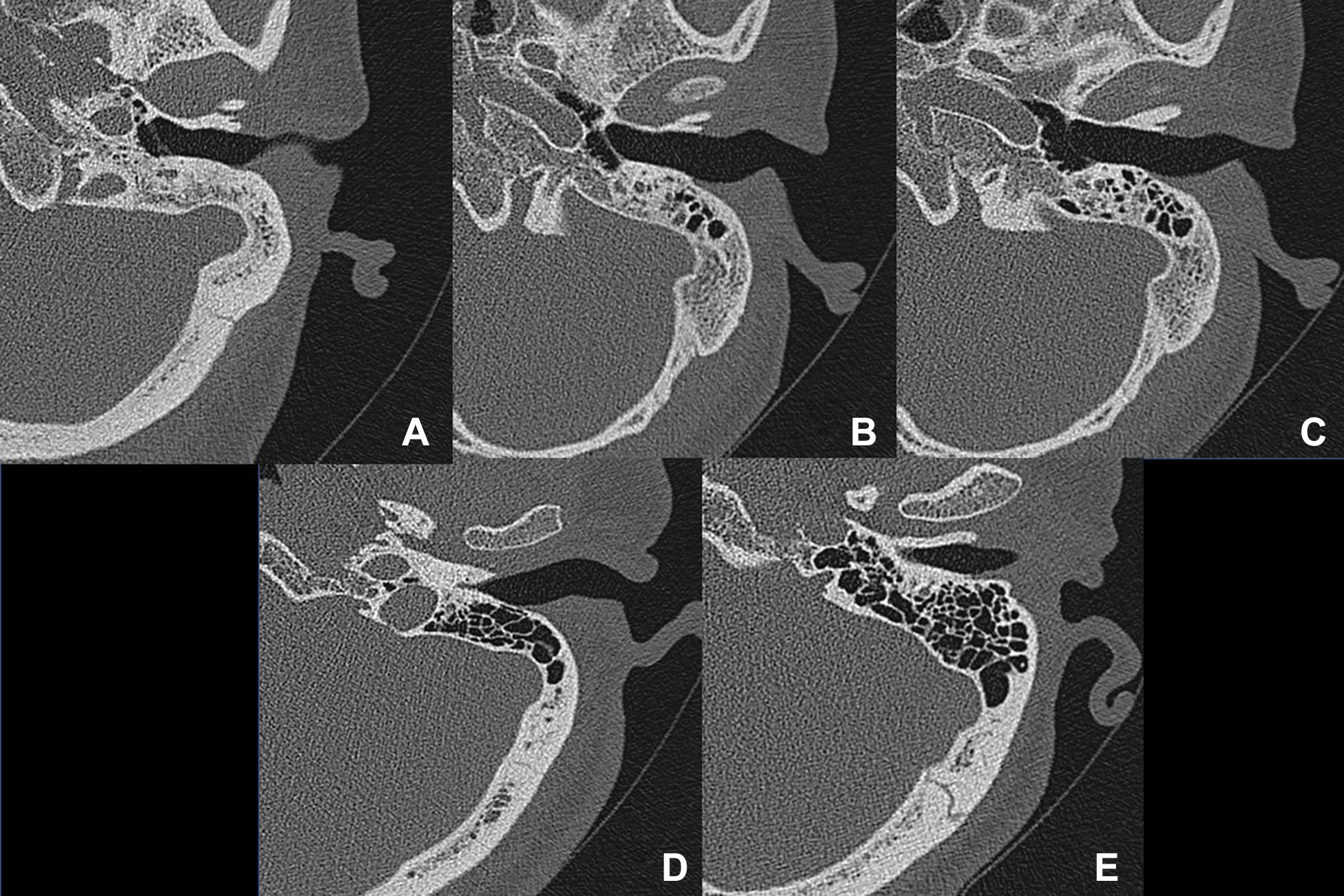
Mastoid pneumatization was shown on axial temporal multidetector computed tomography. (A) Grade 0: No mastoid pneumatization, (B) grade 1: 25% aeration, (C) grade 2: 50% aeration, (D) grade 3: 75% aeration, and (E) grade 4: 100% aeration.
Statistical Analysis
All analyses were performed using version 16 of the Statistical Package for the Social Sciences software. Independent samples t test, paired samples t test, χ2 test, and Spearman correlation ρ coefficient test were used. A P value <.05 was considered to reflect statistical significance.
Results
Measurement results of scutum-CP and scutum–promontorium, FCD, and mastoid pneumatization are indicated in Table 1. The mean of the scutum-CP distance was 5.84 ± 0.77 mm (right) and 5.81 ± 0.82 mm (left) in the males and 5.73 ± 0.66 mm (right) and 5.70 ± 0.65 mm (left) in the females (P > .05). Scutum–promontorium distance was 5.56 ± 0.68 mm (right) and 5.56 ± 0.64 mm (left) in the males and 5.55 ± 0.65 mm (right) and 5.56 ± 0.64 mm (left) in the females (P > .05). For each of the males and females, the differences between right and left sides for scutum-CP and scutum–promontorium were not significant (P > .05; Table 1).
Measurement Results of Scutum-CP and Scutum–Promontorium, Facial Canal Dehiscence, and Mastoid Pneumatization.
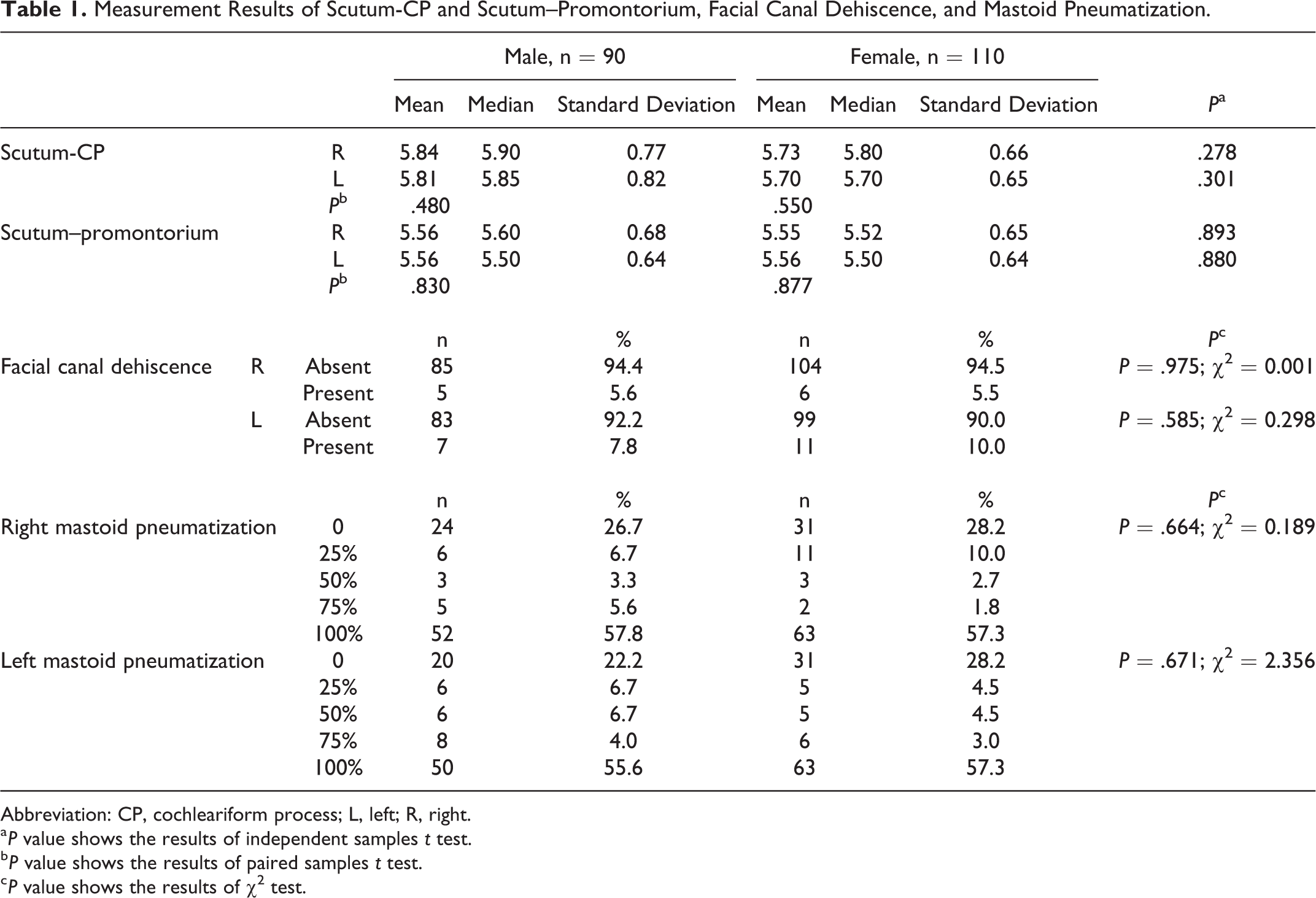
Abbreviation: CP, cochleariform process; L, left; R, right.
a P value shows the results of independent samples t test.
b P value shows the results of paired samples t test.
c P value shows the results of χ2 test.
Facial canal dehiscence in the tympanic segment was detected: 5.6% (right) and 7.8% (left) in the males and 5.5% (right) and 10.0% (left) in the females (P > .05; Table 1).
Mastoid pneumatization of the both males and females on the right and left sides was not statistically significant (P > .05; Table 1). For the right side, grade 4 (100%) pneumatization was detected more (57.8% in males and 57.3% in females). Grade 0 (0%) pneumatization was detected in the second order, 26.7% in males and 28.2% in females (P > .05). For the left side, grade 4 (100%) pneumatization was detected more (55.6% in males and 57.3% in females). Grade 0 (0%) pneumatization was detected in the second order: 22.2% in males and 28.2% in females (P > .05; Table 1).
Spearman correlation ρ coefficient test results are presented in Table 2: ‒ There were positive correlations between scutum-CP and scutum–promontorium distances bilaterally (P < .05; Table 2). ‒ There were positive correlations between mastoid pneumatization and scutum-CP and scutum–promontorium distances bilaterally (P < .05; Table 2). In more pneumatized mastoids, scutum-CP and scutum–promontorium distances increased. In sclerotic mastoids, scutum-CP and scutum–promontorium distances decreased. ‒ There were no significant correlations between mastoid pneumatization and FCD (P > .05). ‒ There were no significant correlations between age, gender, mastoid pneumatization, FCD, scutum-CP, and scutum–promontorium distances (P > .05).
Correlation Tests.a
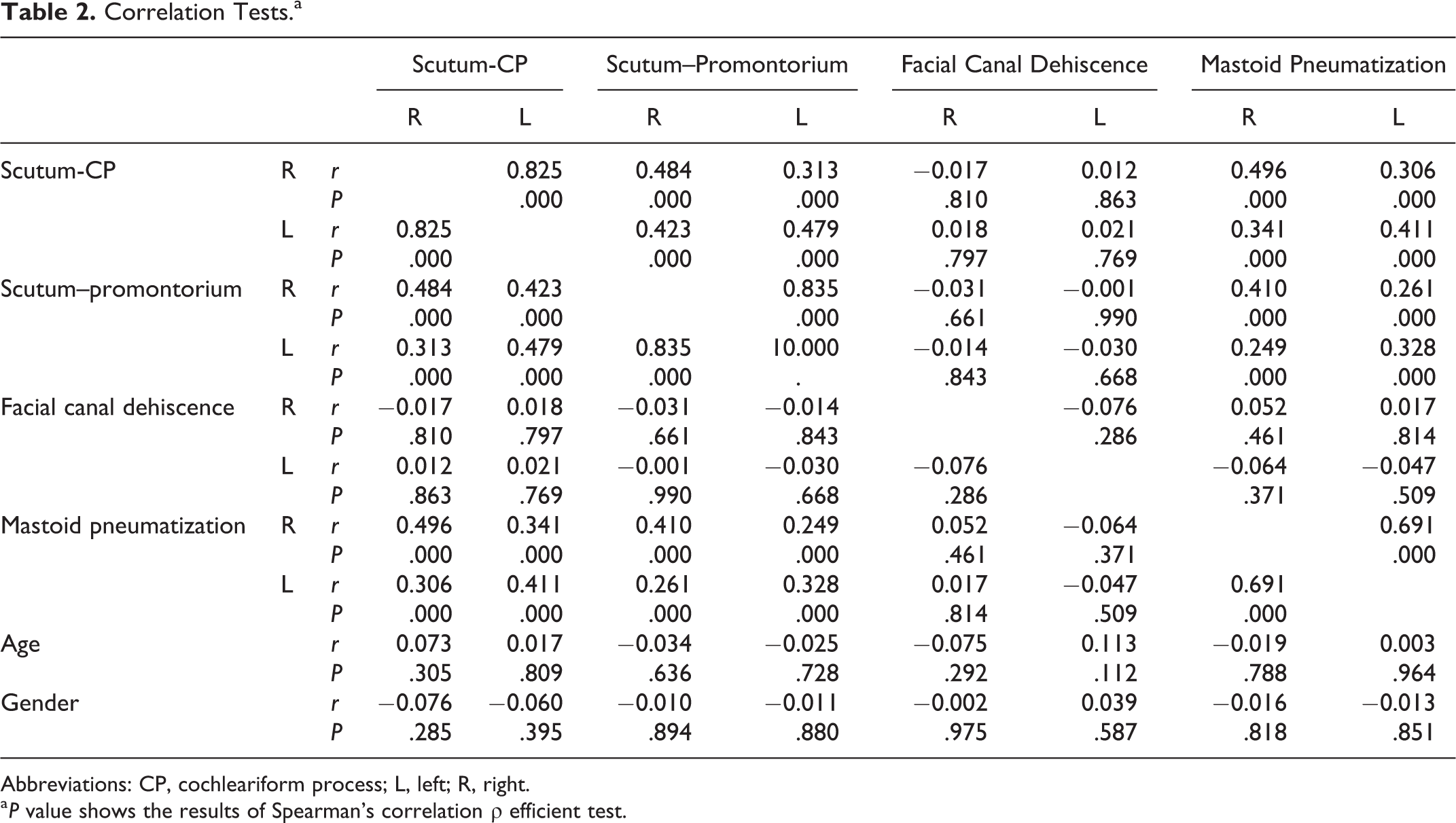
Abbreviations: CP, cochleariform process; L, left; R, right.
a P value shows the results of Spearman’s correlation ρ efficient test.
Discussion
The narrowest points of the facial canal were reported at the level of the meatal foramen. After that, geniculate fossa proximal portion, geniculate fossa bulbous enlargement portion, and distal portion are the other narrowest parts. Also one of the narrowest parts of the facial canal is at the CP level, and at this level, the width of the canal was reported as 1.29 to 1.55 mm. 9,10 The facial canal expands gradually from the meatal foramen to the geniculate fossa. After that, it gradually becomes narrower to the level of the stapes and enlarges to the stylomastoid foramen. 11
Ge and Spector 12 reported that ossification on the facial canal labyrinthine segment occurs before the 15th week of pregnancy. Similarly, ossification is performed in the CP, from the 20th week to the 22nd week of pregnancy. At the 24th gestational week, ossification at the stapes occurs. Between 25 and 27 weeks of gestation, ossification at the pyramidal eminence is detected. 13 In other parts of the horizontal and vertical segments, ossification has delayed, which causes the dehiscence of the bony wall. 11
In the present study, we investigated the relationship between mastoid pneumatization and CP, and the neighboring structures. Because the facial nerve has been found to pass behind the CP and the tensor tympani, it has been recently concluded that the CP is a useful landmark to locate the facial nerve. It is recommended that surgeons can depend on the CP as a fixed landmark for the facial nerve, but not for the geniculate ganglion. 14 Our results showed that the distances between scutum-CP and scutum–promontorium were not different between males and females between and right and left sides. Facial canal dehiscence on the tympanic segment was detected: 5.6% (right) and 7.8% (left) in males and 5.5% (right) and 10.0% (left) in females. In this study, pathologic temporal MDCTs were not included and scutum erosion was not detected. Scutum erosion may be observed in cholesteatoma cases.
Facial canal dehiscence increases the injury to the facial nerve during the ear surgery. Facial canal dehiscence rates were reported as 0.5% to 11.4% in patients not having chronic otitis surgery, such as otosclerosis. 2,15,16 In chronic otitis surgery, FCD rate increases to 33%. 2,17,18 Dehiscences are most commonly found in the tympanic segment, especially in the adjacent tissues of the oval window, but they can also be seen in the geniculate ganglion and even in the vertical segment. 19
In our study, mastoid pneumatization is also evaluated. Grade 4 (100%) pneumatization was detected mainly in 55.6% to 57.8% of the patients in both genders. Grade 0 (0%) pneumatization (sclerosis) was detected in 22.2% to 28.2% in both males and females. In more pneumatized mastoids, scutum-CP and scutum–promontorium distances increased. In sclerotic mastoids, scutum-CP and scutum–promontorium distances decreased. The FCD rates were not related to the mastoid pneumatization levels. It may be because of the development of FCD that occurs during the intrauterine period. As CP is a useful landmark for the facial nerve, the decreased scutum-CP and scutum–promontorium distances must be kept in mind in ear surgeries to avoid facial nerve injury. Additionally, in the presence of FCD, these distances are more important.
In the transcanal endoscopic approach, the second tract of the facial nerve passes toward the surgeon’s instrument. The endoscope allows us to see the structures that directly represent the floor of the epitympanum: “the second tract of the facial nerve, the CP, and the tensor fold.” Particularly the CP and tensor fold with the tensor tympani canal represent “the floor of the anterior epitympanic space.” 20
The scutum is also an important landmark for ear surgeries. One of the early sign of the cholesteatoma abnormalities that can be evaluated in CT scan is the erosion of the scutum with the medial direction of the roof of the external auditory canal where the tympanic membrane attaches superiorly. Scutum erosion can easily be seen in coronal CT images. 21,22
Genç et al 23 reported that the presence of a scutum defect is an important finding in predicting the degree of disease and FCD. They evaluated the operation records of 154 patients with tympanomastoidectomy. The patients had chronic otitis media (with or without cholesteatoma). Rate of the scutum defect was 29.22% and FCD rate was 22.07%. 23 In the present study, FCD in the tympanic segment was detected: 5.6% (right) and 7.8% (left) in males and 5.5% (right) and 10.0% (left) in females. The difference between our study and Genç et al’s 23 study in the aspect of the FCD rates may be related to our patients who did not have chronic otitis media or cholesteatoma.
Conclusion
Cochleariform process is an important landmark to localize the tympanic segment of the facial canal. In sclerosed mastoids, scutum-CP and scutum–promontorium distances decreased. Facial canal dehiscence rates were not related to the mastoid pneumatization levels. It may be due to the development of FCD that occurs during the intrauterine period. In endoscopic and classic ear surgeries, mastoid pneumatization must be evaluated preoperatively to avoid facial nerve injuries.
Footnotes
Author contributions
Mikail Inal and Neşe Asal contributed to planning, designing, data collection, and literature survey. Nuray Bayar Muluk contributed to planning, designing, literature survey, statistical analysis, and writing. Mehmet Hamdi Şahan, Gökçe Şimşek, and Osman Kürşat Arıkan contributed to planning, designing, and literature survey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.