
Abstract
Objective:
To compare the outcomes of adult patients with recurrent epistaxis treated intraoperatively with either bipolar electrocautery or microwave ablation (MWA).
Study Design:
Prospective randomized control study.
Materials and Methods:
One hundred ten patients with idiopathic recurrent epistaxis who met the inclusion criteria were randomly assigned into MWA group and bipolar electrocautery group. Primary outcomes were the proportion of patients in each group whose bleeding had stopped within 24 hours after treatment and time to achieve successful hemostasis. Secondary outcomes were the rebleeding rate after 3 days, 1 and 12 weeks, and 6 months and complications.
Results:
Successful immediate arrest of epistaxis was achieved in all patients. The times to achieve successful hemostasis were 2.13 ± 1.04 minutes in the MWA group and 6.60 ± 2.68 minutes in the bipolar electrocautery group (P = .000). The rates of recurrent bleeding were similar in patients treated with the different approaches (P = .231). However, secondary crusting was observed endoscopically in 59 patients in the bipolar electrocautery group, while pseudomembrane of the ablation zone was seen in 19 (36.5%) patients in the MWA group. Nevertheless, there were no severe postoperative complications, including septal perforation and orbit and brain complications, in either group at the 6-month follow-up.
Conclusion:
Bipolar electrocautery and MWA had similar outcomes for the treatment of adult patients with recurrent epistaxis. However, MWA resulted in rapid hemostasis with less local nasal pain and less crust. Thus, MWA could be a favorable treatment option for patients with idiopathic recurrent epistaxis.
Introduction
Idiopathic recurrent epistaxis is one of the most frequently occurring emergent otorhinolaryngological conditions. Although hemostasis can be achieved by treatment in outpatient departments in many cases, we have encountered some difficult-to-treat cases involving patients with recurrent bleeding. Conventional management pathways dictate that the patient be initially resuscitated, and if the bleeding site cannot be identified, then anterior and posterior nasal packing should be done to arrest the bleeding. 1,2 The use of either bipolar cautery with suction or suction monopolar cauterization is well established for the treatment of recurrent epistaxis with recent advances in endoscopic sinus surgery. 3 -5 In addition, arterial ligation and/or embolization of the responsible vessel, for example, the sphenopalatine artery (SPA), rarely the internal maxillary artery and posterior ethmoidal artery, were also adopted for severe recurrent epistaxis. However, SPA ligation only had the success rates of 87% to 93%. 6 -8
Microwave ablation (MWA) is a relatively new technique which has been used intraoperatively to achieve hemostasis at surgical margins in laparotomy. 9 Many studies have shown that MWA is safe and effective for the treatment of active hemorrhage of the liver 9 and hemorrhaging angiosarcoma, 10 minimizing intraoperative blood loss. In recent years, MWA has also been used to treat epistaxis, and it has shown a high success rate. 11,12 The authors declared that there is any overlapping data with our previously published studies. 11,12
This study compared hemostasis procedures and side effects between MWA and bipolar electrocautery in patients with idiopathic epistaxis emanating from the posterior nasal cavity to Kiesselbach’s area.
Materials and Methods
Ethical Considerations
The study protocol was reviewed and approved by the Institutional Ethical Review Board of Wenzhou Medical College-Affiliated Yiwu Hospital in Yiwu, Zhejiang, China. Informed consent was obtained from all participants.
Study participants were recruited from consecutive patients diagnosed with idiopathic recurrent epistaxis who visited the outpatient Department of Otorhinolaryngology, Head and Neck Surgery, at the Affiliated Yiwu Hospital of Wenzhou Medical College between January 1, 2016, to December 31, 2018. The inclusion criteria were unilateral idiopathic recurrent epistaxis with or without a history of anteroposterior or anterior nasal packing, age >18 years, history of repeated epistaxis with at least 3 episodes in the preceding 2 days, a bleeding point identified endoscopically, only 1 site anatomic region responsible for the bleeding, and showing an isolated bulge of nasal mucosa with a red top. Patients with traumatic epistaxis, bleeding from a tumor, postoperative epistaxis, Osler disease, who used antiplatelet agents or anticoagulants, and multiple bleeding sites or bleeding of unknown origin after endoscopic examination were excluded. Patients with insufficient follow-up and clinical records, bilateral epistaxis, or multiple lesions were also excluded after endoscopic examination. Children were excluded because surgical treatment requires general anesthesia in most children. In addition, the majority of cases of epistaxis in children and recurrent bleeding occur repeatedly due to nose-picking. The bleeding sites were classified according to their anatomical locations: Kiesselbach’s area, the middle and posterior nasal septum, olfactory cleft, middle meatus region, inferior meatus region, and others. The middle nasal concha, middle meatus, and posterior nasal cavity (superior posterior end of the inferior concha) were included in the middle meatus region, whereas the inferior nasal concha and inferior meatus were included in the inferior meatus region. The bottom of the common nasal meatus and anterior nasal roof were classified as others.
Age, sex, duration of bleeding, site of bleeding, concomitant comorbidities (including cardiovascular disease, atherosclerotic disease, diabetes, and so forth), and having been treated with or without nasal packing were recorded at the initial visit. The time to successful hemostasis was defined as the time from first identification of the bleeding points to successful hemostasis.
Technical Details
The procedures were performed in the operating room and then general anesthesia or local anesthesia was selected based on the pain tolerance and physical condition of the patients. The patients were placed in a normal sitting position or the supine position.
The nasal cavity was examined endoscopically to identify the bleeding sites/points prior to randomization. Subsequently, the principal investigator, aided by a registered nurse, allocated patients to various treatments using simple random sampling. Specifically, consecutive patients who met the inclusion criteria and definite bleeding site/point were assigned random numbers generated by SPSS for Windows software (ver.19.0; SPSS, Inc, Chicago, Illinois), which allocated them to the bipolar electrocautery group and MWA group. Informed consent was signed by the patients or family member.
Microwave Ablation Group
Cotton–wool pledgets soaked in 1% lidocaine and 0.1% epinephrine were placed in the nose and bleeding sites 3 times for 5 minutes each time before ablation. When anesthesia was achieved, bleeding points were treated using MWA (EBH-IV microwave therapy; Shanghai Xiyu Electromechanical System Co Ltd, Shanghai, China) equipped with a 2450-MHz cooled-shaft antenna with output power of 60 W. 11
The maximum ablation time of the EBH-IV MWA device was set to 20 seconds, and the footplate-operated switch was used to control the ablation time. The microwave immediately stopped ablating if the footplate-operated switch was deactivated. The microwave application time was 1 to 3 seconds for each ablation treatment; repeated ablation may be performed on the same bleeding point region. The contact-type antenna was used to contact the nasal mucosa or bleeding point; the antenna tip was a split-type double needle with an upward portion. 11 The size of the MWA antenna is similar to the outer diameter of the bipolar cautery or monopolar suction that is commonly used to control epistaxis (Figure 1). In most cases, the length and outer diameter of the microwave antenna allowed it to reach all regions of the nasal cavity under the endoscope (Figure 2). Medial and lateral shifting of the turbinate may increase the space available for the microwave antenna and endoscope in patients with anatomical variation; in addition, the microwave antenna is malleable. The shape of the thermal lesion was elliptical at each ablation, whereas multiple ablations resulted in an irregular ablation zone. The thermal lesion was approximately 2 mm in length and 1 mm in width, which corresponded to or slightly exceeded the length and width of the upward portion of the microwave antenna tip. The depth of penetration of the thermal lesion was approximately 0.5 to 1 mm (Figure 3).
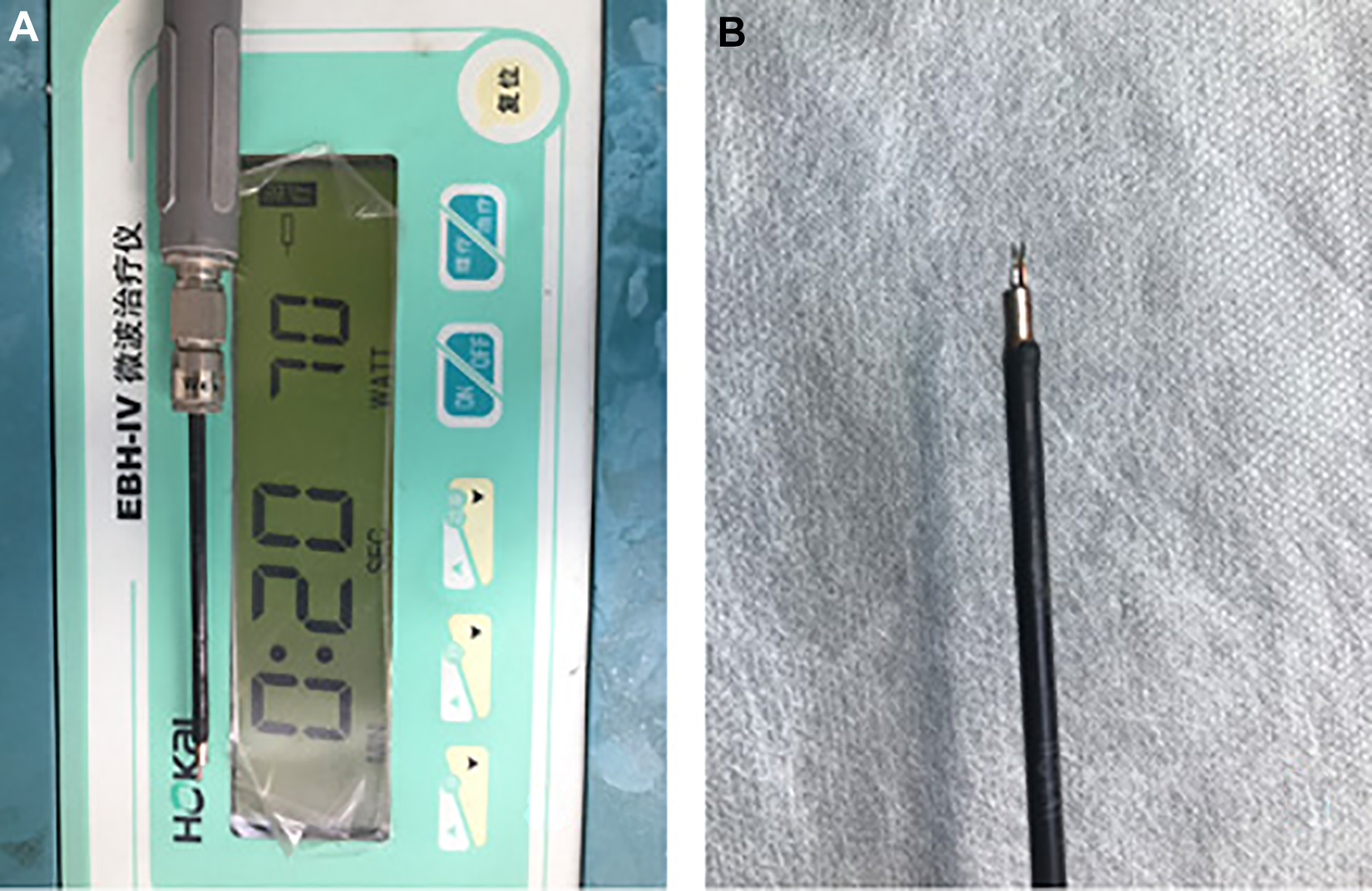
The microwave ablation (MWA) device and cooled-shaft antenna. A, Working parameters of MWA. B, The MWA antenna.
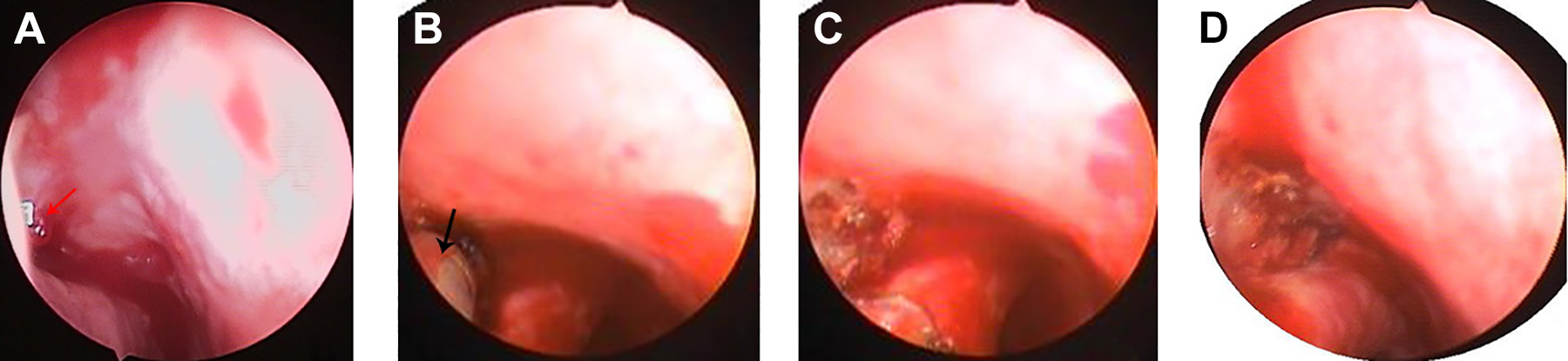
The bleeding point was on the anterior end of the lateral wall of the inferior meatus: isolated primary telangiectasias (A), microwave ablation antenna (B), microwave ablation coagulation (C), and ablation zone (D). Red arrows indicate the bleeding point; black arrows indicate the ablation antenna.

The bleeding point was on the middle inferior nasal septum: isolated primary telangiectasias with active hemorrhage (A), inactive hemorrhage after nasal packing using cotton–wool pledgets soaked in 1% lidocaine and 0.1% adrenaline (B), distal ablation of the bleeding point (C), proximal ablation (D), and microwave ablation coagulation (E).
The bleeding point was endoscopically ablated in a distal to proximal fashion to achieve a uniform light gray color ablation zone in the periphery and the lesion (Figures 3 and 4). When a lesion bled excessively during microwave application, the MWA antenna was placed directly on the lesion to remove the lesion and reduce the blood flow.
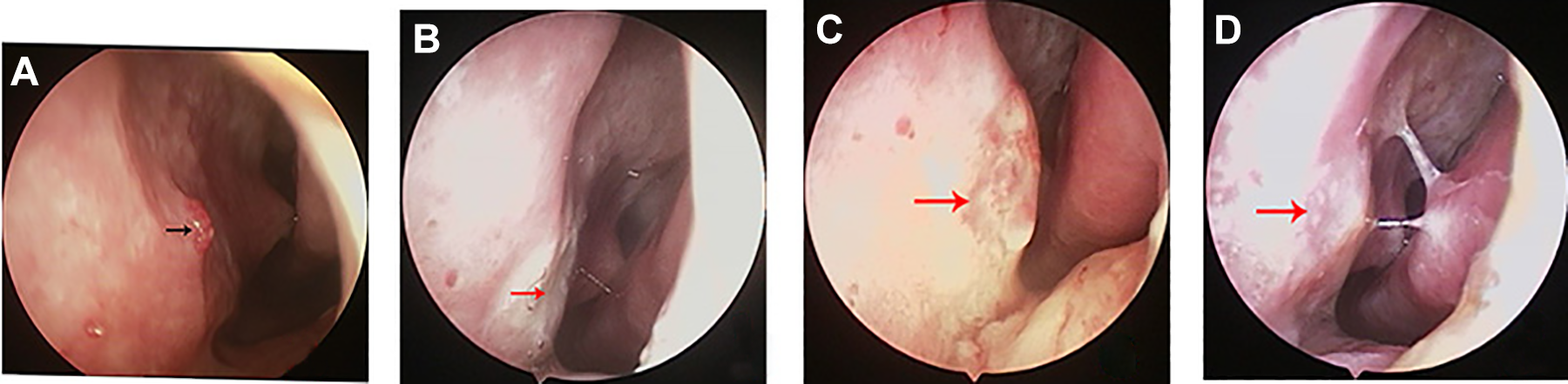
The bleeding point was on the middle inferior nasal septum: isolated primary telangiectasias (A), microwave ablation coagulation (B), 1 week after ablation (C), 2 weeks after ablation (D). Black arrows indicate the bleeding point; red arrows indicate the ablation zone.
Bipolar Electrocautery Group
Cotton–wool pledgets soaked in 1% lidocaine and 0.1% adrenaline were placed in the nose and bleeding sites 3 times for 5 minutes each time before cautery. When anesthesia was achieved, bipolar cautery was performed under endoscopic visualization with bipolar forceps. The power was typically set to 20 W. The bleeding points were endoscopically cauterized in a distal to proximal fashion (Figure 5).
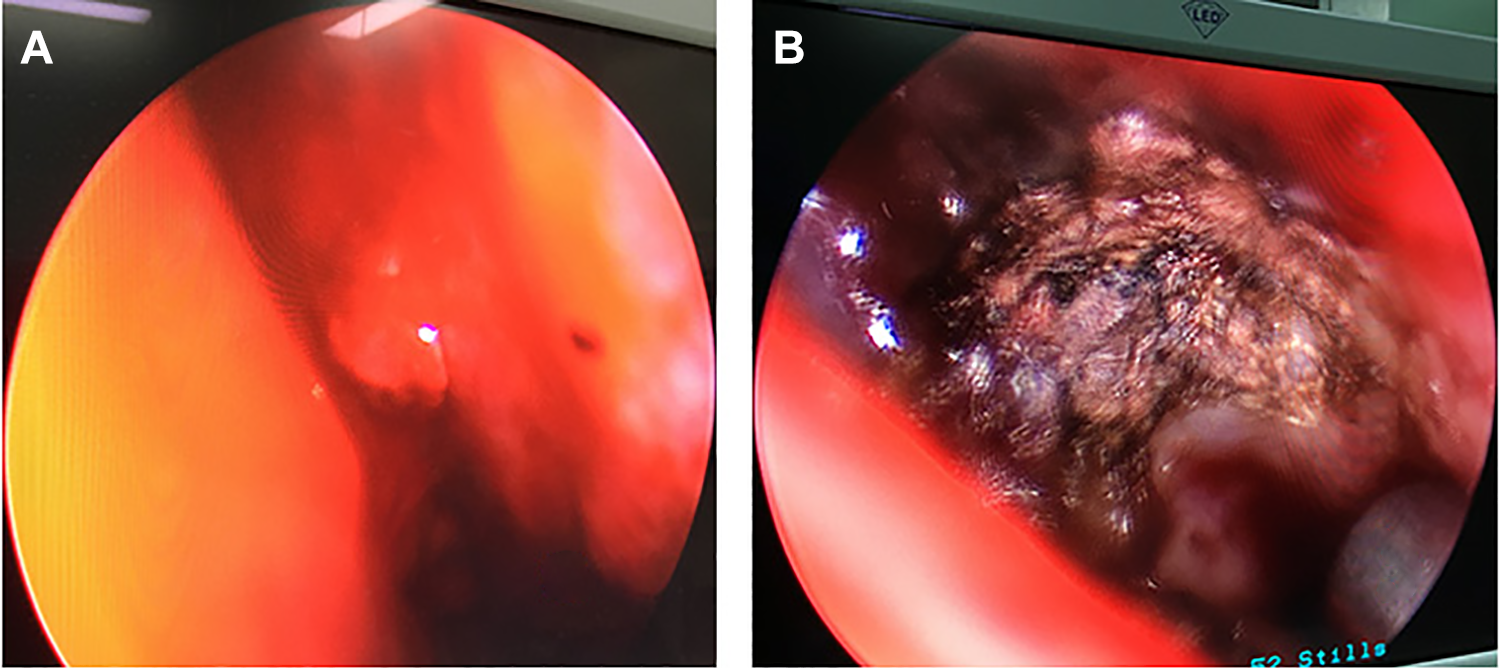
The bleeding point was on the olfactory cleft region: isolated bulge of nasal mucosa with red top (A); bipolar forceps cauterization formed a black crust (B).
All patients were admitted for 3 days after treatment. Patients were reevaluated after 3 days, 1 and 12 weeks, and 6 months. All patients were asked to score their pain on a visual analog scale (VAS) from 0 to 10 on postoperative days 1 and 2.
The primary outcomes were the proportion of patients in each group whose bleeding had stopped within 24 hours after treatment and time to achieve successful hemostasis. Secondary outcomes were the rebleeding rate after 3 days, 1 and 12 weeks, and 6 months and complications. The complications were defined as postoperative crust formation, increasing rhinorrhea, synechiae formation, septal perforation, and orbit and brain complications. Patients were questioned regarding the presence and frequency of bleeding, and the nasal cavity was reexamined endoscopically at each visit. Patients with persistent episodes of epistaxis despite treatment were considered treatment failures and another treatment regimen was ordered. A bleeding event following electrocautery or ablation, confirmed by a doctor and requiring intervention, was considered a recurrent epistaxis event during the follow-up period. Interventions included applying pressure to the nose for more than 5 minutes, additional electrocautery or ablation, arterial ligation/embolization, or nasal packing; however, a few cases of nasal oozing that resolved without intervention were not considered recurrent epistaxis events. The outcomes were blindly assessed by independent clinician.
Statistical Methods
Statistical analyses were performed using SPSS for Windows version 13 (SPSS Inc, Chicago, Illinois). The χ2 test was used to analyze categorical data. The Kolmogorov-Smirnov test was used to evaluate the normality of the distribution of the continuous data. In the case of a normal distribution, the independent samples t test was used, otherwise the Mann-Whitney U test was used. In all analyses, P < .05 was taken to indicate statistical significance. We regarded an absolute difference in the order of 25% as being significant with clinical importance to favor a group for the primary outcomes. To have a 75% power to exclude a difference in this magnitude at a 5% significance level, a total of 100 patients would be required.
Results
Demographic Data
A total of 110 patients with idiopathic recurrent epistaxis met the inclusion criteria; of the 110 patients, 52 patients were in the MWA group while 59 patients in the electrocautery group. The age and sex of the patients, the side of bleeding, frequency, duration of epistaxis, with or without preexisting nasal packing, anesthesia method, concomitant comorbidities, and operating room versus outpatient clinic were matched between the groups (P > .05; Table 1). The bleeding sites were also matched between the groups (P > .05; Table 2). The bleeding points showed an isolated bulge of nasal mucosa with a red top in 63 patients and similar isolated primary telangiectasias in 47 patients.
The Comparison of Demographic Variables Between the 2 Groups.a
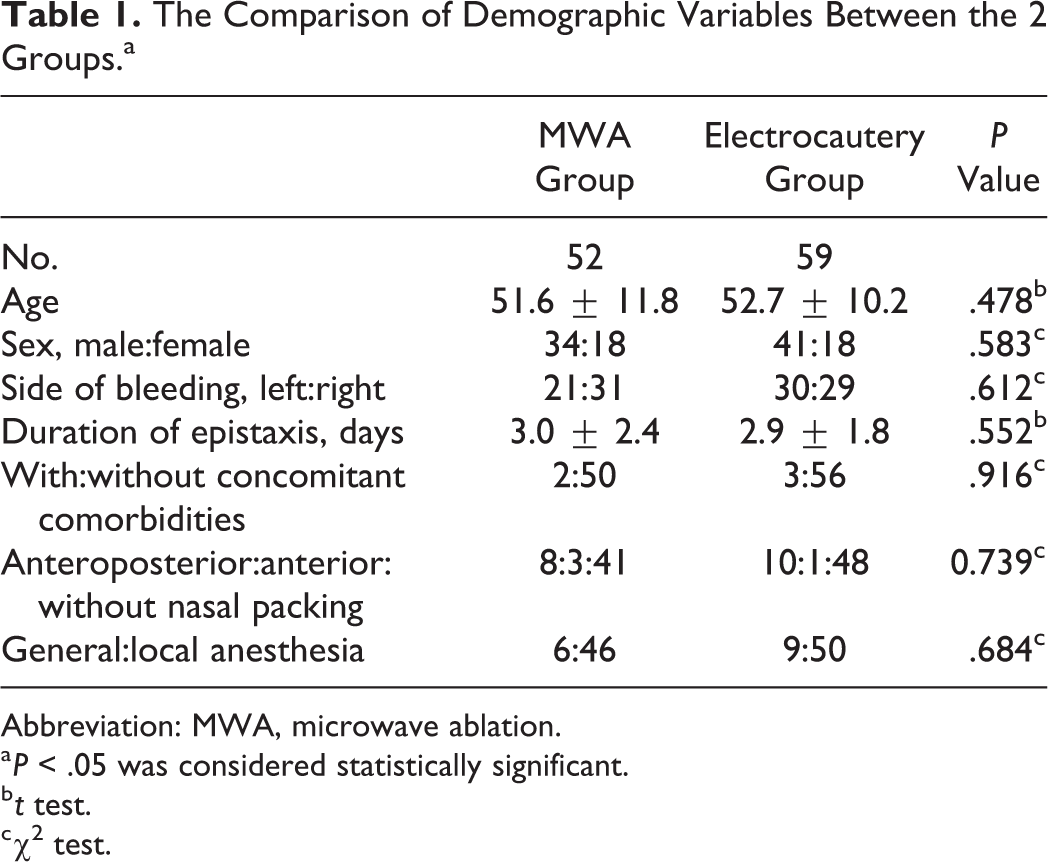
Abbreviation: MWA, microwave ablation.
a P < .05 was considered statistically significant.
b t test.
c χ2 test.
The Comparison of Bleeding Site Between the 2 Groups.a
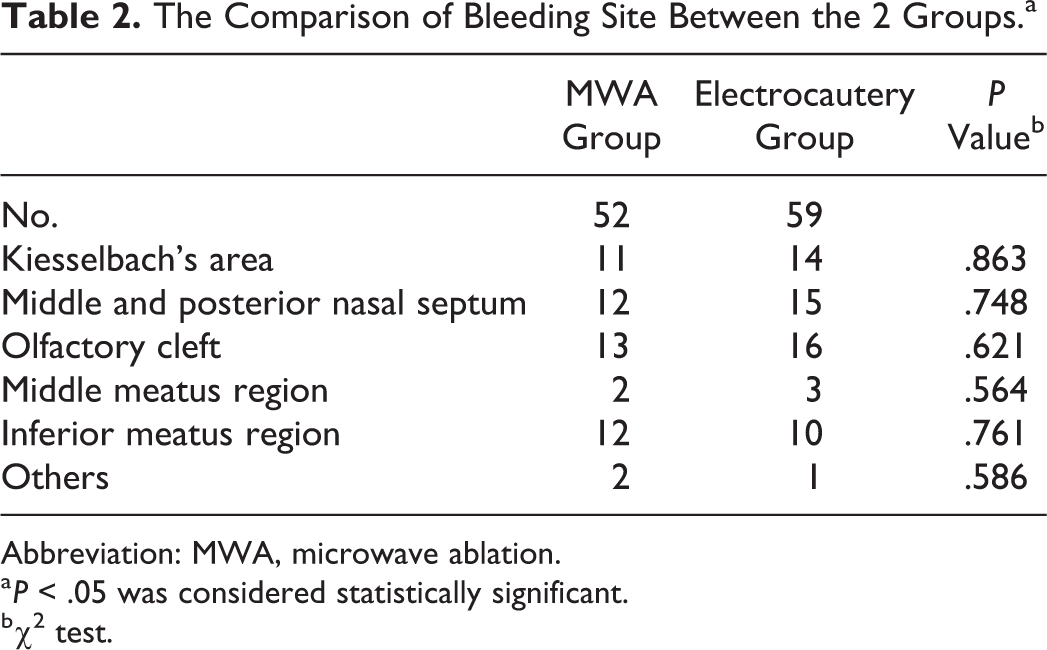
Abbreviation: MWA, microwave ablation.
a P < .05 was considered statistically significant.
b χ2 test.
Primary Outcome
The outcome measures of the 2 groups are shown in Table 3. Successful immediate arrest of epistaxis was achieved in all patients. The average times to achieve successful hemostasis were 2.13 ± 1.04 minutes in the MWA group and 4.60 ± 2.68 minutes in the bipolar electrocautery group (P = .000). Only 1 patient in the bipolar electrocautery group had an epistaxis event within 24 hours after treatment and required anterior nasal packing using Merocel (The medical company of XOMED in USA). However, as operative instruments damaged the nasal mucosa, nasal oozing occurred after treatment in 14 (26.9%) patients in the MWA group and in 18 (30.5%) patients in the bipolar electrocautery group (P = .47). The additional cost benefit was the same between the 2 groups. The cost–benefit analyses only included the equipment costs, and cost-effectiveness of treatment was 79 Renminbi (RMB; approximately US$13.17) in the MWA group and 152 RMB (approximately US$25.33) in the bipolar electrocautery group.
The Outcome Measures of the 2 Groups.
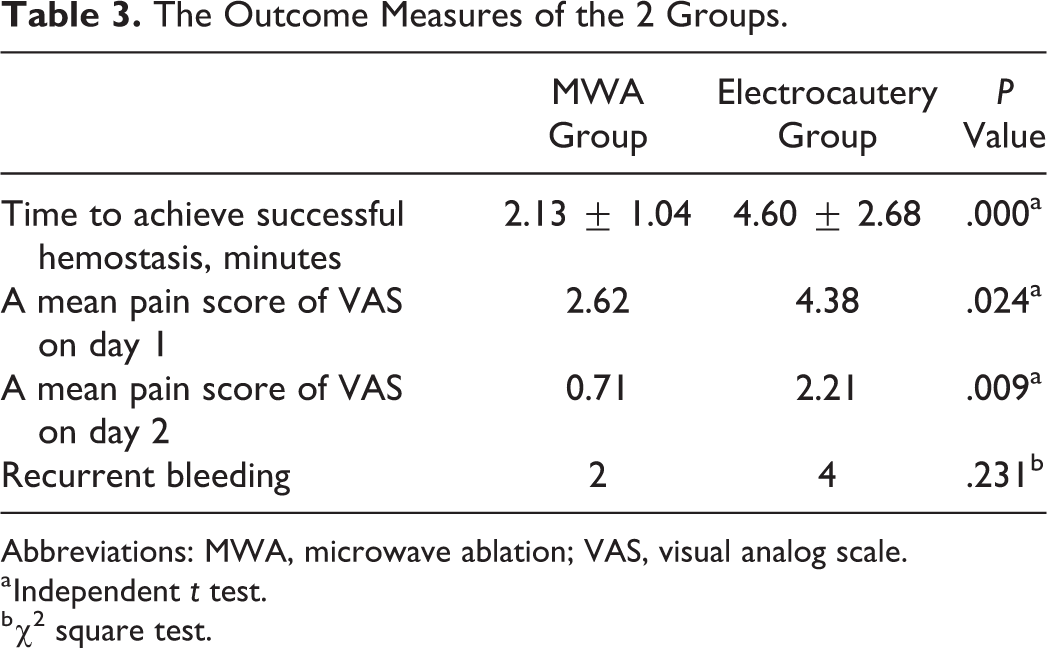
Abbreviations: MWA, microwave ablation; VAS, visual analog scale.
a Independent t test.
b χ2 square test.
Secondary Outcomes
The mean pain scores on days 1 and 2 were 2.62 versus 4.38 (P < .05) and 0.71 versus 2.21 (P < .05) in the MWA group and the bipolar electrocautery group, respectively. All of the patients were followed up at 6 months. Rebleeding was encountered in 4.5% of the patients, and 95.5% of the patients did not have bleeding during the follow-up period. One patient had rebleeding at 5 weeks after treatment in the bipolar electrocautery group, but endoscopic findings showed that the bleeding point was different from the original bleeding point, and therefore, the patient was not included in those with recurrent bleeding. Recurrent bleeding was experienced by 2 (3.8%) patients treated with ablation and by 4 (6.7%) patients treated with bipolar electrocautery. The rate of recurrent bleeding was similar between the 2 treatments (P = .231). However, during this period, no patients in this series required arterial ligation/embolization for recurrent bleeding.
Complications
All of the patients in the bipolar electrocautery group had a black crust at 3 days and 1 week after treatment, which disappeared at 12 weeks and 6 months. However, no black crust was seen after 3 days and 1 week in the MWA group, and only the ablation zone was covered by a light gray pseudomembrane in 19 (36.5%) patients. The electrocautery area or ablation zone showed normal nasal mucosa for all patients at 12 weeks and 6 months after treatment.
Increased rhinorrhea was observed in 32 (54.2%) patients in the bipolar electrocautery group but in only 14 (26.9%) patients in the MWA group within 1 week following the procedures (P < .05). None of the patients in either group complained of increased rhinorrhea at 12 weeks and 6 months after treatment. In addition, synechiae formation in the middle turbinate and nasal septum was seen endoscopically in only 1 patient in the electrocautery group at 6 months, but there were no severe postoperative complications (including septal perforation and orbit and brain complications) in either group at 6-month follow-up.
Discussion
Efficient epistaxis management requires the identification of bleeding points because it allows control by cauterization and reduces the need for more complex procedures that can prolong hospital stay, increase patient morbidity, and place demands on hospital resources. 1 Anterior and posterior nasal packing should be done previously in patients with idiopathic recurrent epistaxis, and endoscopic electrocautery of the responsible vessel/bleeding point, 2,3,13 arterial ligation, and/or embolization 6 -8 have also been considered for severe epistaxis.
However, rebleeding usually occurs when nasal packing material cannot be accurately packed into a bleeding site/point. In addition, arterial ligation of responsible vessels is associated with high failure rates due to multiple branches of the SPA. 6 -8 Microwave ablation is a minimally invasive therapeutic technique that has mainly been used for the treatment of active hemorrhage of the liver in cases of trauma or ruptured vascular tumors. 9,10,14 Some studies have shown that MWA is useful for controlling life-threatening hemorrhages even when active bleeding occurs in a large-diameter vessel. 9,10,15 Microwave ablation has also been used to treat hypertrophic rhinitis, allergic rhinitis, and epistaxis in China. 11,12,16,17 However, few studies have compared MWA and bipolar electrocautery with regard to control of recurrent epistaxis in adult patients.
In this study, 52 cases of idiopathic recurrent epistaxis were successfully controlled by MWA in patients with a known bleeding site. Compared to bipolar electrocautery treatment, MWA significantly reduced the time to achieve successful hemostasis (2.13 ± 1.04 vs 6.60 ± 2.68 minutes, respectively; P < .05), and the reduced duration of treatment with MWA means a shorter anesthetic and/or reduced patient discomfort if completed under local anesthesia in an awake patient. Microwave heating occurs in a volume around the applicator antenna, while bipolar electrocautery heating is limited to areas of high current density. Bipolar electrocautery heating requires an electrically conductive path, while microwaves are capable of propagating through materials with low or zero conductivity. 18 In addition, the bipolar cautery tip is not easy to use in the nose, particularly in narrow spaces, such as the superior olfactory cleft and inferior meatus. By contrast, the microwave device is similar to monopolar cauterization that tends to be very easy to use in the nose. More importantly, bipolar cautery is needed to achieve hemostasis after lesion removal, while the use of MWA enables both lesion removal and hemostasis with the same instrument. Moreover, the adjustable tines of the forceps measure only up to approximately 8 mm, and therefore, multiple hemostasis procedures need to be performed for prominent large-diameter vessels. 5 However, MWA has the advantage of achieving a consistent tissue temperature and covering a larger volume, thus theoretically leading to faster ablation time and a larger area of coagulation, resulting in rapid hemostasis. 19 In addition, MWA can be used with equal efficacy for actively bleeding lesions if the lesion has bled excessively during the application of microwaves. In our study, the application time for microwaves was about 1 to 2 minutes in most cases.
The mean VAS pain scores on days 1 and 2 in the MWA group were significantly lower than those in the bipolar electrocautery group. In a previous study, the microwave antenna of MWA in the target tissue only obtained an average local temperature of 65°C to 100°C, 15 while in another study bipolar electrocautery produced average temperatures of >400°C that may injure normal surrounding tissue and perichondrium or periosteum, thereby causing significant nasal pain. 5 In that latter study, even when performed properly, there was minor black crusting in the bipolar cautery group, so patients treated with bipolar electrocautery were more likely to have black crust formation compared to the MWA because of the high temperatures of >400°C and multiple electrocautery. Although there were no significant differences in epistaxis recurrence rates between the 2 groups, the black crust tended to adhere to the cauterized tissue causing rebleeding when the crust was removed. 5 Nevertheless, a light gray pseudomembrane covered the ablation zone in 19 patients with larger lesions in the MWA group. This may have been related to pathological changes during microwave coagulation. 20 In addition, only 1 patient had synechiae formation between the middle turbinate and nasal septum in the electrocautery group at 6 months. Theoretically, the low temperatures (typically less than 100°C) of MWA and the smaller outer diameter of the MWA antenna caused less injury to adjacent tissues.
No severe complications, such as septal perforation or orbit and brain complications, were encountered during the follow-up period. The use of a cooled-shaft antenna prevented excess carbonizing and thermal injury of the ablation zone in the MWA group. 21 In addition, a footplate-operated switch was used to control the ablation time. A contact-type antenna was used to contact the nasal mucosa or bleeding point. The thermal lesion was approximately 2 mm in length and 1 mm in width, with a thermal lesion penetration depth of approximately 0.5 to 1 mm at each ablation. 11 Therefore, MWA was not able to deeply penetrate the proximity of the orbit and brain and cause orbit and brain complications. However, it should be noted that multiple electrocautery or ablation should be avoided in the same area of septal cartilage to avoid necrosis and perforation of the nasal septum. Moreover, MWA and bipolar electrocautery have similar cost efficiency (US$13.17 vs US$25.33, respectively). Thus, MWA could be a favorable treatment option for patients with severe recurrent epistaxis. Further studies in multiple centers and larger numbers of patients are recommended to clarify the effectiveness and safety of such treatment options. However, this study had limitations including potential heterogeneity in the size, nature, and severity of lesions that may have affected comparison of the outcomes between the 2 groups.
Conclusion
No previous studies have compared intraoperative bipolar electrocautery and MWA. While both are safe and effective for treating recurrent epistaxis in adults, MWA resulted in rapid hemostasis with slight local nasal pain and less crust formation. Therefore, MWA may serve as another option to stop bleeding that is applicable to adult patients with recurrent epistaxis. This method is simple, convenient, and inexpensive and can rapidly achieve hemostasis. Nevertheless, the bleeding sites/points must be identified prior to MWA and electrocautery. Although no complications were encountered in the present study, ablation should be performed with caution, and the patient should be informed of the associated pain and risk of septal perforation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.