
Abstract
Objective:
We aim to describe the parotid fascia as a landmark that can help identify the immediately underlying facial nerve trunk.
Methods:
Dissection of the parotid fascia and identification of the facial nerve trunk were carried out on 8 fresh cadaveric parotid glands. The attachments and arrangement of the parotid gland and its fascia were evaluated and histologically assessed, with special attention to the fascia overlying the facial nerve trunk.
Results:
The parotid fascia envelops the posterior aspect of the parotid gland in an open-book fashion. Posteriorly, it connects to the anterior and medial aspect of the mastoid tip. Posterosuperiorly, it attaches to the inferior aspect of the tragal pointer. Directly medial to the fascia lies the facial nerve trunk.
Conclusion:
The parotid fascia, particularly the parotid–mastoid segment overlying the facial nerve trunk, can be utilized as an additional landmark of depth to help identify the facial nerve trunk during a parotidectomy in conjunction with other commonly used standard anatomic landmarks. The parotid fascia sling spans from the mastoid and tragal pointer to the parotid gland and can be easily palpated intraoperatively. Once the fascia is removed, the facial nerve trunk is identified.
Introduction
Critical to successful parotid surgery is complete tumor removal and safe identification and preservation of the facial nerve. There are a number of accepted anatomic landmarks used to locate the facial nerve, including the use of the tragal pointer, 1 the tympanomastoid suture line 2,3 ; the attachment of the posterior belly of the digastric muscle to the mastoid tip 4 ; and the styloid process 5 (Figure 1). Despite these anatomic markers, it can be a challenging and time-consuming process. The final plane of dissection through the parotid gland fascia uncovers the facial nerve trunk. Until this layer is meticulously opened, the facial nerve trunk cannot be identified. In this way, the parotid gland fascia lends itself as a landmark of depth to identify the facial nerve trunk.
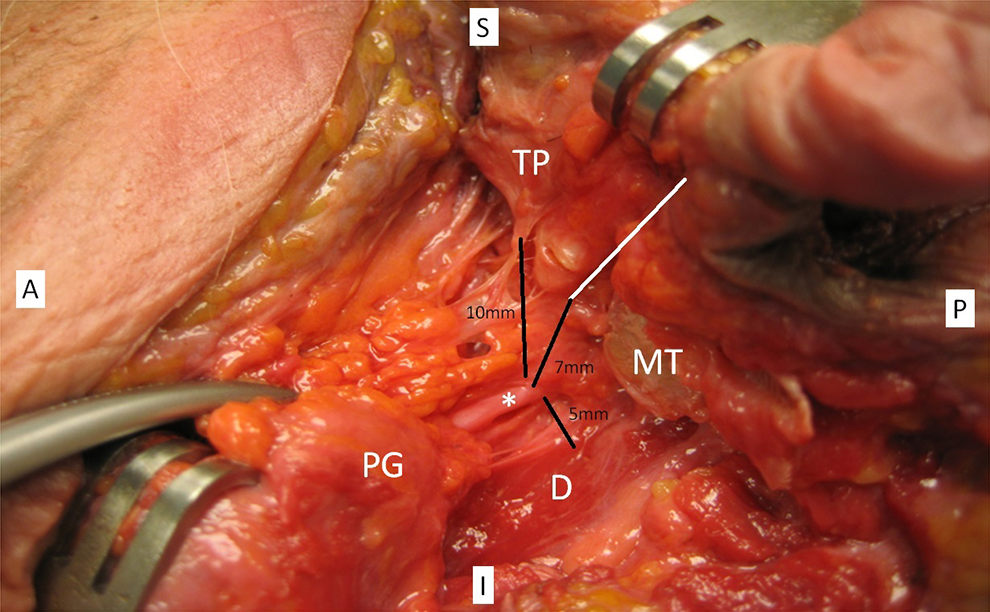
Left parotid gland, delineating common landmarks to the facial nerve trunk (*) and distances. Tragal pointer (TP), tympanomastoid suture (white line), digastric (D), mastoid tip (MT), and parotid gland (PG).
The parotid fascia refers to the investing layer or superficial layer of the deep cervical fascia of the neck that envelops the parotid gland. 6 It covers both the deep and the superficial part of the gland. The superficial layer of the deep cervical fascia divides posterior to the angle of the mandible and anterior to the sternocleidomastoid muscle to form a capsule around the parotid gland. 7 The sheath is tough except medially where the gland may or may not approximate with the pharynx. 8 While the parotid gland fascia therefore lends itself as a potential landmark of depth to identify the facial nerve trunk, it has not been well described. For the purposes of our study, we refer to the portion of the parotid gland fascia directly overlying the facial nerve as the parotid-mastoid fascia.
The goal of this study was to investigate the attachments, anatomy, and histology of the parotid-mastoid fascia overlying the facial nerve trunk. We aim to assess how this fascial layer could be used to provide an additional helpful landmark, in conjunction with other well-known landmarks, to identify the facial nerve trunk during parotidectomy.
Methods
An exemption was granted for this work through the Kaiser Permanente Northern California institutional review board. Eight fresh frozen cadaveric parotid glands were dissected by a senior-level otolaryngology resident and attending. All parotid glands were approached in the same manner. First, a pretragal incision was made, and sharp dissection was utilized to raise a subcutaneous/skin flap off of the parotid fascia. The parotid gland was then separated from the sternocleidomastoid muscle posteriorly. It was also raised off the lateral aspect of the mastoid tip. The landmarks of the tragal pointer, the tympanomastoid suture line, and the attachment of the posterior belly of the digastric muscle to the mastoid tip were also utilized to identify the general area of the facial nerve trunk. The attachments of the parotid fascia overlying the facial nerve trunk were left intact. The parotid fascia was lifted laterally, and the facial nerve trunk was identified just medial to this fascia in antegrade fashion. The attachment of the fascia was assessed and photo documentation performed.
Histopathological analysis was then completed. Fresh cadaveric specimens of the parotid, parotid-mastoid fascia, and facial nerve trunk were taken en bloc and placed in 10% formalin solution prior to routine embedding in paraffin. After fixation, the slides were sectioned according to standard protocol in axial and coronal planes. Sections of 4 µm thickness were stained with hematoxylin-eosin (HE) or trichrome, which is exceptional for visualizing fascia. Histological findings were then further correlated with gross cadaveric findings.
Results
The attachments of the posterior parotid fascia were analyzed in all specimens, with specific attention to the parotid fascia overlying the region of the facial nerve trunk. (Figure 2) In all specimens, the facial nerve trunk was easily identified upon lifting off the parotid gland fascia. The parotid fascia was thicker posterior inferiorly. It enveloped the posterior aspect of the gland in an open book fashion (Figures 3 and 4). Posterosuperiorly, it attached to the tragal pointer and the cartilaginous external auditory canal. The fascia was thinner in this region. Posterioinferiorly, the fascia was thicker with a dense attachment to the anterior and medial aspect of the mastoid tip. There was also a dense attachment to the space between the mastoid and the tragal pointer. In all cases, the posterior attachment of the parotid fascia could be palpated as a taut sling overlying the facial nerve.
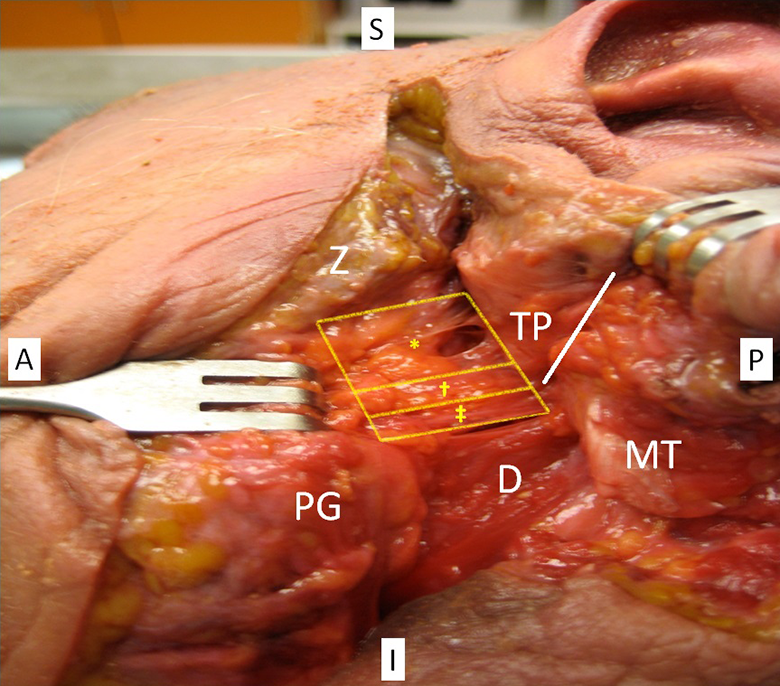
Left parotid gland with parotid-mastoid fascia separated into thin (*), intermediate (†), and thick (‡) components. Zygoma (Z), tragal pointer (TP), parotid gland (PG), mastoid tip (MT), digastric (D), and tympanomastoid suture (white line).
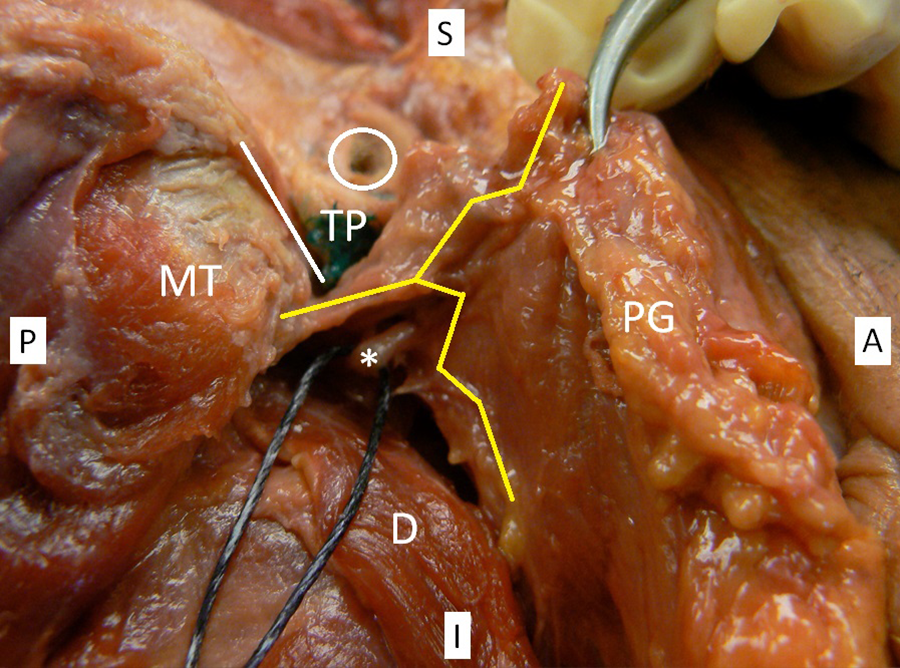
Right parotid gland with auricle removed. Parotid fascia in open-book configuration (yellow line) around the parotid gland (PG) and superficial to the facial nerve (*). Mastoid tip (MT), tragal pointer (TP), tympanomastoid suture (white line), external auditory canal (white circle), and digastric (D).
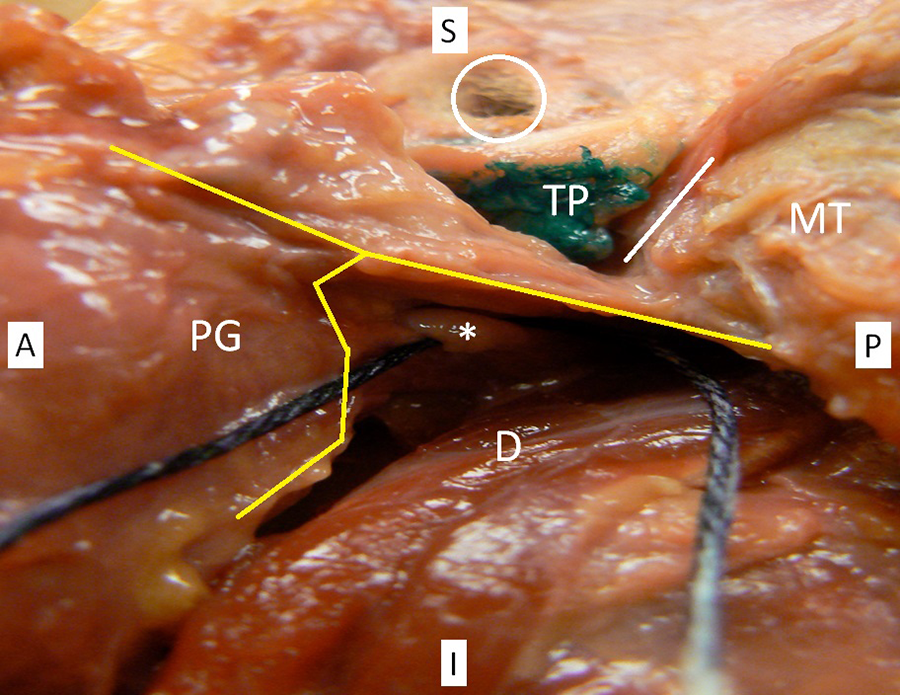
Left parotid gland with auricle removed. Parotid fascia in open-book configuration (yellow line) around the parotid gland (PG) and superficial to the facial nerve (*). Mastoid tip (MT), tragal pointer (TP), tympanomastoid suture (white line), external auditory canal (white circle), and digastric (D).
Histopathological analysis was completed and correlated with the anatomical dissections. The relationship of the parotid-mastoid fascia to the facial nerve trunk was further elucidated with coronal and axial sections as illustrated in Figures 5 and 6. The histology shows a substantial, intervening segment of the parotid-mastoid fascia situated deep to the parotid parenchyma and just superficial to the facial nerve trunk. This facial layer can also be morphologically different in obese patients, with adipose tissue interspersed in layers within the parotid-mastoid fascia. Figure 7 shows an axial cut through the parotid gland, facia, and nerve with trichrome stain. Here the parotid-mastoid fascia is anchored to the gland with interspersed septations extending into the deep aspect of the superficial lobe of the parotid gland.
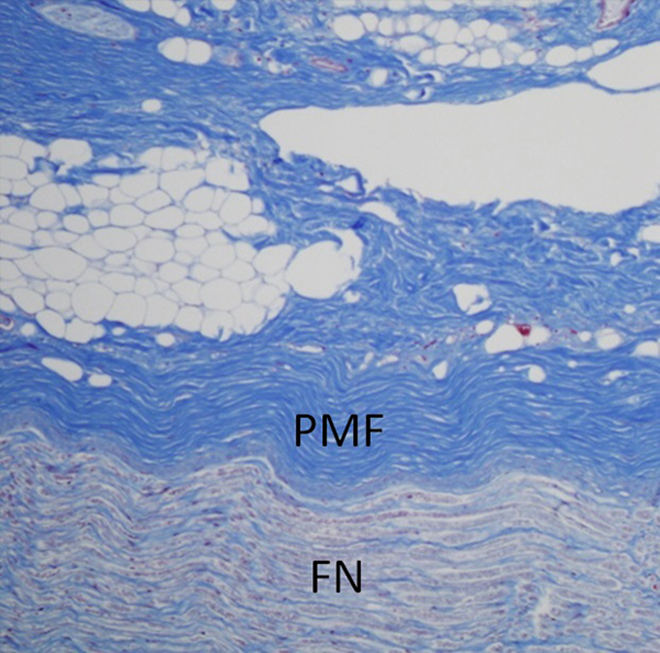
Histological example specimen of a coronal section through the facial nerve (FN) trunk and the overlying parotid-mastoid fascia (PMF) with trichrome stain.
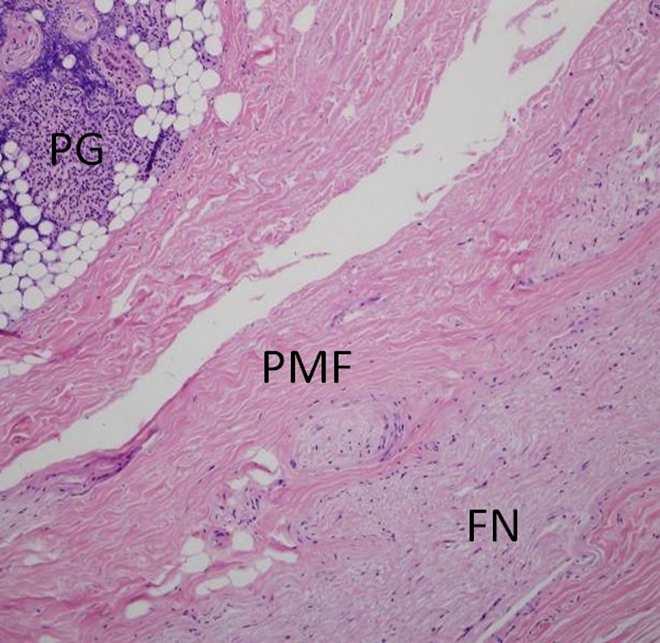
Histological example specimen of an axial section through the facial nerve (FN) trunk and the overlying parotid-mastoid fascia (PMF) on hematoxylin-eosin (H&E) stain. Additional parotid gland (PG) parenchyma is seen in relation to the underlying fascia.
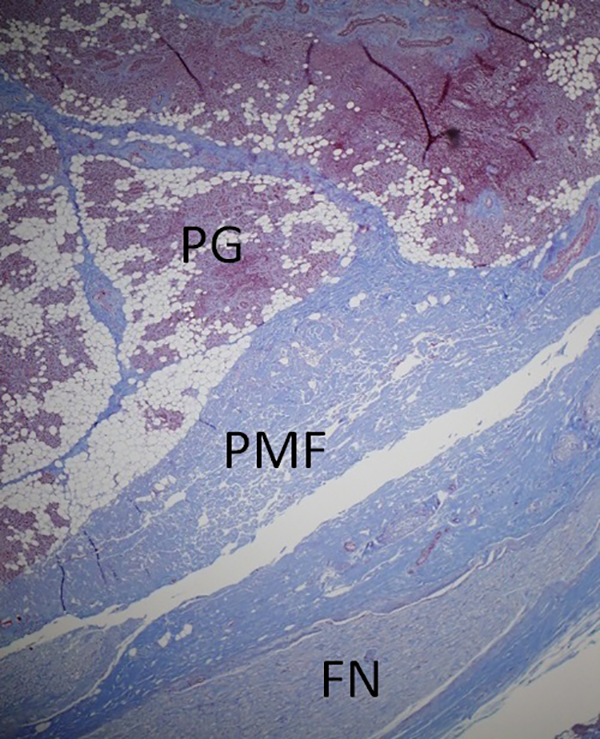
Histological example of an axial section through the facial nerve (FN) trunk using trichrome stain. The overlying parotid-mastoid fascia (PMF) is seen with septations extending into the substance of the parotid gland (PG).
Discussion
The goal of a successful parotid surgery is complete tumor removal and safe identification and preservation of the facial nerve. 9 There are 2 conventional approaches to finding the facial nerve trunk: antegrade and retrograde. Multiple landmarks have been studied to help identify the facial nerve trunk. Lathrop first described the relationship of the facial nerve trunk with the styloid process. 5 The styloid process was positioned deep, above, and in front of the main trunk. Eddey et al demonstrated the facial nerve trunk is 5 to 6 mm inferior and medial to the tragal pointer. 1 Kratz and Hogg showed that the nerve exits from the stylomastoid foramen 6 to 8 mm medial to the inferior end of the tympano-mastoid fissure. 2 The digastric muscle was shown to provide an accurate depth for the facial nerve trunk dissection, although care must be taken when retracting as this soft tissue landmark may be displaced and mislead the inexperienced surgeon. 4,10
More recently, Ji et al provided a systematic review, reporting average distances of the landmarks to the facial nerve trunk. 11 Yet while these landmarks are useful in guiding the surgeon to the area of the facial nerve, they give little information about the depth of the dissection at which to find the facial nerve trunk. This can create a challenge for the new or inexperienced parotid surgeons who often sacrifice speed and efficiency for fear of transecting the nerve. Furthermore, the relationship of the nerve with many of these landmarks can vary slightly and often becomes apparent only after the facial nerve trunk has already been identified.
In the present study, the dense and easily palpable bands of parotid-mastoid fascia attaching to the mastoid acted as a good landmark of depth in finding the facial nerve. Only after these bands are taken down, can the trunk be identified. The majority of studies concerning this fascia have done so in the context of facelift surgery and focus primarily on the parotid fascia, as it approximates the superficial musculoaponeurotic system (SMAS) layer, rather than its relationship with the facial nerve trunk. 6,12 -16 The findings in these studies have been varied. In 1976, Mitz and Peyronie first described the parotid fascia as discrete and deep to the SMAS. 16 The SMAS is described as being thicker in the pretragal region overlying the parotid gland. 13,16,17 The SMAS concept was rejected by Jost and Levet who believed there was only 1 anatomic structure deep to the dermis, described as the primitive platysma or the parotid fascia that was attached to the platysma inferiorly. 14 Further studies by Gosain et al describe the SMAS as distinct from the parotid fascia, with a plane of fat separating them. 12 Stuzin et al described the parotid fascia as part of the deep facial fascia and the SMAS as part of the superficial facial fascia. 13 Trussler et al described the parotid-mastoid fascia, although his team used the term parotid temporal fascia. 15 The parotid temporal fascia’s attachments to the zygoma in relation to the frontal branch of the facial nerve were reviewed in detail in the context of performing a high-SMAS facelift. They confirmed a distinct fascial layer separating the frontal branch from the temporoparietal fascia. Yet, none of these studies evaluated the parotid fascia as an anatomic landmark for localization of the facial nerve trunk itself.
As shown in the present study, this temporoparietal fascia described by Trussler et al is in fact the superior extension of the parotid-mastoid fascia overlying the facial nerve trunk and is itself independent of the SMAS and the superficial layer of the deep cervical fascia. We hypothesize that the parotid-mastoid fascia may have origins from an evolutionary standpoint as a final protective layer to the facial nerve from avulsion injuries.
Ramsaroop et al did discuss the parotid-mastoid fascia as it relates to the facial nerve trunk. He described the parotid fascia as being thick in the upper two-thirds of the parotid region and thinner in the lower one-third as it blended with the platysma muscle. 17 The fascia attached to the tip of the mastoid across the cartilaginous part of the external acoustic meatus to the lower border of the zygomatic process of the temporal bone. Superiorly, it extended to the zygomatic arch and inferiorly it extended towards the upper cervical region.
Similarly, we found in our study that the parotid fascia overlying the nerve attached to the mastoid posteriorly and that the attachment of this fascia at the anterior and medial aspect of the mastoid was quite thick and dense. Posterosuperiorly, it attached to the space between the mastoid and the tragal pointer, and again this was dense and adherent. Anterosuperiorly, it attached to the tragal pointer more loosely. The dense bands of fascia attaching to the mastoid acted as a good landmark of depth in finding the facial nerve. Until these dense bands are taken down, the trunk cannot be identified. This attachment is easily palpable intraoperatively.
While Ramsaroop et al felt that identifying this fascia precluded the need for identification of well-documented landmarks for identification of the facial nerve trunk in most cases, 17 our findings suggest that the initial dissection should proceed to identify the commonly accepted landmarks, particularly the tympanomastoid suture, the tragal pointer, and the posterior belly of the digastric muscle. Once these structures are identified, the general location of the facial nerve trunk can be isolated. At this point, the posterior attachment of the parotid fascia to the mastoid can be a useful landmark of depth and should be easily palpated as a tense band. Caution must be taken at this point, as the facial nerve trunk lies immediately deep to this facial plane. Once the fascia is divided, the facial nerve trunk can be easily identified and traced distally in antegrade fashion to complete the remainder of the parotidectomy.
Conclusion
In conclusion, commonly accepted landmarks are useful in guiding the surgeon to the general location of the facial nerve trunk, but they do not provide the surgeon with a reliable marker for the actual depth of dissection. In addition, these landmarks and their relationship with the facial nerve trunk are most clearly delineated after the trunk is identified. Here, we have described the anatomy of the parotid-mastoid portion of the parotid fascia in the region overlying the facial nerve trunk. We propose that the parotid fascia acts as a useful guide of true anatomic depth in identifying the trunk of the facial nerve, as it lies just superficial or lateral to the nerve trunk and can be both visualized and palpated. We believe that the parotid-mastoid fascia should be used in conjunction with other well-known anatomical landmarks to safely and efficiently identify the facial nerve trunk during parotid surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.