
Abstract
The purpose of this study was to compare the success rates and hearing outcomes of transcanal composite chondroperichondrial cartilage graft with that of underlay temporal muscle fascia (TMF) graft for myringoplasty. In this retrospective study, the medical records of patients who underwent type 1 myringoplasty between September 2015 and February 2018 at Otorhinolaryngology Department of Erzurum Ataturk University were reviewed. Demographic properties, preoperative otological findings, preoperative pure ton audiogram findings, postoperative pure ton audiogram findings, and duration of surgeries were reviewed from medical records. The patients with lack of one or more of these information at medical records or lost to at least 3 months of follow-up were excluded from the study. According to the graft material used in the operation, the patients were divided into 2 groups. The patients operated with cartilage graft by transcanal composite chondropericondrial cartilage graft myringoplasty (TCM) technique was regarded as first group, while patients operated with temporal fascia was regarded as the second group (TMF). Both groups were compared according to preoperative and postoperative air–bone gap (ABG), graft acceptance rate, and duration of operation using SPSS version 20.0 software. A total of 113 patients whose medical records met the inclusion criteria were included in the study. Of these, 59 underwent TCM and 54 underwent TMF myringoplasty. Tympanic membrane perforation closure success rate was higher in the cartilage group (94.9%) than in the fascia group (83.3%; P = .046). In the former, preoperative and postoperative ABG was 19.5 ± 5 and 10.8 ± 4.8 dB, respectively. In the latter, the corresponding values were 20.7 ± 5.4 and 11.5 ± 5.4 dB, respectively (P < .05). Duration of surgery was 29.5 ± 3.4 minutes in the TCM group and 61.5 ± 6.0 minutes in the TMF group (P < .05). Transcanal cartilage myringoplasty could be considered as an appropriate surgical option because of its simplicity, shorter operation time, and rapid patient recovery, with no significant difference in terms of hearing outcomes compared to temporal fascia.
Introduction
Myringoplasty, a surgical procedure for closure of tympanic membrane perforation, was first described by Wullstein in 1952 and Zollner in 1955. 1 The aim of myringoplasty is to eradicate middle ear disease and improve hearing by closing the perforation in the ear membrane. Although temporal muscle fascia (TMF) is the most commonly used graft material, the use of cartilage graft has evoked considerable interest in the last decade. 2 The first cartilage myringoplasty was performed by Salen in 1963. 3 During the last 20 years, various types and methods of cartilage myringoplasty have been presented. 4 In 2008, Tos classified the known 23 cartilage myringoplasty techniques into 6 main groups. 5 Our technique was classified in the group of “special cartilage tympanoplasty techniques” named as “composite chondroperichondrial clip tympanoplasty.”
Transcanal cartilage myringoplasty is a simple, comfortable, and effective technique. Because no postauricular incision is required, no mastoid dressing and no tympanomeatal flap elevation is necessary, the hospitalization of the patient is lesser. The only question of cartilage myringoplasty is its effect on hearing outcomes because of thickness. Hearing outcomes of different cartilage myringoplasty techniques were studied in the literature. 6–7 In this report, we aimed to present our experience in composite cartilage-perichondrium grafting technique by comparing to TMF myringoplasty in terms of anatomical and functional outcomes.
Materials and Methods
In this retrospective study, the medical records of patients who underwent type 1 myringoplasty by the same surgical team between September 2015 and February 2018 at Otorhinolaryngology Department of Erzurum Ataturk University were reviewed. Demographic properties, preoperative otological findings, preoperative pure ton audiogram findings, postoperative pure ton audiogram findings, and duration of surgeries were reviewed from medical records. The follow-up period was also reviewed from medical records. Postoperative air–bone gap (ABG) was calculated from the pure tone audiogram performed at postoperative first month. Acceptance of the graft was determined as the closure of the tympanic membrane at the otological examination performed at postoperative third month. The patients with lack of one or more of these information at medical records or lost for at least 3 months of follow-up were excluded from the study. Also patients whose medical records demonstrated a presentation with wet ear, history of a previous otological surgery, and presence of cholesteatoma or ossicular chain erosion were excluded from the study.
According to the graft material used in the operation, the patients were divided into 2 groups. The patients operated with transcanal composite chondroperichondrial cartilage graft myringoplasty (TCM) technique was regarded as the first group, while patients operated with temporal fascia was regarded as the second group (TMF). Both groups were compared according to preoperative and postoperative ABG, graft acceptance rate, and duration of operation.
Temporal muscle fascia myringoplasty was performed as previously described by Rizer. 8 Our surgical technique for TCM is as follows: Once the surgical field had been sterilized, 2 and 4 mL of local anesthetic were administered at the meatal and lateral face of the tragus and 4 quadrants of the outer ear canal. An ear speculum was inserted into the outer ear canal, and the perforation margins were de-epithelized with a straight pick. An incision was then made over the meatal surface of the tragal skin. Tragal cartilage was taken together with the lateral perichondrium. The lateral perichondrium was 1 mm larger than the tragal cartilage. The tragal cartilage was then thinned to 0.5 mm using a scalpel. The middle ear was filled with spongostan through the tympanic perforation. The cartilage graft was placed into the tympanic perforation without elevation of tympanomeatal flap. The perichondrium was overlaid to the tympanic membrane so as to remain in a lateral position to the membrane residue (Figure 1). The operation was completed by supporting the lateral aspect of the cartilage graft with spongostan.
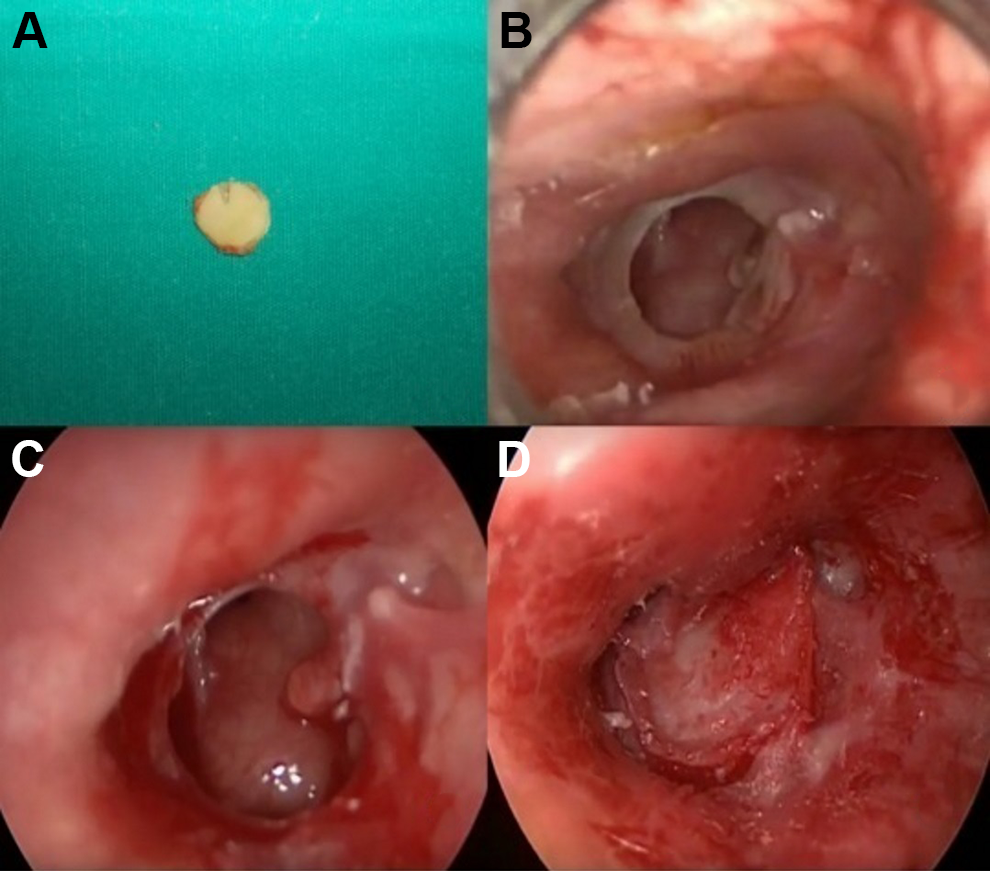
Appearance of cartilage (A), tympanic membrane perforation (B), and de-epithelialization of perforation margins (C). Graft is placed into perforation (D).
Statistical analysis was performed using SPSS version 20.0 software (SPSS Inc, Chicago, Illinois). The independent samples test was used to examine the relationship of continuous variables such as duration of surgery and mean ABGs. The χ2 test was used to assess the relationship between categorical variables such as demographic data and acceptance rates. A P value <.05 was considered indicative of a statistically significant difference.
Power Analysis
As we expected a similar postoperative ABG in both groups, the primary outcome of the study was the difference in operation times. In our preliminary study, the standard deviation of operation time was 6.0 in the TMF group and 3.0 in the TCM group. The expected difference in the operation time was at least 20 minutes. Accordingly, with 50 patients in both groups, the power of the study was calculated as 100%, with α error of .05 using Russ Lenth Piface Java Module.
Results
A total of 113 patients whose medical records met the inclusion criteria were included in the study. Of these, 59 patients underwent TCM and 54 underwent TMF myringoplasty. Forty-six of the 59 ears treated by TCM were operated under local anesthesia and 13 (22%) under general anesthesia. All 54 patients treated with TMF were operated under general anesthesia.
Of 59 patients who underwent TCM, 35 were women and 24 were men (mean age: 29.1 ± 8.2 years). Of 54 patients who underwent TMF, 30 were women and 24 were men (mean age: 31.9 ± 10 years). The mean duration of follow-up was 9 months (range: 7-21 months). There was no significant difference between groups with respect to demographic characteristics. The demographic properties of patients are summarized in Table 1.
Demographic Properties of Patients.
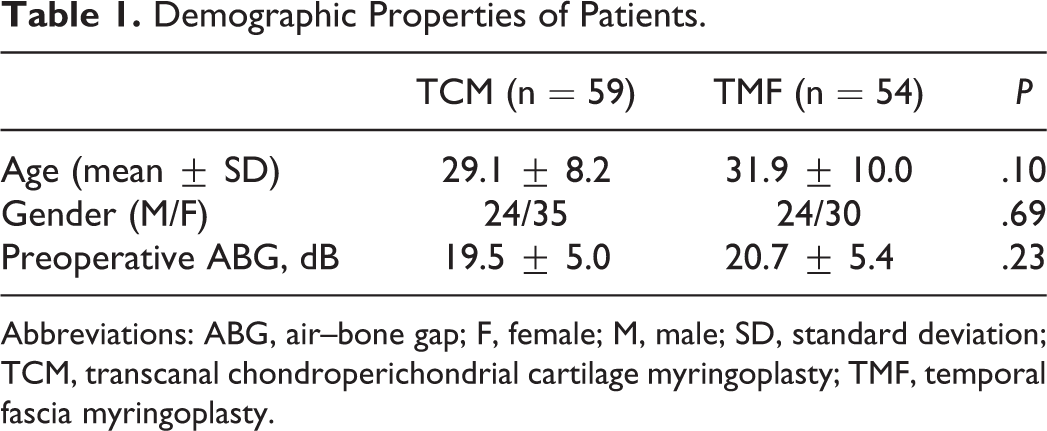
Abbreviations: ABG, air–bone gap; F, female; M, male; SD, standard deviation; TCM, transcanal chondroperichondrial cartilage myringoplasty; TMF, temporal fascia myringoplasty.
Tympanic membrane perforation closure success rate in the cartilage group was higher than those in the fascia group (91.0% vs 83.3%; P = .046). Comparison of pre- and postoperative audiometry revealed a significant improvement in ABG in both groups, with no significant difference between groups. In the cartilage group, preoperative ABG was 19.5 ± 5 dB and postoperative ABG was 10.8 ± 4.8 dB. In the fascia group, the corresponding values were 20.7 ± 5.4 and 11.5 ± 5.4 dB, respectively (P < .05). The mean duration of surgery was 29.5 ± 3.4 minutes in the TCM group and 61.5 ± 6.0 minutes in the TMF group. Durations of surgery were significantly shorter in the TCM group (Table 2).
Comparison of Outcome Measurements in Both Groups.
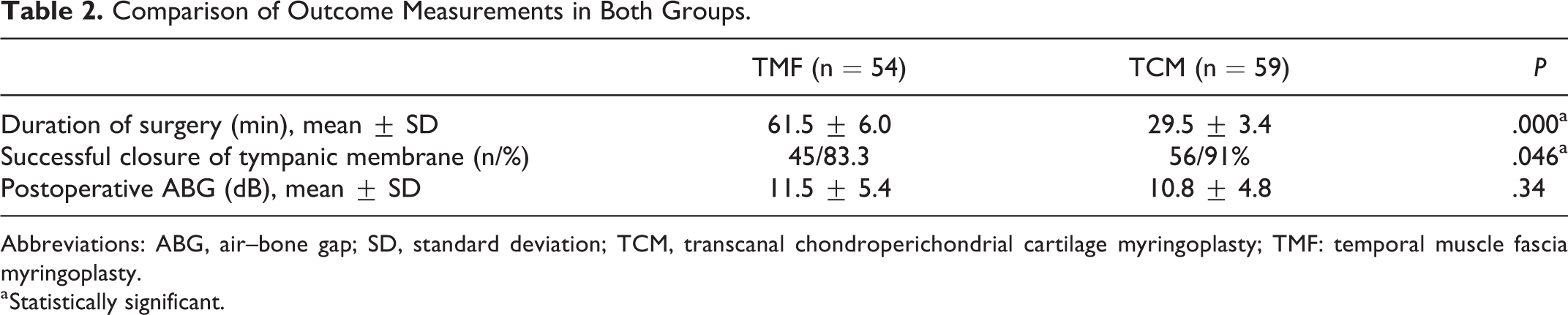
Abbreviations: ABG, air–bone gap; SD, standard deviation; TCM, transcanal chondroperichondrial cartilage myringoplasty; TMF: temporal muscle fascia myringoplasty.
a Statistically significant.
Discussion
The results of this study suggested several advantages of TCM technique over myringoplasty with TMF. Graft acceptance success was higher and the duration of surgery was shorter in the TCM group. Both surgical techniques had similar outcomes in terms of changes in ABG.
Myringoplasty, which is aimed to establish a dry middle ear cavity and restoration of hearing, is one of the most common otological procedure. Although fascia of temporal muscle is still the most common graft material used for myringoplasty, cartilage is being popular in recent years. Cartilage can be harvested near the surgical field and is more resistant to infection, lack of vascularization, and resorption. 9 These properties made it more useful for difficult cases, such as Eustachian tube dysfunction, negative pressure in the middle ear, retraction pocket, and revision cases. There are several techniques reported in the literature for cartilage myringoplasty including the cartilage-perichondrium composite graft, butterfly techniques, palisade cartilage tympanoplasty, and diced cartilage. 4 We used the cartilage-perichondrium graft technique in this study to maximize the graft acceptance rate by preventing the risk of mobilization of the graft.
One of the main disadvantage of using cartilage as a graft material is the thickness. Tympanic membrane is 0.1 mm thick and the graft material should be similar to that thickness for better audiological results. Aslıer et al reported that cartilage myringoplasty has a negative effect on acoustic transfer performance and they recommend cartilage reduction to 400 µm instead of using full thickness graft to yield better transfer performance. 10 We used a partial thickness graft in this study.
There are several studies in the literature comparing the clinical outcomes of cartilage and fascia myringoplasty techniques. In the meta-analysis conducted by Jeffery et al, the palisade cartilage tympanoplasty was found to have an overall 96% success rate with similar ABG closure level to temporalis fascia tympanoplasty. 4 Mohanty et al compared the clinical outcomes of endoscopic cartilage versus temporalis fascia grafting in anterior quadrant perforations and they reported an overall success rate as 91.9% in cartilage and 79% in fascia groups. The changes in ABG were similar in both groups. After 1-year follow-up, they observed medialization in 5 patients in the fascia group but no patients in the cartilage group had medialization or lateralization. They suggested cartilage-perichondrium technique as an effective technique for anterior quadrant perforations. 9 Balci et al compared the hearing outcomes of cartilage and fascia graft techniques in patients with normal preoperative hearing levels and they reported a similar ABG closure levels, word recognition score, and pure tone audiogram increase. They also reported a higher graft acceptance rate in cartilage group. 11 Ciğer et al compared these 2 graft materials in their prospective, randomized study and they found similar hearing outcomes in both techniques. Graft success rate at the first year was 85.1% in the fascia group and 97.7% in the cartilage group and this difference was statistically significant. 12
In a study performed by Jain et al, the graft take-up rate was 97.1% in the cartilage group and 82.9% in the fascia group with similar hearing outcomes. Also they reported 2 patients in the fascia group had retraction in their follow-up period but no patient in the cartilage group had retraction. 13 Guler et al compared the temporal fascia and cartilage graft techniques in elderly patients and reported a higher graft acceptance rate in the cartilage group, but they reported that mean hearing gain was significantly higher in the fascia group. 14 Baklaci et al reported a better graft acceptance rate in cartilage tympanoplasty in pediatric patients. 15 In a recent meta-analysis, Jalali et al reviewed a total of 37 studies and they reported that cartilage grafting had a higher graft acceptance rate compared to fascia grafting. They also suggested that the hearing outcomes of cartilage and fascia grafting techniques were similar. 16
Some of the key disadvantages of TMF myringoplasty include use of postauricular incision, canal incision, elevation of tympanomeatal flap, greater postoperative pain, requirement for mastoid dressing, and longer duration of hospitalization. Use of a transcanal cartilage graft does not require postauricular and canal incision or mastoid dressing; there is less postoperative pain and the hospitalization time is shorter. 6 In the study of Mauri et al, the mean duration of cartilage myringoplasty was 33.6 ± 7.8 minutes, compared to 62.9 ± 12.7 minutes for TMF. 17 In our study, the length of surgery was 29.5 ± 3.4 minutes in the TCM group and 61.5 ± 6.0 minutes in the TMF group.
Our study has some limitations which have to be pointed out. First, this was a retrospective study and the data of patients obtained from medical records may be inaccurate. Second, the follow-up was limited. Third, the perforation size of the tympanic membrane of the patients was variable. New prospective studies with larger populations and long-term follow-up are needed.
Conclusion
Transcanal cartilage chondroperichondrial cartilage myringoplasty may be the first choice of surgical technique to its higher success rates, shorter operation time, and functional outcomes similar to those of temporalis fascia myringoplasty.
Footnotes
Authors’ Note
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was approved by Ethical Committee of Ataturk University, Faculty of Medicine with approval number 2019;04:51.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.