
Abstract
Background:
Surgical repair of septal perforations has been historically cumbersome. Recently described techniques utilizing interposition grafting with polydioxanone (PDS) plates wrapped in a temporoparietal fascia (TPF) graft have reported successful closure in 90% to 100% of cases. Our objective is to expand the investigation into the use of interposition grafts of polydioxanone plates combined with a temporoparietal fascia graft for nasal septal perforation repair.
Methods:
Retrospective review of the medical record was performed for all septal perforation repairs using the TPF-PDS plate interposition graft technique from August 1, 2017 to March 1, 2021 at the University of Iowa. Minimum post-operative follow-up was 1 month.
Results:
Our series included 31 patients with symptomatic nasal septal perforations. Thirteen patients underwent open while 18 patients underwent endonasal graft placement. The mean perforation size was 1.49 cm2. The mean post-operative follow-up was 11.5 months.
Conclusions:
Repair of symptomatic nasal septal perforations using an interposition graft of polydioxanone plate wrapped in temporoparietal fascia demonstrated an overall success rate of 90%.
Introduction
Septal perforations are a frustrating entity for both clinicians and patients. Nasal septal perforations are full-thickness, often anterior, defects in the nasal septum. The resulting aberrant connection between the right and left nasal cavities causes turbulent airflow in the nasal airway. Consequentially, patients experience a variety of troubling symptoms including whistling, epistaxis, crusting, pain, nasal obstruction, rhinorrhea, rhinosinusitis, dysosmia, and in severe cases, saddle nose deformity. 1 Reported etiologies of nasal septal perforations are numerous, and include: trauma, autoimmune diseases, infection, neoplasms, iatrogenic (incidence of perforation after septoplasty ranging from 0.5% to 3.1% 2 ), and intranasal drug use. Management of septal perforations ranges from medical optimization with humidification or emollients to prosthetic septal replacement 3 (ie, septal button) to surgical repair, with treatment goals aimed predominantly at symptom resolution as opposed to reconstitution of the native septum.
Surgical repair of septal perforations has been historically cumbersome. Between challenging surgical conditions and hostile healing environments, operative results have been fraught with variable success rates ranging from 30% to 100%. 4 Numerous techniques have been designed to repair nasal septal perforation—bilateral mucoperichondrial flap repair with interposition graft, 5 staged inferior turbinate flap, 6 acelluar dermis interposition graft, 7 auricular cartilage interposition, 8 facial artery myomucosal (FAMM) flap, 9 and interposition grafting with synthetic4,10,11 and autologous grafts. 12 In addition to operative technique, other contributing factors to successful closure and symptom resolution include the etiology of the septal perforation and the diameter, with perforations greater than 20 mm displaying higher failure rates.
Recently described techniques utilizing interposition grafting with polydioxanone (PDS) plates wrapped in a temporoparietal fascia (TPF) graft have reported successful closure in 90%10,11 to 100% 4 of cases. In addition to a relatively high success rate, the technique sports the advantage of not requiring utilization of surrounding mucosal advancement/rotational flaps to aid in repair. The PDS-TPF interposition graft instead serves as a mesenchymal scaffold that promotes both revascularization and mucosalization. Therefore, we aim to demonstrate that in addition to an open approach, endonasal septal perforation repair using the PDS-TPF interposition graft is an efficient utilization of a surgical technique familiar to the general otolaryngologist and plastic surgeon. We additionally intend to corroborate previously published data supporting the success of this technique,10,11 and add further insight into nuances that may contribute to success or failure rates. Outcomes of both open and endonasal approaches performed at our institution will be reported, as well as, concurrent nasal airway procedures performed at the time of surgical septal perforation repair.
Methods
Study Design
A retrospective review of medical records was performed for all septal perforation repairs performed by a single surgeon at the University of Iowa using the PDS-TPF interposition graft technique from August 1, 2017 to March 1, 2021. These dates were inclusive of all patients, regardless of open or endonasal approaches, with no exclusion criteria utilized. The study was approved by the University of Iowa institutional review board and patient consent was waived as all data was deidentified and collected retrospectively. The primary outcome was the successful closure of the septal perforation with a secondary outcome being symptom resolution. Minimum post-operative follow-up time was 1 month with mean follow-up being 11.5 months. Initially, all patients underwent an open approach but as the sample size increased, the senior author began to perform the procedure via an endonasal, hemi transfixion incision reserving the open approach for patients who required more complex concurrent vestibular stenosis repair.
Surgical Technique
Circumferential external nasal anesthesia blocks are performed with local anesthesia containing epinephrine. The bilateral nasal cavities are examined with a 0° rigid endoscope and the dimensions of the perforation measured in both anterior-posterior and cranio-caudal dimensions. For the endonasal approach, a hemitransfixion incision is made at the caudal end of the quadrangular cartilage. Submucoperichondrial flaps are elevated around the septal perforation and deviated septal cartilage and bone are removed or repaired. Dissection extends from the perpendicular plate of the ethmoid bone posteriorly to the floor of the nose inferiorly. A 0.15 mm thick, porous PDS plate is then fashioned to allow 5 mm overlap of the perforation on at least 3 sides.
In the open approach, an inverted-V incision is made across the waist of the columella in addition to marginal incisions along the border of the lower lateral cartilages. After a sub-SMAS dissection, the septum is approached via a split-cartilage approach (Figure 1).
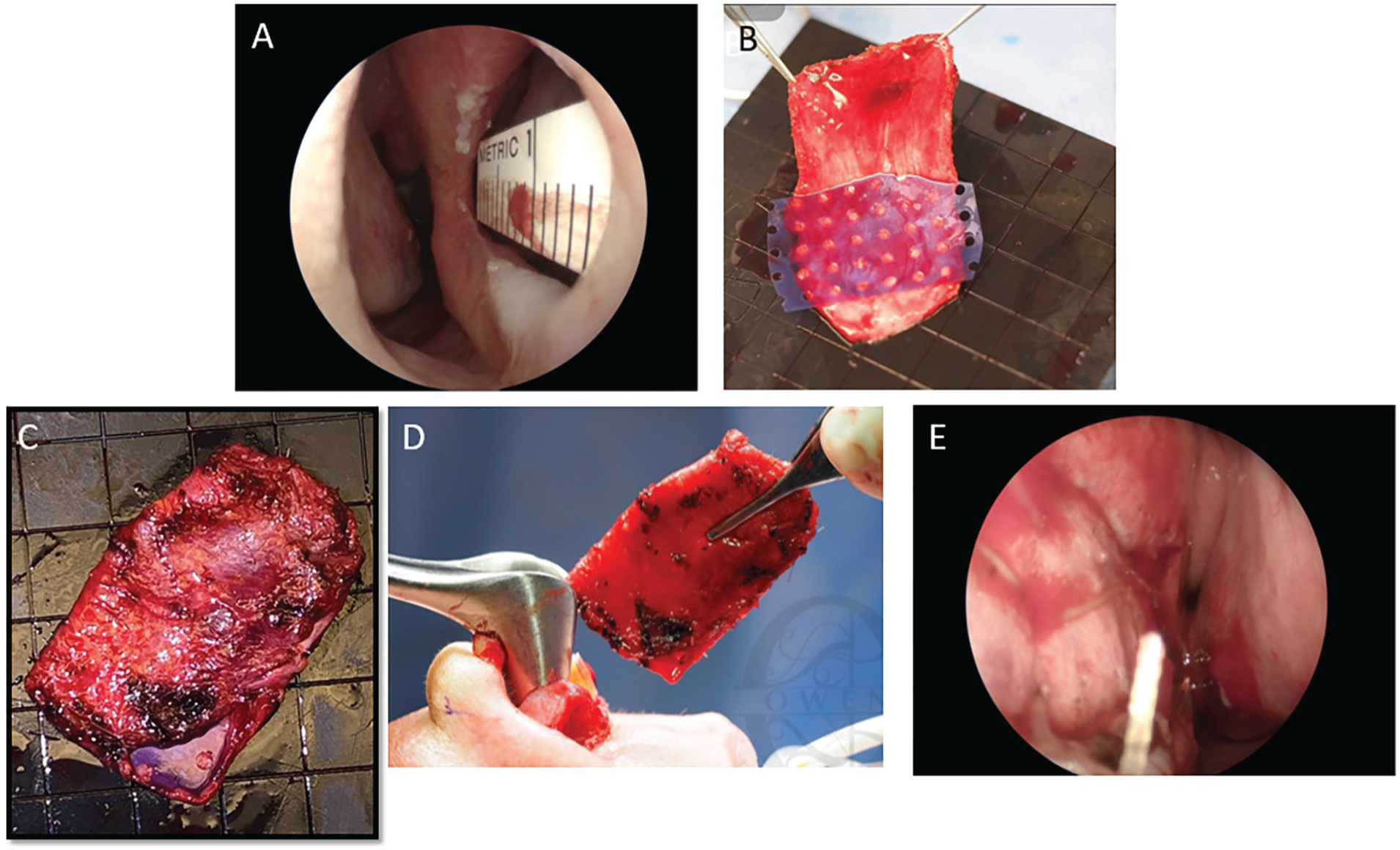
Temporoparietal fascia (TPF) graft design and placement. Intraoperative Measurement of Septal Perforation in the anterior-posterior (A) dimension. Harvested TPF graft (B) wrapped around 0.15 mm PDS plate and secured with Monocryl (C). Placement of the interposition graft from an open approach (D) and intraoperative view of secured graft with quilting stitch after endonasal placement (E).
Harvest of Temporoparietal Fascia Graft and Coverage of PDS Plate
A 4 cm incision is planned in the left temporalis region of the scalp superior to the left auricle. A beveled incision is made to protect the hair follicles. Using a 15-blade scalpel, the incision is deepened to the level of the temporoparietal fascia. 13 Monopolar cautery is used to dissect the temporoparietal fascia from the overlying subcutaneous tissue. A portion of TPF is then harvested to ensure a snug, 360° envelope around the PDS plate, with care taken to avoid excessive tension and subsequent warping of the construct. The free ends of the TPF envelope are sutured using 4-0 Monocryl and approximately 5 full-thickness U-stitches are dispersed centrally throughout the construct to ensure close adherence of the TPF to the underlying PDS plate. The PDS-TPF graft is inserted under the submucoperichondrial flaps, directly over the septal perforation and sutured in place with a quilting 5-0 Chromic gut, again ensuring 5 mm overlap of the perforation on at least 3 sides. If endonasal, the hemitransfixion incision is closed with 5-0 Chromic. If open, the transcolumellar and marginal incisions are closed with 6-0 fast absorbing plain gut. The septal flaps are then secured to the graft using 4-0 plain gut suture on a straight SC-1 needle via a mattress stitch. The repair is reinforced with 0.04 inch silastic splints and Doyle splints placed in bilateral nasal cavities and secured to the anterior membranous septum with a 3-0 nylon suture. The Doyle splints are removed 7 to 10 days post-operatively and the silastic sheeting removed 5 to 6 weeks post-operatively.
Results
Patient Characteristics
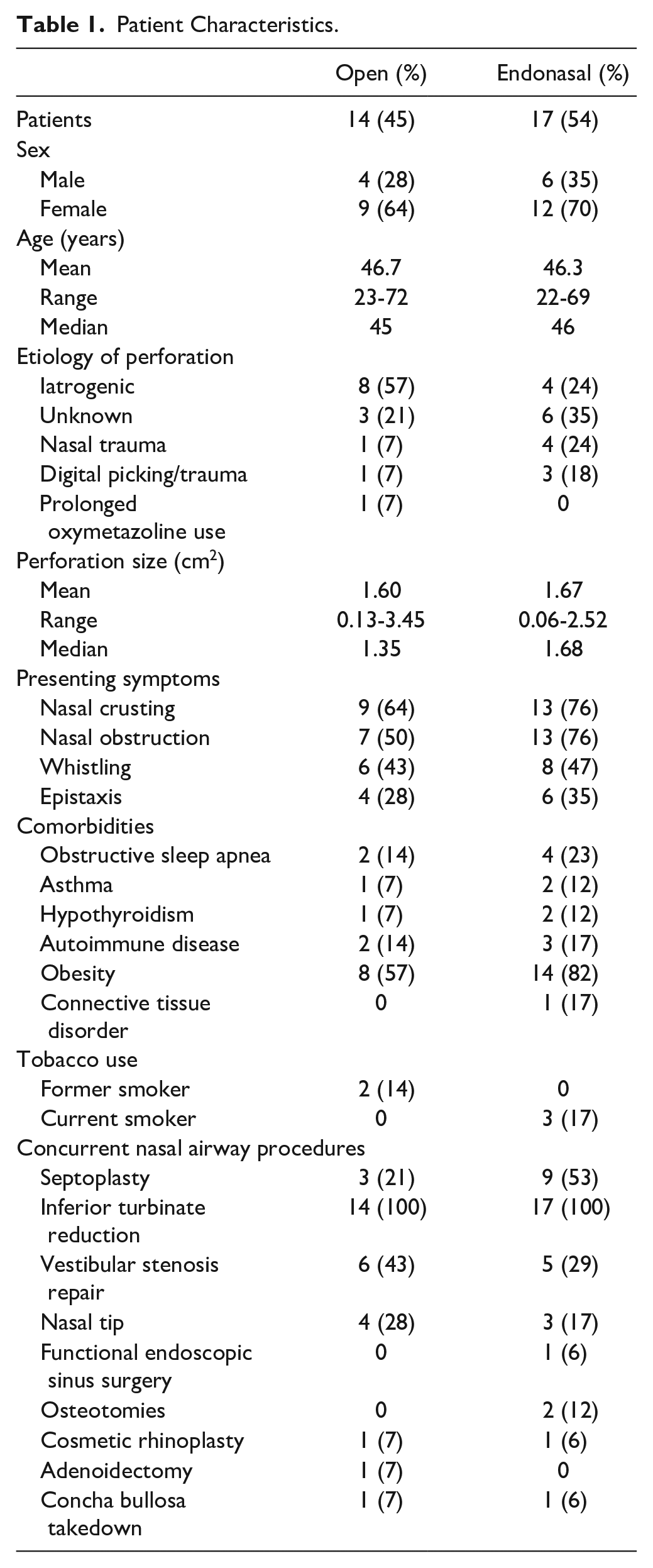
Our series included 31 patients (21 women (67%), 10 men (33%); mean age 47.8 years). The etiology of the nasal septal perforations included iatrogenic (12 [35%]), unknown (9 [29%]), nasal trauma (5 [16%]), digital trauma/picking (4 [13%]), and prolonged oxymetazoline use (1 [3%]). Patients presented most commonly with nasal crusting (22 [71%]), nasal obstruction (20 [64%], whistling (14 [45%]), and epistaxis (10 [32%]). The mean perforation size was 1.49 cm2. Two patients were former smokers (6%) and 3 patients (9%) were actively smoking at the time of surgical repair. Patient comorbidities included obstructive sleep apnea (6 [19%]), asthma (3 [9%]), hypothyroidism (3 [9%]), autoimmune disease (5 [16%]), obesity (19 [61%]), morbid obesity (2 [6%]), and 1 patient with Ehlers-Danlos Syndrome (3%). Additionally, another patient was being actively treated with bevacizumab for treatment of stage IV colon cancer at the time of repair (1 [3%]) (Table 1).
Patient Characteristics.
Surgical Outcomes
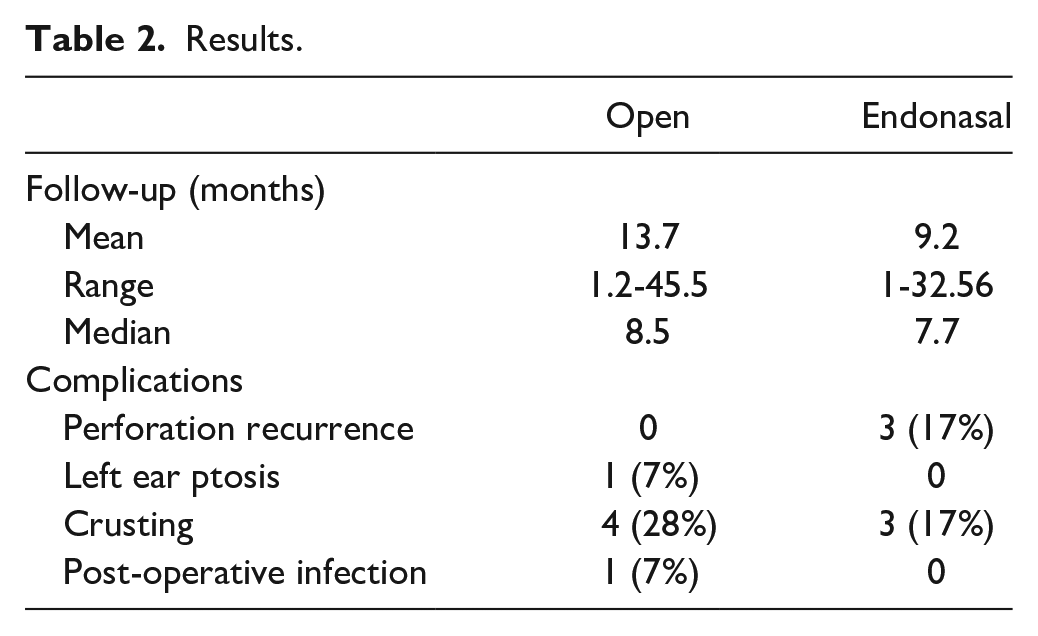
In our case series, 14 patients (45%) underwent open septoplasty approach for surgical correction of septal perforation and 17 (54%) underwent an endonasal approach. The mean post-operative follow-up was 11.5 months. Overall, our results demonstrated a 90% (28/31) success rate in septal perforation closure using the TPF-PDS interposition graft. All patients who underwent open procedures had complete resolution of their perforation with mucosalization of the graft at their most recent follow-up. Of the patients who underwent endonasal approach, 3 (17%) developed graft failure causing plate exposure and extrusion with recurrence of the septal perforation.
The most common complication of this technique was graft crusting, which was observed in 7 patients (22%) post-operatively—3 patients had resolution of crusting with evidence of mucosalization after replacement of silastic splints for an additional 6 to 8 weeks while 4 patients mucosalized after treatment with nasal emollients and humidification. No patients required revision nasal surgery; however, 1 patient developed a left ear ptosis as a complication of the left scalp TPF graft harvest site and required surgical revision 6 months post-operatively. A single patient underwent repair of an oronasal fistula, costal cartilage harvest and secondary cleft rhinoplasty at the time of septal perforation repair. They subsequently developed a post-operative surgical site infection that required a peripherally inserted central catheter (PICC) and intravenous antibiotics. Overall, 16 patients (51%) experienced no post-operative complications and had resolution of symptoms (Table 2).
Results.
Discussion
In this retrospective study, we were able to substantiate the results of Flavill and Gilmore, 14 Epprhect et al, 10 and Morse et al. 11 Similar to Epprecht et al, 10 we demonstrated that endonasal insertion of the PDS-TPF interposition graft via a technically familiar endonasal surgical approach yields similarly favorable outcomes to the open, transcolumellar approach. In our series, 28 of 31 nasal septal perforations (90%) were resolved, which is similar to the reported outcomes of other interposition grafting techniques described in the literature.14-17
In addition to placement of the PDS-TPF graft, every patient in this case series underwent additional, concurrent nasal airway procedures at the time of surgery. In our series, nasal obstruction was the second most commonly reported pre-operative symptom (22/31 [64%]). Nasal obstruction can be the result of anatomic, physiologic, and pathophysiologic factors and is often multifactorial. 18 While nasal septal perforations are known pathophysiologic contributors to nasal obstruction, additional anatomic etiologies may also be present and, when identified, should be surgically corrected at the time of perforation repair. A submucous inferior turbinate reduction and outfracture was performed on all patients to improve airway symptoms19-24 and compensate for the slightly larger septal width once our TPF-PDS construct was placed. Furthermore, we did not observe any additional adverse outcomes as the result of concomitant turbinoplasty (eg, hemorrhage and synechia 19 ).
We should note that our experience with this technique evolved over time as our sample size increased. Initially, we performed an open approach, which had the notable advantages of enhanced exposure and easy access to the structures involved in repair of vestibular stenosis. However, post-operative soft tissue edema and prolonged operative time make this approach less desirable. Furthermore, generalists must become proficient with the transcolumellar approach to utilize this technique. Because of this, we transitioned to an endonasal approach as had previously been reported by Epprecht et al. 10 Additionally, we found that the endonasal approach did not limit our ability to correct vestibular stenosis, when indicated.
All 3 patients in our case series who developed graft failure and perforation recurrence had undergone an endonasal approach. The hemitransfixion incision has become a standard endonasal approach to the caudal end of the nasal septum, anterior maxillary spine, crests of the maxilla, and floor of the nose since it was first described by Williams in 1967. One of the advantages of the hemitransfixion incision listed in the original publication is its ability to preserve the blood supply to the septum by accurately elevating the mucoperichondrium, from which the avascular septal cartilage derives its nutrients. 25 Kiesselbach’s plexus on the anterior nasal septum is supplied by the posterior septal artery, along with the greater palatine artery and septal branches of the superior labial and anterior ethmoidal arteries. 26 Though Morse et al. 11 hypothesized the hemitransfixion or Kilian incision inherently risked truncating this anterior blood supply to the ipsilateral mucoperichondrial flap, we do not believe this to be the primary factor resulting in failure in this cohort. Instead, 2 of the 3 patients reported picking at their grafts and/or removal of their splints prematurely and 1 patient began use of nasal irrigations immediately post-operatively likely causing sheering forces on the graft. Disruption of the 6 week splinting period was a common theme in graft failure, suggesting this protection of the graft was important in epithelialization. Persistent smoking was also observed in at least 1 failure. We believe these factors to be relevant in the fate of the TPF-PDS constructs, ultimately resulting in their failure and extrusion. Additionally, the 83% success rate of the endonasal approach remains within the upper range of the 30% to 100% reported success rates of previously described septal perforation repair procedures. 4 Therefore, we feel the endonasal approach for placement of the TPF-PDS graft remains a promising and viable technique for resolution of septal perforations.
Limitations
Our retrospective case series corroborates the previously reported high success rate of this surgical technique to close nasal septal perforations from both the endonasal and open approaches.4,10,11 However, we acknowledge several limitations to our study. First, this is a retrospective evaluation with a small sample size and short follow-up which limits the power of our results. Additionally, the mean perforation size was 1.49 cm2 with only 4 patients having perforations ≥2 cm in greatest diameter and 2 patients missing preoperative documentation of their perforation dimensions. Additional, longer-term follow-up and objective measurement of patient symptoms with a validated patient reported outcome measurement tool perioperatively would also add meaningful information for clinical outcomes as a result of this procedure.
Conclusions
Interposition grafts composed of polydioxanone plates wrapped in free temporoparietal fascia to repair symptomatic nasal septal perforations are associated with positive outcomes. The open transcolumellar and endonasal hemitransfixion approaches are effective options for graft placement, with high success rates of 100% and 83%, respectively. Concomitant surgical procedures to address nasal airway obstruction can be safely executed at the time of septal perforation repair utilizing either approach. While the temporoparietal fascia graft has proven to be an effective scaffold for respiratory epithelial mucosalization, histopathologic studies are needed to determine the cellular architecture and microenvironment of the graft after complete incorporation/uptake.
Footnotes
Author Contributions
Drs. Rossi Meyer, Abthai, and Owen had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.