
Abstract
Cervical vagus nerve is not identified by computed tomography or magnetic resonance imaging. Transcutaneous sonography may be the best imaging study to evaluate the cervical vagus nerve. A 7 to 18 MHz linear array transducer was placed transversely on the lateral neck focusing on the carotid sheath from the clavicle level upward to the digastric muscle level bilaterally. The gray-scale technique was used, with the scan setting for the thyroid gland. Between January 2015 and March 2016, 314 patients with 628 cervical vagus nerves were enrolled, including 104 men and 210 women. Their ages ranged from 14 to 84 years. Transcutaneous sonography identified the entire trunk of bilateral cervical vagus nerves in 254 (80.9%) patients and did not identify 1 or both cervical vagus nerves in the other 60 (19.1%) patients. Among 628 cervical vagus nerves, transcutaneous sonography identified 626 (99.6%) lower cervical vagus nerves and 551 (87.7%) upper cervical vagus nerves. Among 551 visible upper cervical vagus nerves, 495 (89.8%) nerves were located laterally, 17 (3%) nerves were located medially, 9 (1.6%) nerves were located anteriorly, and 30 (5.4%) nerves were located posterior to the internal carotid artery. Man and left-side nerve were the factors associated with the anatomical variation in the upper cervical vagus nerve. Transcutaneous sonography can be the best imaging study to show the cervical vagus nerve and may be helpful to evaluate the nerve before neck operation.
Introduction
The vagus nerve is the longest cranial nerve and originates from the brain stem through the jugular foramen into the carotid sheath between the carotid artery and the internal jugular vein in the neck and then to the chest and abdomen. The vagus nerve supplies a lot of important functions to the pharynx, larynx, and internal organs in the thorax and abdomen. 1
For some clinical reasons, it is necessary to evaluate the integrity or the lesion of the vagus nerve in the neck, for example, vocal fold paralysis or vagus nerve schwannoma. However, it is difficult to show the vagus nerve on the conventional X-ray, computed tomography (CT) scan, and magnetic resonance imaging (MRI). High-resolution transcutaneous sonography may be the best imaging method to show the cervical vagus nerve. 1 –3 Although previous studies have demonstrated sonoanatomy of the cervical vagus nerve, 2 –5 most of the studies did not evaluate the entire cervical vagus nerve along the carotid sheath between level II and level IV and the anatomical variation of the nerve.
In this article, we report that transcutaneous sonography can show the entire cervical vagus nerve between the upper neck and the clavicle level very clearly and describe the anatomical relationship between the cervical vagus nerve and the great vessels in the carotid sheath.
Patients and Methods
Patients who underwent head and neck sonography at the Department of Otolaryngology of the Hospital between January 2015 and March 2016 were enrolled in this study. The exclusion criteria included the patients younger than 10 years, with neck operation, or with untreated/treated head and neck cancer. The ultrasound machine (AplioXG SSA-790A; Toshiba, Medical Systems Co, Otawara, Japan; Hitachi Hivision Avius, Hitachi Aloka Medical, Tokyo, Japan) with a 7 to 18 MHz linear array transducer (PLT-1204BX for the Toshiba machine; EUP-L75 for the Hitachi machine) was used to evaluate the neck with the scan setting for the thyroid gland. All eligible patients lied in supine position with neck slightly extended. The author performed ultrasound examination for the patient with a regular protocol described in a previous article. 6 On examination, the scanner was placed on the lateral neck in a transverse way, focusing on the carotid sheath. The presence and location of the cervical vagus nerve were evaluated from the clavicle level upward to the level of the posterior belly of the digastric muscle bilaterally. The vagus nerve appears as a 1 to 3 mm, small round, relatively hypoechoic, sometimes honeycomb structure inside the carotid sheath. 1
The upper cervical vagus nerve was defined as the nerve superior to the carotid bifurcation (the level II), and the lower cervical vagus nerve was defined as the nerve inferior to the carotid bifurcation (the level III and level IV). The entire cervical vagus nerve identified on sonography was described in percentage of positivity. The anatomical relationship between the cervical vagus nerve and the carotid artery was also described. This study was reviewed and approved by the institutional review board at the National Taiwan University Hospital.
All statistical analyses were performed by SPSS software, version 17.0 (SPSS, Chicago, Illinois). The χ2 test and Student t test were used to determine differences between clinical parameters (ie, sex, age, the side of the neck, and anatomical variation). Corresponding P values ≤.05 were interpreted as statistically significant.
Results
Three hundred and fourteen patients were enrolled in this study, including 170 patients with thyroid nodules, 64 patients with neck mass, 29 patients with a salivary gland tumor, and 51 patients with other indications. The clinical data are shown in Table 1. They included 104 men and 210 women. Their ages ranged from 14 to 84 years, with a mean age of 52 years. Sonography showed the entire cervical vagus nerve in the both neck in 254 (80.9%) patients and did not show the nerve, either one or both sides, in the other 60 (19.1%) patients (Figure 1). Among 628 cervical vagus nerves evaluated, sonography showed 551 (87.7%) cervical vagus nerves from the lower to upper neck, 626 (99.6%) lower cervical vagus nerves, and only 551 (87.7%) upper cervical vagus nerves.
Demographic Characteristics of 314 Patients Receiving Sonography of the Cervical Vagus Nerve.
Abbreviations: F, female; M, male.
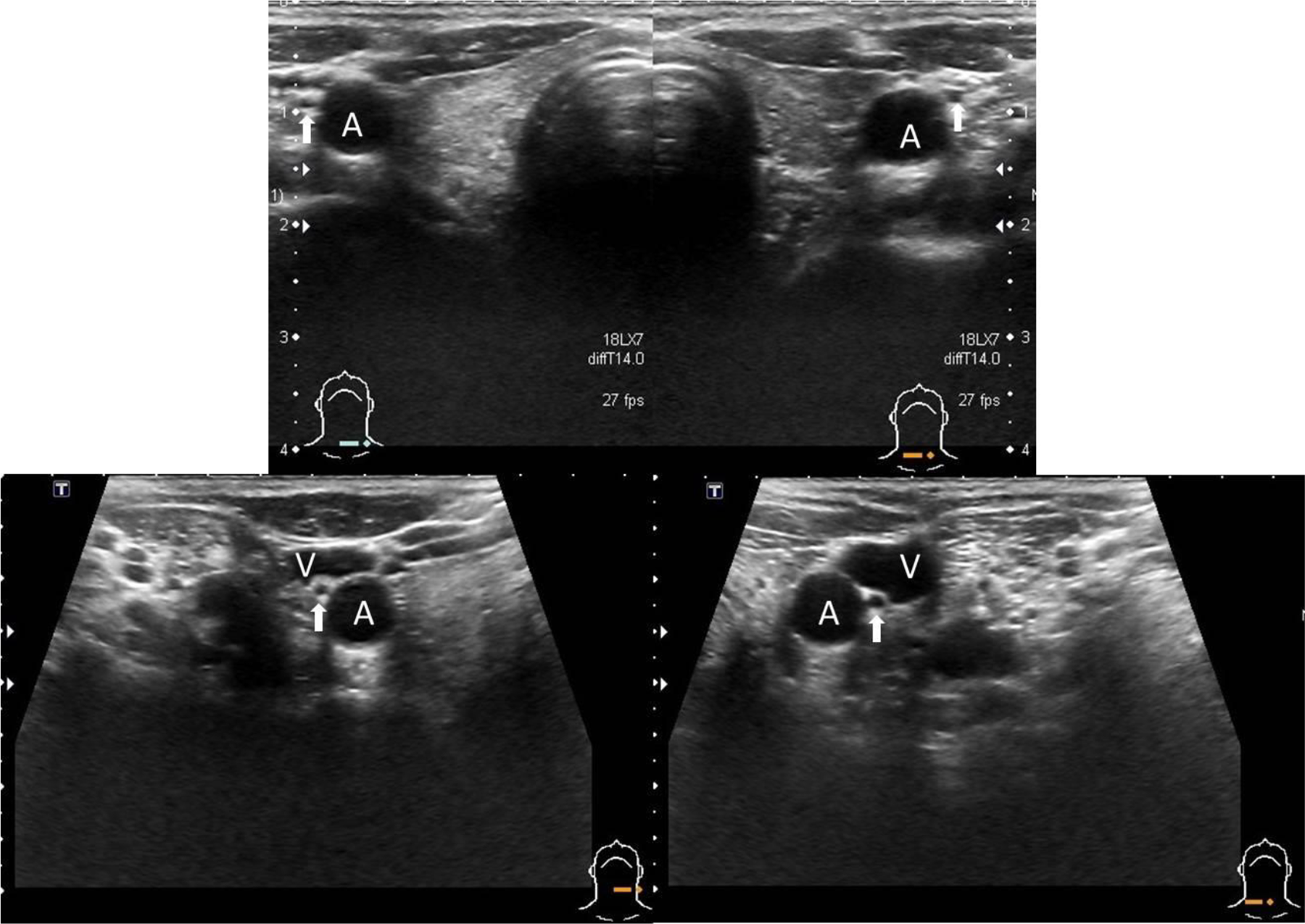
The anatomical relationship between the lower cervical vagus nerve and the common carotid artery. Vagus nerve (arrow). Common carotid artery (A). Internal jugular vein (V).
The clinical factors associated with invisible upper cervical vagus nerve on sonography are shown in Table 2. The age of the patient with visible upper cervical vagus nerves at both sides was similar to that of the patient with invisible upper cervical vagus nerves (mean 51.46 ± 14.46 years old vs 53.85 ± 12.5 years old, respectively, P = .23). The gender distribution between these 2 groups was similar (P = .969). Comparing right and left cervical vagus nerves, it was also similar between these 2 groups (P = .551).
Comparisons of Demographic Characteristics Between the Patients With Visible Upper Cervical Vagus Nerve at Both Sides of the Neck, and With Invisible Upper Cervical Vagus Nerve on Sonography.
In terms of the anatomical relationship between the upper cervical vagus nerve and the internal carotid artery (Figure 2; Table 3), among 551 visible upper cervical vagus nerves, 495 (89%) upper cervical vagus nerves were located lateral to the internal carotid artery, 17 (3%) nerves were located medially, 9 (1.6%) nerves were located anteriorly, and 30 (5.4%) nerves were located posteriorly. Man and left-side vagus nerve were the factors associated with the anatomical variation in the upper cervical vagus nerve (P = .012 and P = .02, respectively; Table 3). Age was not the factor associated with the anatomical variations of the upper cervical vagus nerve (P = .192).
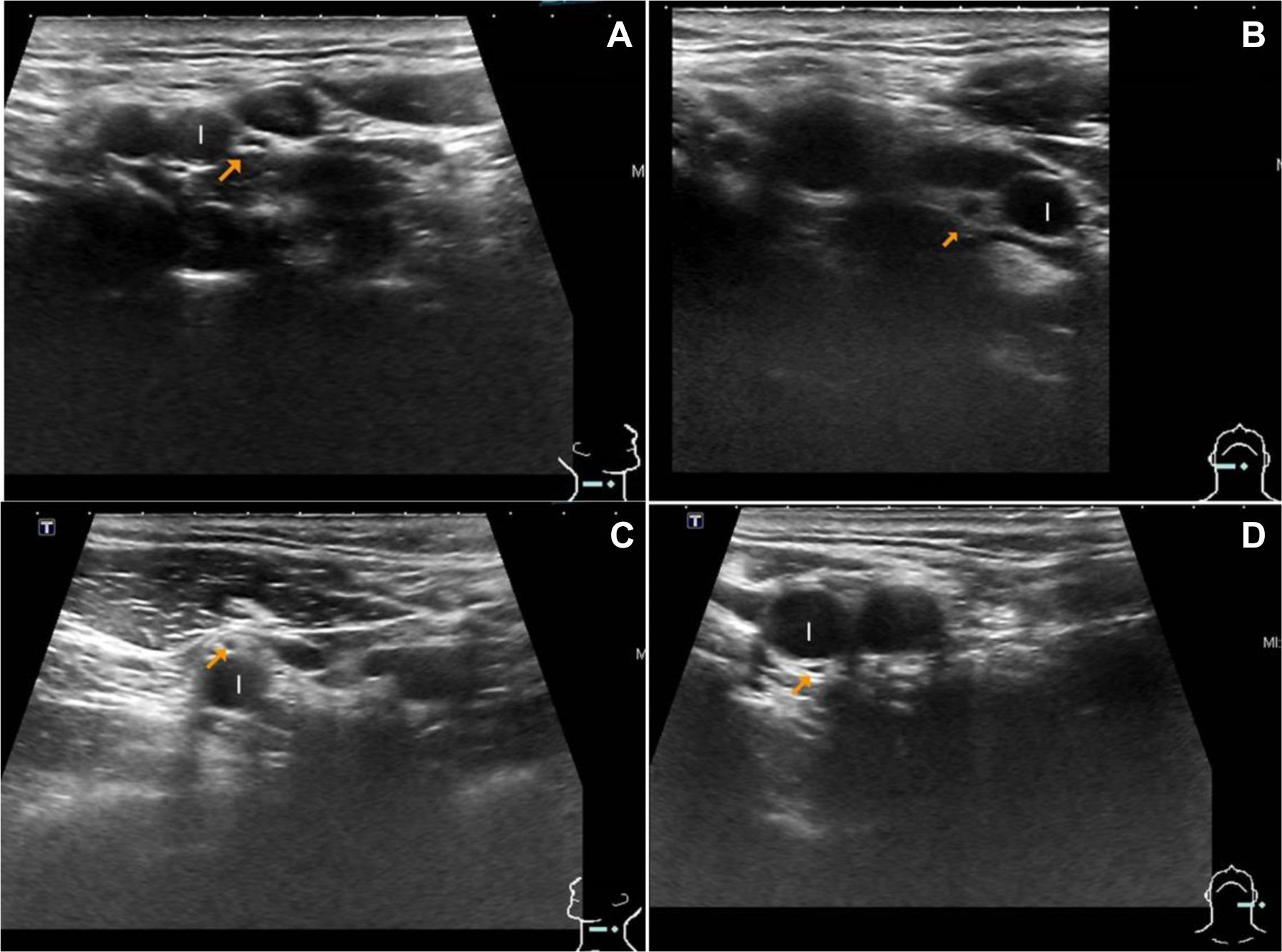
The anatomical variations between the upper cervical vagus nerve and the internal carotid artery. A, Lateral location. B, Medial location. C, Anterior location. D, Posterior location. Vagus nerve (arrow). Internal carotid artery (I).
The Anatomical Relationship Between the Invisible Upper Cervical Vagus Nerve and the Internal Carotid Artery.
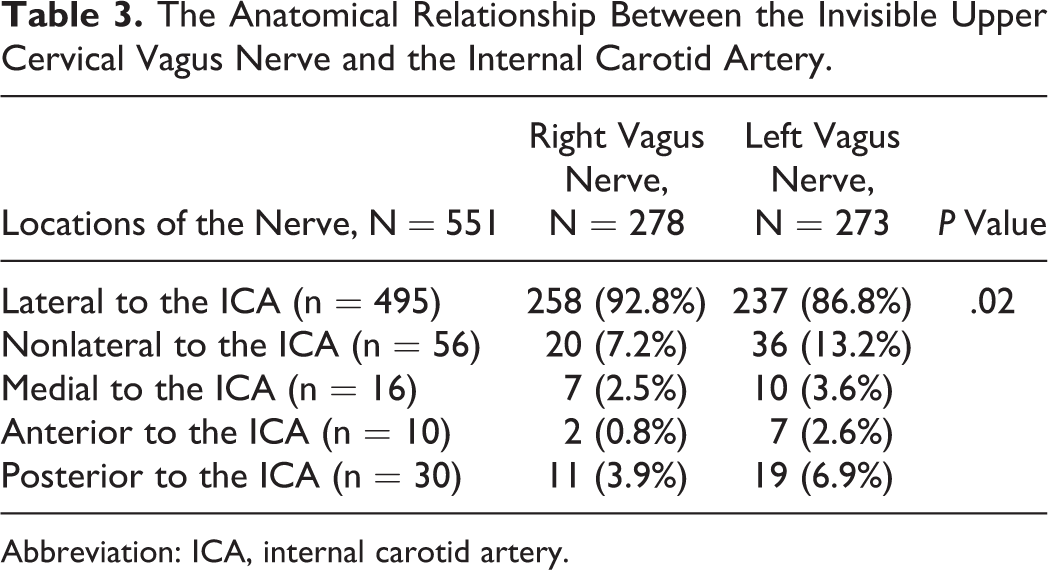
Abbreviation: ICA, internal carotid artery.
Discussion
In the head and neck regions, the vagus nerve involves many physiological functions of the larynx and pharynx including swallow and phonation. When the cervical vagus nerve is damaged, the patient has chocking, aspiration, dysphagia, and hoarseness. It is generally suggested to arrange CT scan or MRI from the skull base to the chest to evaluate the area around the recurrent laryngeal nerve and the vagus nerve when a patient has unilateral vocal fold paralysis without an apparent etiology. 7,8 However, it is difficult to use CT scan or MRI to diagnose thyroid cancer, which is one of the most common tumor causes. 9 Moreover, it is necessary to evaluate the cervical vagus nerve when there is no thyroid pathology, cervical esophageal cancer, or any other lesion in the tracheoesophageal groove, 8 but CT scan or MRI cannot show the vagus nerve. 1
From the previous studies, high-resolution sonography shows the cervical vagus nerve and also demonstrates the adjacent abnormal lesion involving the nerve. 1,2,4,5,10 However, no studies reported the application of transcutaneous sonography in identifying the entire cervical vagus nerve between the upper neck and the clavicle level. This is the first study to identify the entire cervical vagus nerve using transcutaneous sonography. This study showed that almost 100% of the lower cervical vagus nerves between the carotid bifurcation and the clavicle level were clearly identified on transcutaneous sonography. Transcutaneous sonography can identify 88% of the upper cervical vagus nerves because the level II of the neck is a little blurred on sonography, and the location of the upper cervical vagus nerve varies among people. Because none of other imaging studies can show the entire cervical vagus nerve, sonography is the best imaging study to evaluate the entire cervical vagus nerve. Nowadays, we suggest transcutaneous sonography as one of the imaging studies on the neck pathology with suspicious vagus nerve involvement. For example, when the patient has unilateral vocal fold paralysis without an apparent cause, we recommend sonography as the first-line imaging study to check the thyroid gland, cervical esophagus, tracheoesophageal groove, and cervical vagus nerve from the clavicle level to the upper neck. 7,8
Almost all lower cervical vagus nerves are located between the common carotid artery and the internal jugular vein. This is in accordance with previous studies, which showed only 0.7% and 5.5% of the lower cervical vagus nerves were medial to the common carotid artery 2.4,5 The medial variation in the lower cervical vagus nerve is located between the common carotid artery and the thyroid gland so that the nerve is potentially damaged when the thyroid gland is dissected laterally from the carotid sheath, especially when the thyroid tumor is big and the energy device is used. 2,3 It may be helpful to prevent vagus nerve injury during thyroid surgery if sonography indicates the location of the lower cervical vagus nerve in addition to the diagnosis of the thyroid nodule and the cervical lymph node metastasis although the medial variation is uncommon.
Regarding the anatomical variation in the upper cervical vagus nerve, the majority of the upper cervical vagus nerve is located lateral to the internal carotid artery. Lateral location of the upper cervical vagus nerve is potentially damaged when the lymphoareolar tissue is dissected from the internal carotid artery during neck dissection. Anterior location of the nerve is potentially divided when the internal jugular vein is ligated in level II during radical neck dissection. In terms of the diagnosis of the schwannoma or paraganglioma of the different nerve origins, sonography can distinguish schwannoma from other tumors and demonstrate the schwannoma of the vagus nerve or other nerves. Most of the upper cervical vagus nerve tumors are lateral to the internal carotid artery so that the tumor cannot separate the internal carotid artery from the external carotid artery (Lyre sign) and may not separate the internal carotid artery from internal jugular vein. 11 Only the tumor of the medial variation can splay the internal and external carotid arteries. This information of the nerve origin is very helpful before operation. 10
Conclusion
Transcutaneous sonography can be the best imaging study to show the cervical vagus nerve. This information may be helpful for differential diagnosis of the neck tumor of the nerve origin and prevention of vagus nerve injury during the operation.
Footnotes
Acknowledgments
The authors thank Division of Ultrasound, Department of Integrated Diagnostic & Therapeutics, National Taiwan University Hospital for support the ultrasound equipment during the study
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the National Science Council of the Republic of China (104-2314-B-002 -160 -MY3)” and in part by the National Taiwan University Hospital (NTUH.98- M1238).