
Abstract
Objective:
To investigate the value of diffusion tensor imaging (DTI) in the evaluation of vocal fold tissue microstructure after recurrent laryngeal nerve (RLN) injury.
Methods:
Six canines were divided into 2 groups: a unilateral vocal fold paralysis group (n = 4) and a control group (n = 2). The RLN was cut in the unilateral vocal fold paralysis group, and no intervention was applied in the control group. After 4 months, the canines’ larynges were removed and placed in a small animal magnetic resonance imaging (MRI) system (9.4T BioSpec MRI; Bruker, Germany). After scanning, the vocal folds were isolated, sectioned, and stained. The slides were then analyzed for the cross-sectional area and muscle fiber density through feature extraction technology. Pearson correlation analysis was performed on the DTI scan and histological section extraction results.
Results:
In the vocal fold muscle layer, the fractional anisotropy (FA) of the unilateral RLN injury group was higher than that of the control group, and the Tensor Trace was lower than that of the control group. This difference was statistically significant, P < .05. In the lamina propria, the FA of the unilateral RLN injury group was lower than that of the control group, P > .05, and the Tensor Trace was lower than that of the control group, P < .05. The muscle fiber cross-sectional area of the RLN injury group was significantly smaller than the control group with statistical significance, P < .05, and the density of muscle fibers was lower, P < .05. The correlation coefficient between FA and the cross-sectional area was −0.838, P = .002, and .726; P = .017 between Tensor Trace and the cross-sectional area.
Conclusion:
Diffusion tensor imaging is an effective method to assess the changes in the microstructure of atrophic vocal fold muscle tissue after RLN injury.
Introduction
During normal voice production, active contraction of the thyroarytenoid (TA) muscle increases the tension of the vocal folds. After recurrent laryngeal nerve (RLN) injury, however, the TA muscle may lose function due to denervation, which results in a decrease in pitch, vocal fatigue, hoarseness, and loss of voice projection. 1,2 This denervated condition, known as unilateral vocal fold paralysis (UVFP), reduces patients’ quality of life, interfering with verbal communication and causing fatigue due to increased respiration during speech. 3 -6 The diagnosis and evaluation of unilateral vocal fold paralysis are often performed by stroboscopic laryngoscopy and laryngeal electromyography. Stroboscopic laryngoscopy allows visual observation of the movement of vocal folds, based on which otolaryngologists make subjective evaluations. Laryngeal electromyography, on the other hand, is invasive and difficult to operate, and, as a qualitative and semiquantitative examination, the diagnosis of laryngeal electromyography lacks clear and unified criteria. 7,8 Although these methods are commonly used in clinical practice, there is no thorough, complete evaluation of the changes in vocal fold muscle microstructure. Besides changes in the midline position of the vocal folds, patients with UVFP may experience decreased stiffness and tension, decreased vocal fold thickness, and TA muscle atrophy. Additionally, patients with UVFP may experience associated movement of the affected side of the vocal folds that adversely affects vibration, which further impacts voice quality. 5
Diffusion tensor imaging (DTI) is a new technique for calculating the diffusion properties of water molecules in tissues, 9,10 a noninvasive method for characterizing soft tissue properties at the microstructural level. 11,12 The DTI has been used as a highly sensitive imaging method for skeletal muscle. 13 -15 Two DTI parameters, fractional anisotropy (FA) and Tensor Trace, can be applied to reflect changes in the internal structure caused by active movement of healthy muscles and changes in the internal structure of atrophic muscles after denervation. 16,17 Fractional anisotropy refers to the anisotropy of water molecules in tissues and is a common index in DTI magnetic resonance imaging (MRI) for describing the directional correlation of water diffusion in tissues. Fractional anisotropy ranges from 0 to 1; 0 indicates that the dispersion is not limited; for example, the FA value of cerebrospinal fluid is close to 0. For regular directional tissues, the FA value is greater than zero and near 1 for tissues with high directionality. The FA of white matter fibers in the brain, for instance, is close to 1. The diffusion tensor, referred to as Tensor Trace in this article, reflects the total water content of the tissue in mm2/s. Tensor Trace is a commonly used clinical measurement, and its changes are attributed to changes in the tissue microstructure. 17 -20
The DTI–MRI is a noninvasive method for assessing the histological characteristics and pathology of atrophic muscles. However, there is no current research on DTI assessment of vocal fold muscle fiber atrophy, common in UVFP. This study uses DTI to examine the microstructure of vocal fold tissue after RLN injury.
Materials and Methods
Model Preparation
This study was carried out in compliance with the Guidelines for Animal Experimentation at the School of Medicine, Xiamen University. Six healthy adult canines were selected for the experiment. The canines were all females, the same breed and age, and were raised with a similar diet and living environment. All dogs weighed between 10 and 11 kg at the time of denervation. Laryngoscopy was used to confirm normal vocal fold appearance. Each dog of the experimental group was fixed to the operating table in a supine position and anesthetized with sodium pentobarbital. The 6-cm incision began at the upper edge of the cricoid cartilage and proceeded inferiorly. The cervical anterior band muscle was separated, the trachea was exposed, and the paratracheal and esophageal tissues were separated. The right RLN was exposed and resected after confirmation by laryngeal electromyography. The proximal nerve stump was sutured onto the sternothyroid muscle to prevent reinnervation (Figure 1). No surgery was performed on the dogs of the control group. To prevent reinnervation of the RLN which may occur beyond 3 months denervation, 21 we sacrificed the canines after the fourth month.
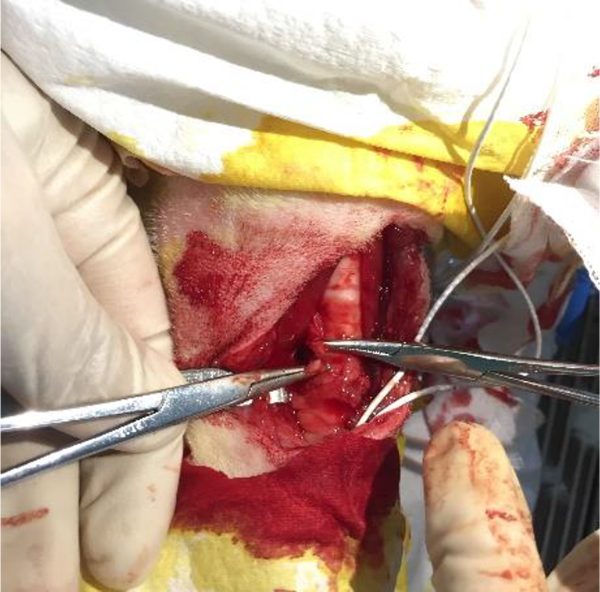
Recurrent laryngeal nerve (RLN) resection. The clamp of the hemostatic forceps is near the separated RLN.
Diffusion Tensor Imaging
All 6 canines were euthanized 4 months postinjury, and their larynges were excised. The supraglottic tissue was removed, and the vocal folds were exposed. Each canine larynx was immediately placed in the 9.4T Bruker BioSpec small animal MRI imaging system. Coils with a diameter of 20 mm were selected, and each larynx was placed in the same position in the coils. The scanning range spanned from the inferior edge of the cricoid cartilage to the upper edge of the false vocal fold. Scanning parameters were as follows: axial fast 2-dimensional T2-weighted image, echo time (milliseconds)/repetition time (milliseconds) 20.5/2500.0, and acquisition time of 10 minutes. In all sequences, the cross-sectional thickness was 1 mm. The parameter maps derived from the T2-weighted and DTI images were matched and compared. During the experiment, each vocal fold was wrapped with plastic wrap to prevent moisture loss. A T2 MRI image was used to orient the laryngeal anatomy to select regions of interest in the lamina propria and the muscle layer (Figures 2 and 3). The FA and Tensor Trace for the selected regions of interest were calculated with Bruker PV5.1 software.
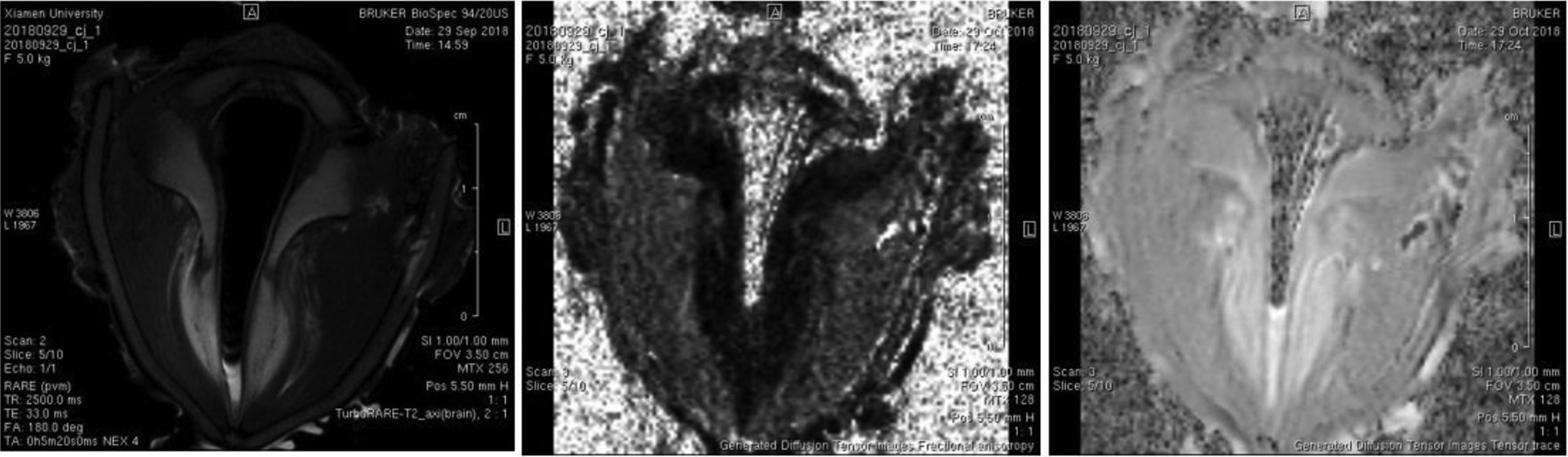
Example diffusion tensor imaging (DTI) maps of unilateral vocal fold paralysis (T2, fractional anisotropy [FA], Tensor Trace images from left to right).
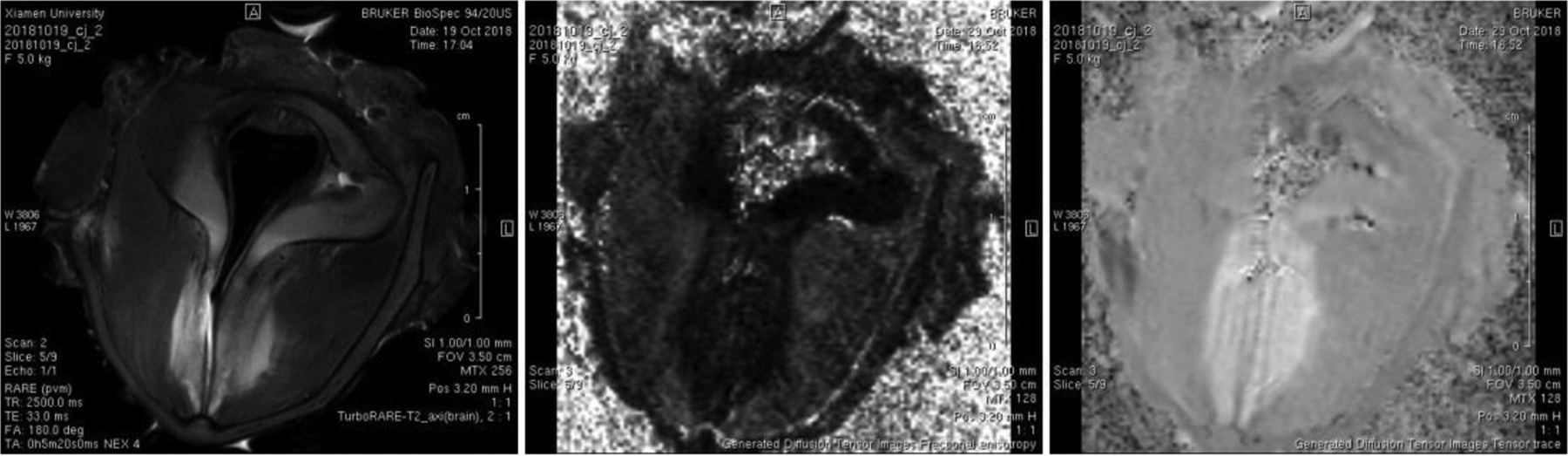
Example diffusion tensor imaging (DTI) maps of normal vocal folds (T2, fractional anisotropy [FA], Tensor Trace images from left to right).
Histological Section Preparation
Immediately after the MRI scan, the vocal folds were sectioned and stained with hematoxylin–eosin staining and digitally scanned by Aperio Digital Pathology Slide Scanners (Aperio XT; Leica; USA). A target detection and extraction technique was used to analyze an 0.264 mm2 area in the middle of the slice. The number of muscle cells in the muscle layer and the cross-sectional area of vocal fold muscle fibers were calculated (Figure 4).

Histological sections of the vocal fold muscle layer in the control group and the unilateral recurrent laryngeal nerve (RLN) injury group. (Hematoxylin and eosin [H&E] stain, magnification level 16 × 16).
Statistical Methods
The statistical analysis was performed using SPSS 22.0 statistical software. For each group, mean values and standard deviations were calculated. The data between the control group and the unilateral vocal fold paralysis group were compared using a paired t test; P <.05 was considered statistically significant.
Results
Results of DTI
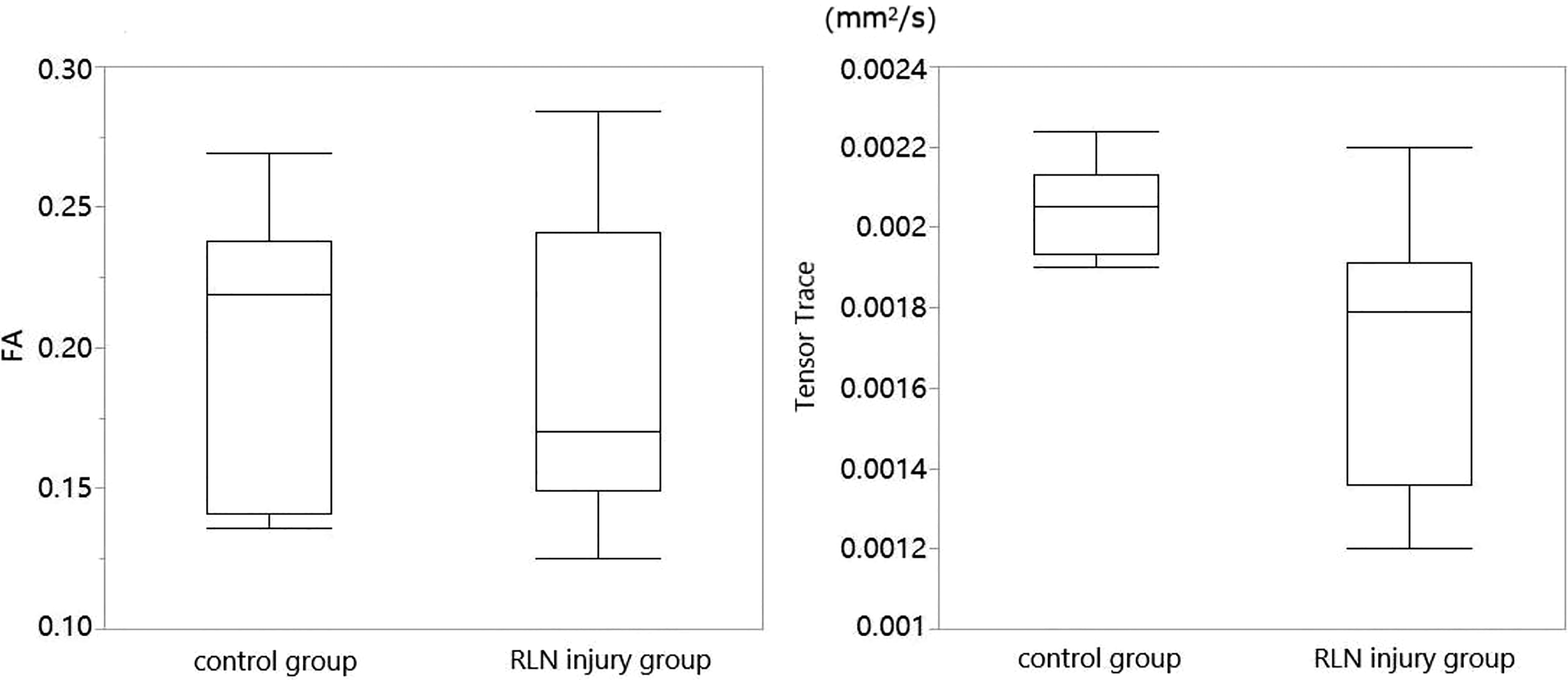
In the vocal fold muscle layer, the FA of the unilateral RLN injury group was higher than that of the control group, P = .009, and the Tensor Trace was lower than that of the control group, P = .001. Both differences were statistically significant. In the lamina propria, the FA of the injury group was lower than that of the control group but was not statistically significant, P = .329. The Tensor Trace was lower than that of the control group, and this difference was statistically significant, P = .001 (Figures 5 and 6; Table 1).
Comparison of diffusion tensor imaging (DTI) parameters between the control group and the recurrent laryngeal nerve (RLN) injury group in the lamina propria. A significant difference in Tensor Trace was observed. The upper/lower bounds represent the 95th/5th percentiles, and the middle line represents the median.
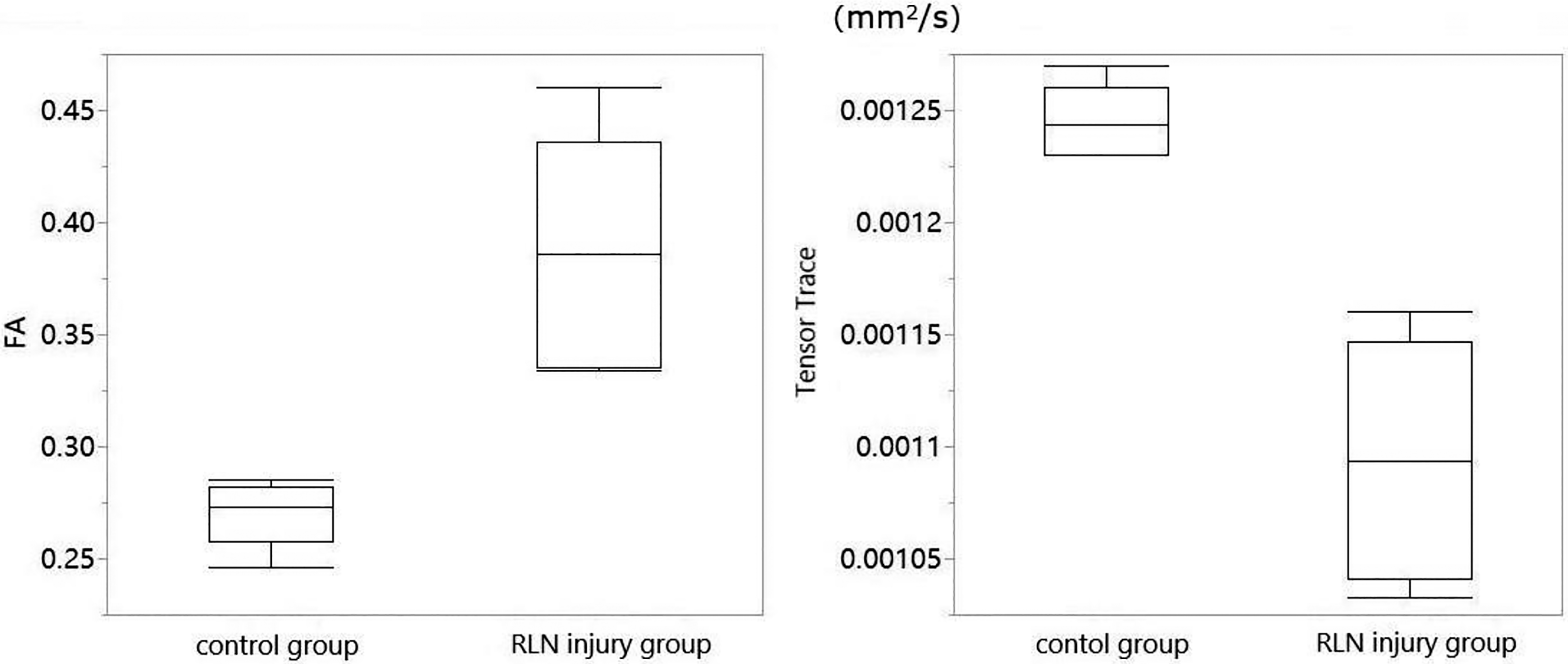
Comparison of diffusion tensor imaging (DTI) parameters between the control group and the recurrent laryngeal nerve (RLN) injury group in the muscle layer. The fractional anisotropy (FA) of the RLN injury group was higher than that of the control group, P = .009, and the Tensor Trace was lower than that of the control group, P = .001. The upper/lower bounds represent the 95th/5th percentiles, and the middle line represents the median.
Comparison of Tensor Trace and FA in the Lamina Propria and Muscle Layer Between the RLN Injury Group and the Control Group.
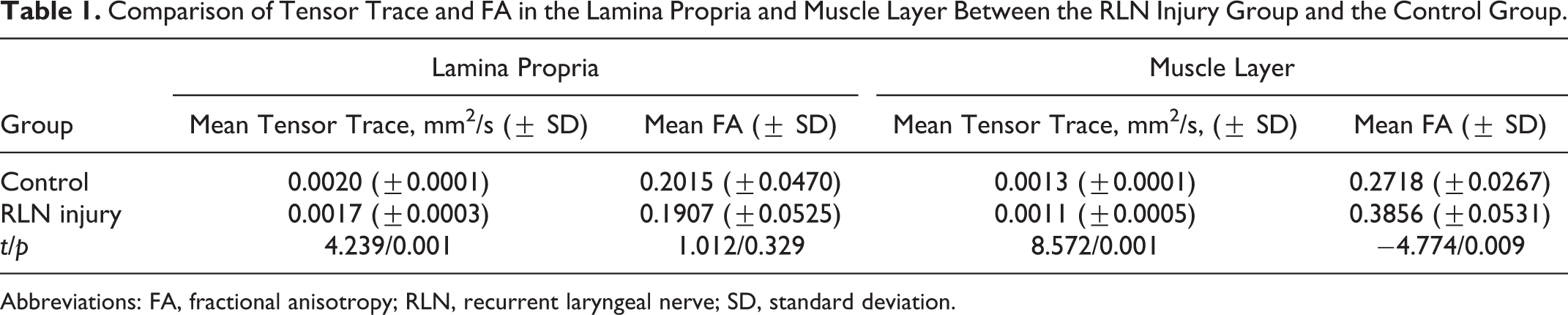
Abbreviations: FA, fractional anisotropy; RLN, recurrent laryngeal nerve; SD, standard deviation.
Pathological Section Results
The cross-sectional area of vocal fold muscle fibers in the RLN injury group was significantly lower than that in the control group, P < .001 (Figure 7). The vocal fold muscle fiber density in the RLN injury group was also lower than that of the control group, P < .001 (Figure 8).
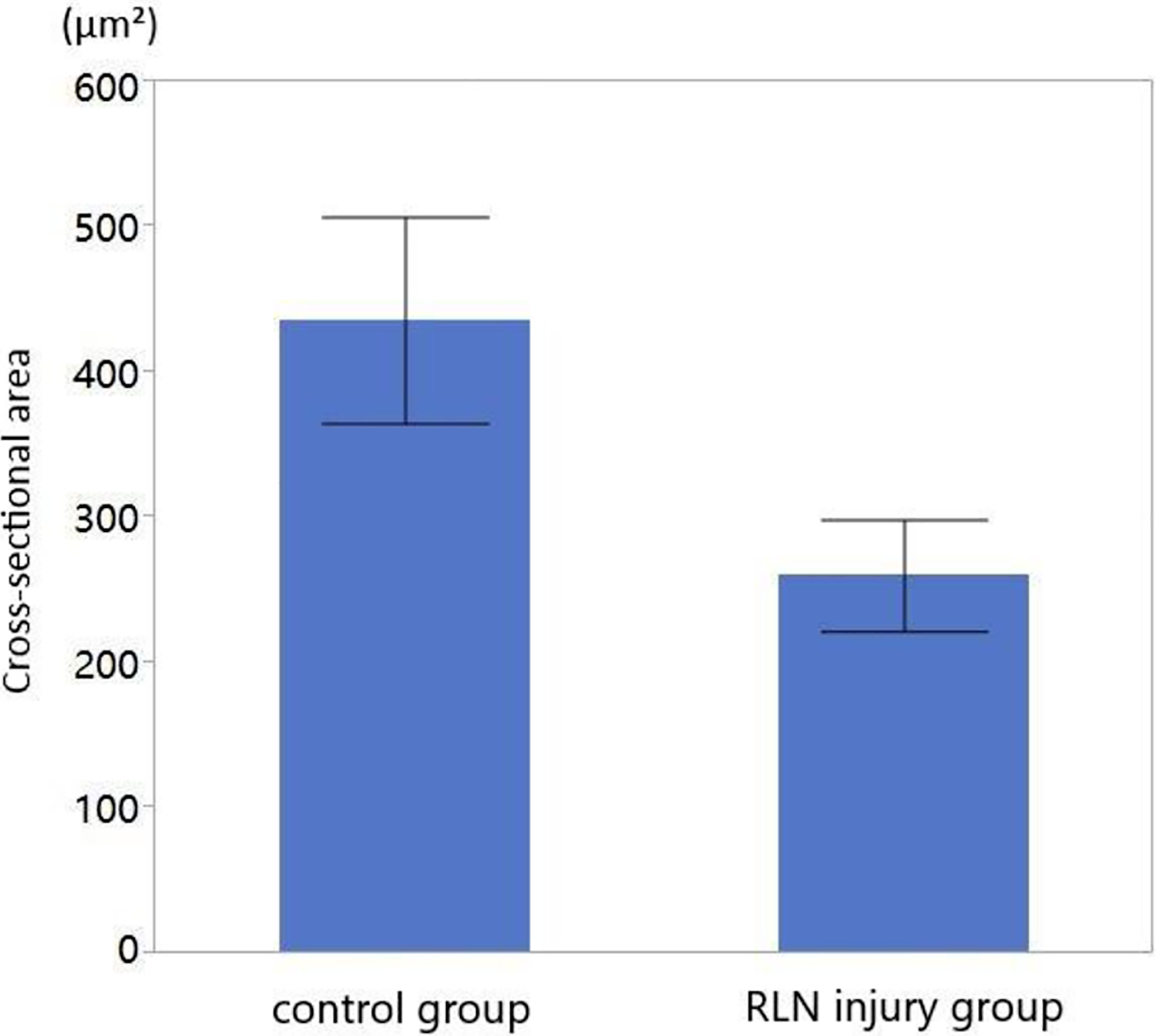
Cross-sectional area of vocal fold muscle fibers in the control group and the recurrent laryngeal nerve (RLN) injury group. At 4 months after RLN injury, the cross-sectional area of vocal fold muscle of the RLN injury group was significantly lower than that in the control group, P < .05.
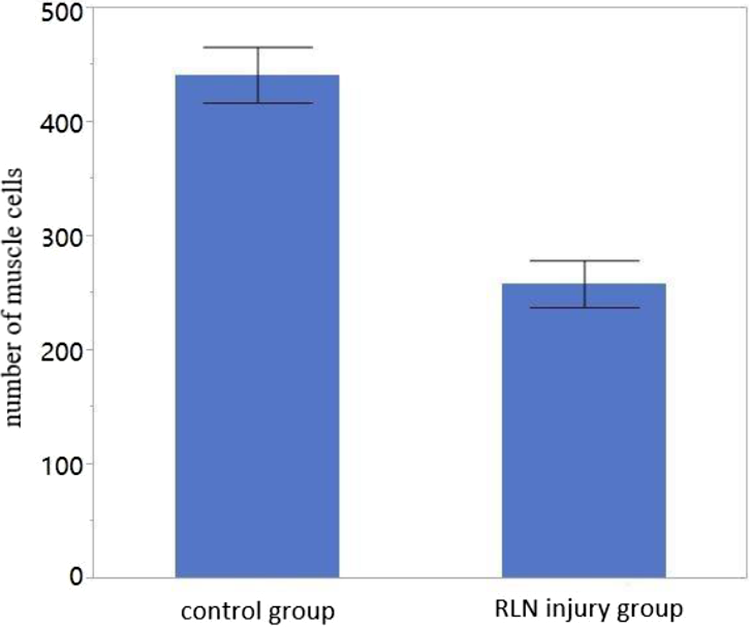
Vocal fold muscle cells in the control group and the recurrent laryngeal nerve (RLN) injury group. At 4 months after RLN injury, the number of cells in the RLN injury group was significantly lower than that in the control group (P < .05).
Correlation Analysis
Pearson correlation analysis was performed on the DTI and pathological slice results from both the injured group and the control group. The correlation coefficient between the FA and the cross-sectional area was −0.838, P = .002, and the correlation coefficient between the Tensor Trace and cross-sectional area was 0.726, P = .017 (Figure 9).
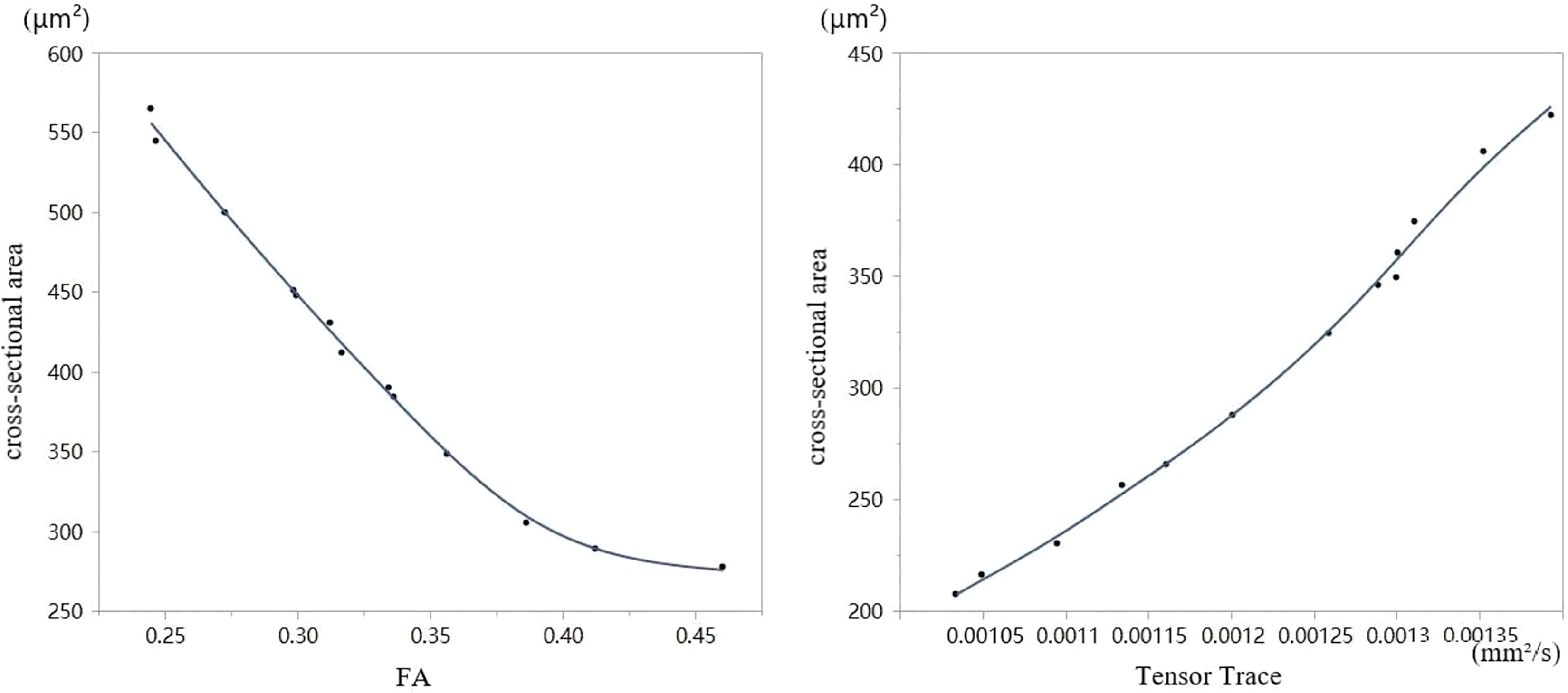
Pearson correlation analysis was performed on the diffusion tensor imaging (DTI) and pathological slice results from both the injured group and the control group. The relationship between cross-sectional area (μm2) and fractional anisotropy (FA) is depicted on the left, demonstrating a negative correlation between the variables. On the right, the relationship between the cross-sectional area and Tensor Trace (mm2/s) is depicted, demonstrating a positive correlation between the variables.
Discussion
This study provided preliminary evidence for DTI as a method of evaluating changes in the vocal fold microstructure. A correlational analysis between DTI measurement results and pathological slice characteristics demonstrated that the DTI parameters, FA and Tensor Trace, reflected changes in the vocal fold muscle structure after RLN injury. In the control group, the FA of the vocal folds was lower than the experimental group, and the Tensor Trace was higher. The cross-sectional area of muscle fibers in the RLN injury group and the muscle density decreased. These findings indicate that vocal fold muscles experience structural changes in muscle cells due to denervation.
Past studies provide evidence of similar changes without the use of DTI. Following RLN injury, vocal fold muscles have been shown to undergo pathological processes such as decrease in muscle volume, loss of contractile function, and gradual atrophy of muscle fibers due to denervation. 22,23 Yumoto et al found that the muscle fiber density in the vocal fold muscular layer became thinner and was surrounded by dense fibrous tissue. Additionally, the lamina propria was thinner after RLN injury. 1 Because our use of DTI has implicated similar structural changes, we may consider this converging evidence supporting the integration of DTI for diagnosing these changes.
Diffusion tensor imaging has also been used for assessment of the microstructure of atrophic muscles in other tissues following denervation. 24 -26 Satome et al used DTI to explore denervated skeletal muscle of rats. It was found that the FA of atrophic, denervated muscle was significantly higher than that of normal muscle, and apparent diffusion coefficient (ADC) was lower. 17 Zhang et al established a denervated muscle atrophy model after unilateral sciatic nerve transection. In denervated skeletal muscles, FA measurements obtained by DTI were significantly higher than the FA of muscles on the uninjured side. These past findings indicate that DTI is sensitive to detect skeletal muscle atrophy. 27 Presently, we found that vocal fold muscle experienced similar changes in DTI parameters as other types of skeletal muscle following denervation, which indicates the potential of this technology as a diagnostic tool for measurement of atrophy in the vocal folds.
In addition to vocal fold muscle atrophy, previous studies have shown that after injury of the recurrent laryngeal nerve, muscle density decreases the cross-sectional area of muscle fibers becomes smaller, and fiber diameter decreases. 28 -30 In our study, we also found that, in the pathological sections of the canine vocal fold, the cross-sectional area of the vocal fold muscle fibers was reduced, and muscle density decreased in the RLN injury group. In addition, our DTI measurements of FA and Tensor Trace showed the DTI parameters of the vocal fold muscle were significantly different between the control group and the RLN injury group, consistent with the pathological section results of the vocal fold. This further indicates that DTI could be used as an effective method to evaluate the microstructural changes in vocal fold muscle fibers after RLN injury. Previous studies have shown that the change in diffusion tensor of water molecules in atrophied muscle is closely related to the change in microstructure of muscle fibers. 31 -33 Previous pathological studies on neurogenic muscular atrophy have shown that many morphological and metabolic changes occur rapidly in denervated muscles. 34,35 Atrophic muscle can result in a decrease in muscle volume, growth of connective tissue between muscle bundles, and decrease in muscle tension. 36,37 These studies are consistent with our conclusions. Due to denervation and atrophy of the vocal fold muscle, the muscle volume decreased and the cross-sectional area and diameter of the muscle fibers became smaller, to some extent, which limits the lateral diffusion of water molecules resulting in an increase of FA and a decrease of Tensor Trace.
In the lamina propria, the FA of the unilateral RLN injury group was lower than that of the control group, but the difference was not statistically significant, P = .329. The Tensor Trace was also lower than that of the control group. This difference was statistically significant, P = .001. As the lamina propria of the vocal fold is mainly composed of collagen fibers and proteins, the regularity of its arrangement is not as obvious as the trend of muscle fibers. Therefore, there is no significant difference in FA.
Our experiment is not without limitations. While the larynges were wrapped throughout the experiment, we cannot rule out the loss of moisture altering our measurements. Furthermore, limitations of DTI and MRI procedures limit us from performing scans without excising the larynges. One such limit arises due to the size of the MRI coil; the canine larynges can only be scanned by magnetic resonance after excision to fit into the machine. Therefore, the diffusion characteristics of water molecules in vocal fold muscle cannot be dynamically observed at different time after injury of the recurrent laryngeal nerve. Using smaller animals suitable for the size of magnetic resonance coils or future improvements in DTI technology will allow improved experimental conditions to measure DTI in vivo.
Fractional anisotrophy and Tensor Trace, as measures of anisotropic viscoelastic properties, have the potential to serve as valuable diagnostic tools to detect changes in water content (indicating an inflammatory response) and tissue stretch which would impact vocal function. Additionally, DTI may have applications for investigation of the molecular mechanism of vocal fold changes after RLN injury and subsequent vocal changes. Clinically, cricoarytenoid joint dislocation and RLN injury can both lead to vocal fold fixation, so the diagnosis of these 2 diseases is difficult. Cricoarytenoid joint dislocation can also cause dysfunction atrophy of the vocal fold muscle. So, in future studies, we will consider the microstructural differences between RLN injury and cricoarytenoid joint dislocation to provide the basis for differential diagnosis of these 2 diseases.
Conclusion
In this study, diffusion tensor parameters in atrophic vocal fold muscle fibers were obtained by DTI. Atrophy of vocal fold muscle after denervation led to an increase in the anisotropy of the muscle fibers, a decrease in Tensor Trace, and a decrease in the cross-sectional area of muscle fibers. These findings indicate that DTI can be a useful diagnostic to assess microstructural changes in vocal fold tissue following RLN injury.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China, NSFC81371080.