
Abstract
Background:
Vocal fold paralysis (VFP) can result from a variety of diseases or surgeries and has various causes. This study determined concurrent etiologies in patients who were treated in a teaching hospital (tertiary medical center).
Methods:
A retrospective review of medical records of patients with VFP from September 2010 to December 2019 was performed to determine the etiology. Patients with laryngeal/hypopharyngeal malignancies, those with incomplete examination and follow-up data were excluded from the study. During the follow-ups, cases involving recovery were also excluded.
Results:
One hundred and ninety-four patients with a determined etiology were included: 113 males and 81 females. Unilateral VFP was present in 178 patients, and 16 presented with bilateral VFP. The causes of unilateral VFP were surgical for 61.3%, neoplastic for 17.5%, idiopathic for 10.3%, traumatic for 1.5%, central for 4.7%, cardiovascular for 2%, radiation-induced for 1.5%, and inflammatory for 1%. Thyroidectomy was the most common surgery for unilateral VFP and was the cause for 54 patients. Lung cancer was responsible for 15 cases and was the most common neoplastic etiology of unilateral VFP. For those who presented with bilateral VFP, surgery was the most common cause and accounted for 56.3% of the incidences. In terms of gender, surgery was the most common cause for both sexes, accounting for 62 of 113 male patients and 57 of 81 female patients. Four cases recovered during the follow-ups and these were excluded.
Conclusion:
Surgery and in particular, thyroidectomy, was the most common cause of VFP for these series. Central nervous system disorders were the cause of VFP (4.5%). Central nervous system disorders, especially cerebrovascular accidents that induced VFP, could not be neglected. Radiation-induced cranial nerve paralysis in the head and neck cancer was possible causes. The percentage for the causes of unilateral VFP, surgery increased and the percentage for neoplasm decreased for Taiwan.
Introduction
Laryngeal motor innervation can result in damage to the neck and mediastinum. The damaged area is usually in the region of the aortic arch (on the left side) or the subclavian artery (on the right side), or in the tracheoesophageal groove. Vocal fold paralysis (VFP) is defined as the loss of normal adduction/abduction due to a lesion that is distant from the vocal cords, as a result of neural injury to the recurrent laryngeal nerve (RLN). Vocal fold paralysis has many known causes, including trauma, malignancy, and surgery. Vocal fold paralysis can be idiopathic but it can also present features of many serious underlying disease processes.1-5 Mechanical fixation of the cricoarytenoid joint can occur after cricoarytenoid dislocation, local inflammation, or neoplastic invasion. The term VFP is used to indicate totally or partially impaired laryngeal movement due to neurological injury, which can affect the larynx unilaterally or bilaterally. Some studies show that the frequency of the various causes of VFP are changing.6-9 The etiology of laryngeal paralysis has changed over time, with a decrease in the prevalence of malignancies and a recent increase in cases that are attributable to thyroid surgery.
This study determined the contemporary etiology of unilateral and bilateral VFP, other than primary laryngeal and hypopharyngeal cancers. During the follow-ups, cases involving recovery were also excluded.
Methods
This retrospective study enrolled 194 consecutive patients with VFP who visited and registered at the author’s practice. The research project was approved by the institutional review board. All studies were performed in accordance with relevant guidelines and regulations. For all patients, VFP was confirmed using a flexible or rigid laryngoscope. The motion of the vocal folds was demonstrated in a vertical view via a laryngoscope check.
This study involved a retrospective review of the records of all patients with the relevant diagnostic code from September 2010 to December 2019 in this teaching hospital. Records were analyzed for sex, age, side of paralysis, and cause of paralysis. The etiology of vocal immobility was determined using the history and a complete head and neck examination. Other examinations, such as chest radiography, ultrasonic echography of the neck and computed tomography or magnetic resonance imaging were performed when required. Exclusion criteria included VFP due to laryngeal or hypopharyngeal malignancies, incomplete examinations, and follow-ups. During the follow-ups, cases involving recovery were also excluded.
The etiologies were categorized to allow comparisons with previous major studies. Idiopathic paralysis was diagnosed if a cause for VFP was not determined after an adequate diagnostic evaluation.
Results
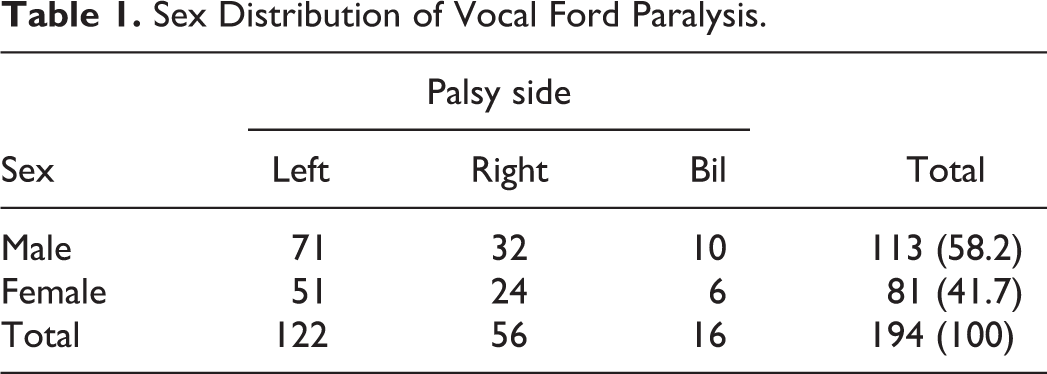
One hundred and ninety-four patients with VFP were identified, including 178 cases with unilateral VFP and 16 with bilateral VFP. The mean age at diagnosis was 61 years, with a range from 16 to 94 years (Figure 1). The causes of unilateral and bilateral VFP and the gender distribution are shown in Table 1. For patients with unilateral VFP, left VFP was diagnosed in 122 (69%) patients and the right vocal cord was paralyzed for 56 (31%) patients. One hundred and thirteen (58%) patients were men and 81 (42%) were women. Surgery was the most common cause of VFP, accounting for 119 (61.3%) patients (Table 2). The surgical procedures included thyroidectomy for 56 patients, surgery on the esophagus for 44, the thorax (lung and heart surgery) for 13, and the spine for 3 (Table 3).
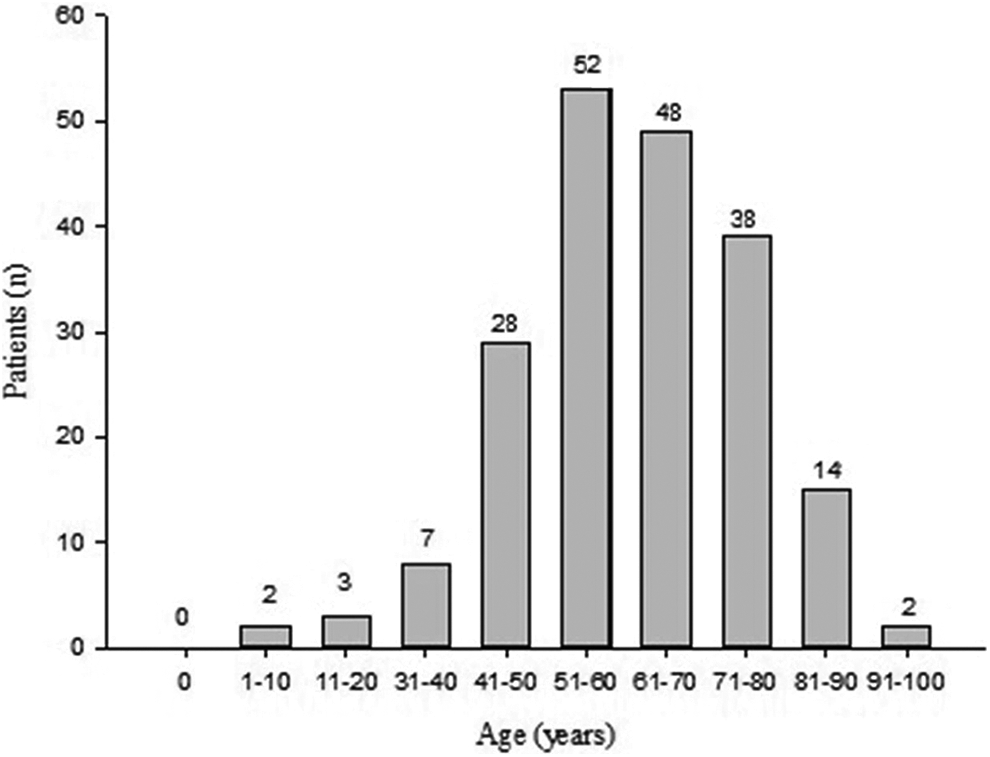
Age distribution (n = 194).
Sex Distribution of Vocal Ford Paralysis.
Etiology for Vocal Cord Paralysis.a
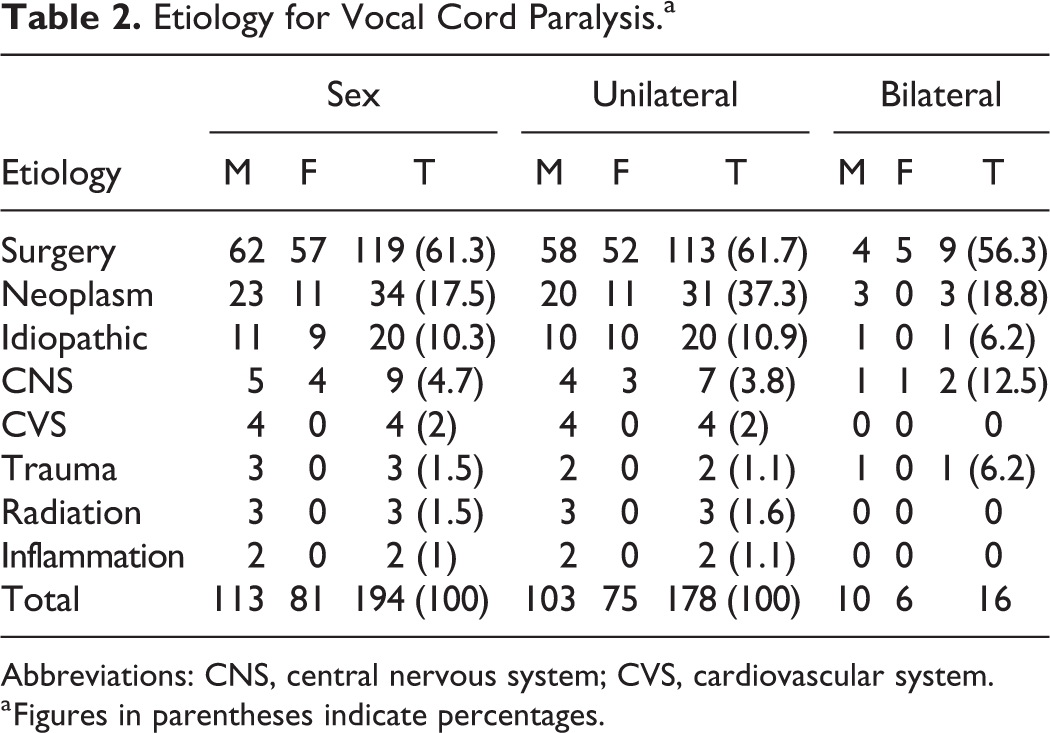
Abbreviations: CNS, central nervous system; CVS, cardiovascular system.
a Figures in parentheses indicate percentages.
Types of Surgery for Vocal Cord Paralysis.a
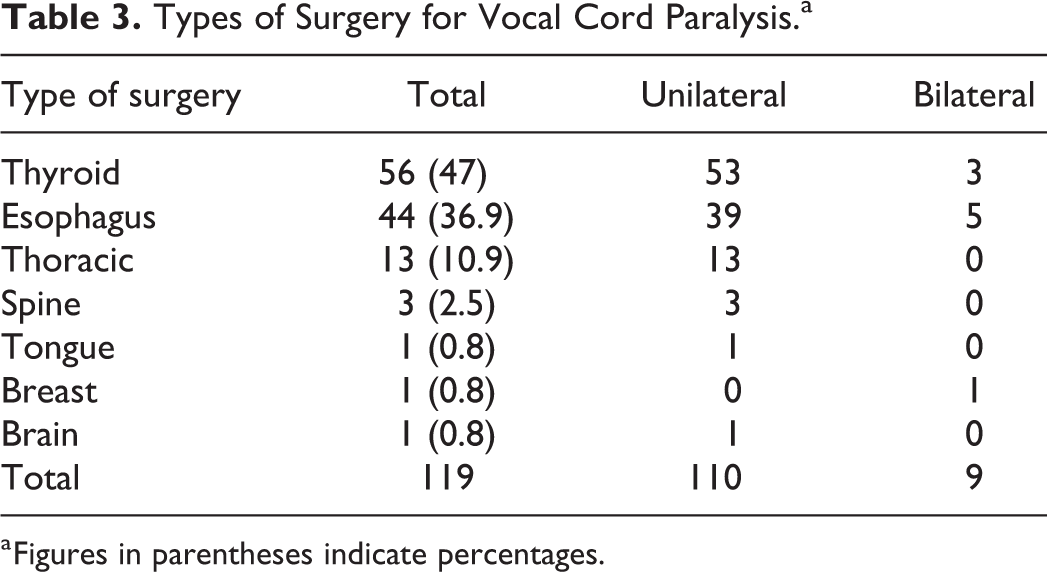
a Figures in parentheses indicate percentages.
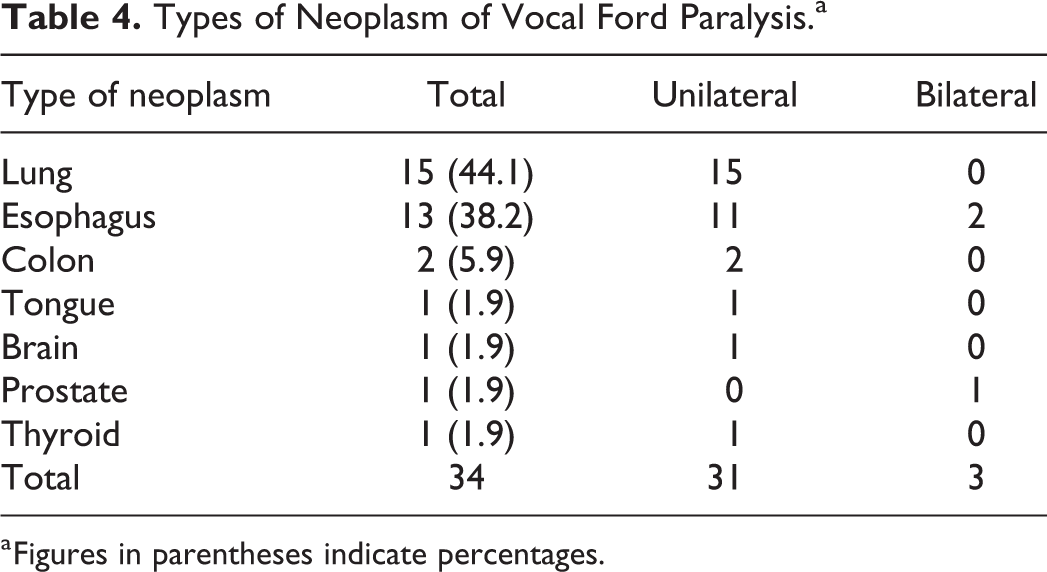
Neoplasm was the second most common cause of VFP. Of the 34 (17.5%) patients with a neoplastic cause, 15 had lung cancer, 13 had esophageal cancer, 1 had breast cancer, 1 had a benign thyroid tumor, 2 had colon cancer, and 1 had a brain tumor (Table 4).
Types of Neoplasm of Vocal Ford Paralysis.a
a Figures in parentheses indicate percentages.
Idiopathic paralysis was the third most common etiology and was noted for 20 (10.3%) patients (Table 2). Trauma was the cause of VFP for 3 (1.5%) patients, with intubation injury being responsible for 2 of these. For 9 (4.7%) patients, VFP was the result of a central nervous lesion. Radiation-induced VFP accounted for 3 (1.5%) patients, 2 of which were nasopharyngeal carcinoma (NPC) post radiation cases. For 2 (1%) patients, VFP was the result of an inflammatory process and for 4 (2%) patients it was caused by cardiovascular disease.
In terms of gender for VFP, surgery was the most common cause, accounting for 62 of 113 males. Surgery was also the most frequent cause for 57 of 81 females.
Ten men and 6 women were diagnosed with bilateral VFP. Similarly to unilateral VFP, the leading cause for bilateral VFP was surgery, accounting for 9 of the 16 cases. Neoplasm was the second most common cause. Esophageal cancer was the cause of most neoplasm-related incidences. Four cases recovered during the follow-ups and these were excluded.
Discussion
Vocal fold paralysis can be caused by a variety of diseases or surgeries. There are many studies of VFP but the exact incidence of VFP is still difficult to determine.10-13 This study showed that the incidence of VFP increased with the age of the patient. The peak incidence was between 51 and 70 years. This was probably a result of the increased incidence of tumor and neurological damage in aging individuals. More male patients than females had unilateral or bilateral VFP, possibly because there was an increase in postsurgical cases resulting from surgery for lung and esophageal cancer for males.
Left VFP occurs about twice as frequently as right VFP. This result was comparable with those of previous studies.5-8 The longer course of the left RLN may account for this variation. Studies showed that neoplasm, surgery, and idiopathic paralysis were the 3 main causes of unilateral VFP (Table 4).9-13
Studies of bilateral VFP were limited but the incidence was about 10% of that for VFP. The results of this study agreed with those of previous studies.9-13 The etiology for bilateral VFP included thyroidectomy, malignancy, trauma, neurological, and idiopathic paralysis. 14 Previous studies showed that neoplasm was the most common etiology in the West and in Taiwan.2,13,15,16 This study showed that surgery was the main cause, followed by neoplasm and central nervous system lesions. Some studies showed that thyroid surgery was decreasing as a cause of VFP because of improved techniques but thyroidectomy was still the most common cause of VFP for this study and others.12,13,16
Esophageal operation was the second most common surgical cause. Vocal fold paralysis in patients who are subject to open-heart surgery, lung surgery, and cervical spine surgery increases due to more frequent operations.1,12 Vocal fold paralysis after cervical spine surgery most frequently occurred on the right side. Studies showed that more than 80% of right RLN enter the larynx at or below C6 to C7. 17 The right RLN approaches the larynx at a wider angle, relative to the sagittal plane, than the left so the right is at a greater risk than the left when a retractor is used during cervical spinal surgery. 18 Neuro or ortho surgeons use an anterior approach for the cervical spine, neck dissection, and other operative procedures along the course of the RLN and this may contribute to the risk of VFP. During anterior cervical discectomy and fusion surgery, the RLN can be exposed and injured. Vocal fold paralysis after an open-heart surgery is usually on the left side because the left RLN passes across the aortic arch.
In terms of changes in the etiology of unilateral VFP, the results of this study were in agreement with those of previous studies,1,9 with some exceptions. Neoplasm accounted for 17.5% of the cases for this study. The most common neoplasm was lung cancer for 15 patients. All of these patients exhibited unilateral VFP and 14 patients had paralysis on the left side, possibly because the intrathoracic portion of the left RLN is longer on the left than on the right side. Esophageal cancer was the second most common neoplasm. This study has 1 patient with a benign thyroid tumor who developed VFP without surgery. Vocal fold paralysis is possible after benign neoplasms such as neurogenic tumors and paragangliomas and after a benign thyroid tumor. About 0.7% of patients with benign thyroid neoplasms have RLN paralysis. 19 Cases of idiopathic VFP have no obvious causes. Idiopathic causes accounted for 10% to 41.3% in previous studies. 1 In this study, 10.3% of VFP was idiopathic. There was no clear reason for the lower incidence of idiopathic VFP but it might be because most patients in this study were referred after operations and for management only.
Central nervous system disorders were the cause of VFP for 9 (4.7%) patients. Central nervous system disorders that induced VFP include Parkinson disease and cerebrovascular accidents and the incidence of these increased with age. Seven cases had cerebrovascular accidents in this study. Trauma was the cause of VFP for 3 (1.5%) patients. The mechanism might involve compression of the RLN by the lateral arytenoids, thyroid cartilage, and an inflated cuff from an endotracheal tube. It has been shown that after intubation or a neck injury, the RLN can become infected by viral attack, such as herpes zoster. 20 Trauma causes VFP after traffic accidents and penetrative neck wounds.
This study identified radiation as a cause of VFP for 3 (1.5%) patients. Radiotherapy is an effective and commonly used treatment for head and neck cancer. However, radiotherapy affects both the tumor and the surrounding normal tissues and adverse sequelae can develop. Cranial nerve palsy, secondary to fibrosis in the head and neck region, is a rare late complication. It is reported for various head and neck cancers in the nasopharynx, hypopharynx, larynx, neck, tonsil, and tongue base. The hypoglossal nerve is the most frequently affected nerve after radiotherapy for head and neck cancers, followed by the vagus nerve and the RLN. The 3 most commonly reported head and neck cancers with radiation-related VFP were those of the nasopharynx, tonsil, and tongue base.21,22 The incidence of radiation-induced VFP in NPC patients was less than 1%. 23 NPC patients are more prone to cranial nerve palsy than patients with other head and neck cancers, possibly because of the anatomic proximity of the nasopharynx to the skull base, so the cranial nerves are inevitably irradiated. It is important to exclude any other possible etiology before making a diagnosis of radiation-induced VFP. Cranial neuropathy in patients with head and neck cancer is far more likely to be caused by tumor recurrence, regional metastasis, or a second primary tumor than by irradiation. It is difficult to distinguish between radiation-induced palsy and that due to true malignancy. History, physical examination, imaging studies, endoscopy with a biopsy, and observation over time are required for a correct diagnosis.
Inflammatory processes that induce VFP include pneumoconiosis, pulmonary tuberculosis, and deep neck infection. CVS disorders were the cause of VFP for 4 (2%) patients. Etiologies of cardiovascular diseases, so-called Ortner’s syndrome, include cardiac tamponade, cor pulmonale, and rheumatic heart disease.
When a patient was diagnosed with vocal palsy, there was little chance of recovery. This series study excluded for only 4 recovery cases by long-term follow-up. General physicians usually refer patients with poor phonation or VFP to otolaryngologists after conservative treatment. The recovery rate might be underestimated for this series. Most cases were referred for further management only.
Surgery, neoplasm, idiopathy, and trauma are the main 4 reported causes of unilateral VFP in 5 previous studies.1,12, 13 , 15,16 A review of the 4 main causes of unilateral VFP was undertaken. The studies used the same methodology, including the 3 retrospective Taiwanese studies (Table 5). The inclusion criteria for these studies were similar to those for this study. Previous studies also determined the contemporary etiology of unilateral and bilateral VFP, other than primary laryngeal and hypopharyngeal cancers. Surgery as a cause for unilateral VFP increased from 22% to 61.3% in Taiwan and neoplasm as a cause decreased from 39% to 17.5%. Idiopathic causes still account for 10% to 20% and this result was in agreement with those of previous studies. Trauma as a cause decreased from 14.3% to 1.5%, possibly because of improvements in intubation devices during anesthesia or emergency intubation using a scope guide.
Review of 4 Main Causes of Unilateral Vocal Fold Paralysis.

Conclusion
Surgery was the most common cause of VFP for this series. Thyroid surgery was the leading etiology for both males and females. Before the cause of RLN paralysis was labeled idiopathic, the possibility of a neoplasm must be ruled out. Central nervous system disorders also cause VFP (4.7%). Central nervous system disorders, especially cerebrovascular accidents that induced VFP, could not be neglected. Radiation-induced cranial nerve paralysis could also occur after some head and neck cancers post radiotherapy. The percentage for the causes of unilateral VFP, surgery increased and the percentage for neoplasm decreased for Taiwan.
Footnotes
Acknowledgments
This work was supported in part by the Taipei Medical University—Shuang Ho Hospital (108FRP-08).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.