
Abstract
Nasal septal deviations (NSD) have been categorized into 7 types. The effect of these different deviations on airflow pattern and warming function has not been fully investigated. The purpose of this study was to utilize a computational fluid dynamics approach to assess the impact of NSD of varying types on nasal airflow and warming function. Patients with each type of NSD were enrolled in the study, and a normal participant as the control. Using a computational fluid dynamics approach, modeling of nasal function was performed. Indices of nasal function including airflow redistribution, total nasal resistance, airflow velocity, and airflow temperature were determined. Among all types of NSD, the maximal velocity and total nasal resistance were markedly higher in type 4 and 7 deviations. The flow partition and velocity distribution were also altered in type 4 and 7 as well as type 2 and 6 deviations. Airflow in all categories of NSD was fully warmed to a similar degree. From a computational aerodynamics perspective, the type of septal deviation may contribute to altered airflow characteristics. However, warming function was similar between septal deviation types. Future studies will help to ascertain the functional importance of septal deviation types and the applicability of these computational studies.
Introduction
The nasal septum serves an important function in nasal structural support. 1 Deviation of the nasal septum is common with an incidence considered to be up to 70% to 90%. 2 Septal deviation may contribute to nasal obstruction and is therefore a common indication for septoplasty. 3 However, the efficacy of a septoplasty is variable; 4,5 thus, additional studies to ascertain the impact of septal deviations on nasal airflow may be beneficial.
Computational fluid dynamics (CFD) is an objective method to scale the airflow pattern and warming characteristics within the nasal cavity. 6 Chen et al reported the aerodynamic characteristics of one patient with a nasal septal deviation (NSD) using CFD. 7 In this study, they demonstrated that the NSD altered flow partitioning, nasal resistance, airflow velocity, intensity and location of turbulence, pressure distributions, and wall shear stress distribution in the nasal cavity. 7 The included case of NSD occurred in the middle portion of nasal cavity, which only represents the most common type of NSD. Evaluation of the various less common deviation types, however, was not performed in that study. 7
Among the classification systems for NSD, 8 the subdivision of NSD into 7 types was proposed by Mladina. 9 We hypothesized that nasal airflow pattern and warming function may be impacted by varying NSD deflection types 10,11 and that studying each NSD type may provide an improved understanding of the impact of NSD on airflow physiology. The purpose of this study was to utilize a CFD approach to investigate the impact of NSD with various deviation types on airflow pattern and warming function of the nasal cavity.
Patients and Methods
Study Population
Seven patients with each of the various types of NSD were enrolled for CFD analysis. Additionally, an asymptomatic patient with no septal deviation was utilized as a control. Informed consent was obtained from 8 participants, and the study protocol was approved by the Ethics Committee of Beijing Tongren Hospital.
The type of NSD was classified according to the method proposed by Mladina.
9,12
– Type 1 is a unilateral vertical septal ridge located at the valve region but does not reach the nasal valve. – Type 2 is a unilateral vertical septal ridge located at the valve region that touches the nasal valve, and the physiologic valve angle is decreased. – Type 3 refers to a unilateral “C” type vertical ridge that is located in the middle portion of the nasal cavity, opposite to the head of the middle turbinate. – Type 4 is a bilateral deformity consisting of type 2 on one side and type 3 on the contralateral side. The laterality of the anterior deflection was defined as the deviated side. – Type 5 is an almost horizontal septal spur that sticks laterally and deeply into the nasal cavity. – Type 6 refers to a large unilateral intermaxillary bone wing with a “gutter” between it and the rest of the septum on the ipsilateral side. On the contralateral side, there is an anteriorly positioned basal septal crest. – Type 7 is a combination of the abovementioned types.
Computational Fluid Dynamics
Computed tomography scan of the nasal cavities and paranasal sinuses combining the axial, coronal, and sagittal directions was performed. With a spatial resolution of 512 × 512 pixels and 0.625 mm thickness, DICOM (Digital Imaging and Communications in Medicine) format images were obtained. Segmentation and primary smoothing based on images were conducted in Mimics version 13.1 (Materialise, Leuven, Belgium) using the work station with 16 cores and 32G memory. The models constructed in Mimics 13.1 were then imported into Geomagic studio 12 (Geomagic, Cary, North Carolina) for further smoothing and surface partition, then the surface elements of IGES (Initial Graphics Exchange Specification) format were acquired for meshing work, which is a prerequisite step for fluid analysis.
The procedure for CFD simulation has been detailed previously. 6 To improve the accuracy of the simulation, mesh independent analysis was conducted in each individual to select the appropriate mesh number for final analysis. 13 Atmospheric pressure and 20°C were imposed at both nostrils in the simulation. The nasal wall was assumed to be no-slip (u = v = 0) and isothermal with a constant value of 34° C. 14 A constant flow rate of 15 L/min was applied at the anterior nostril as the simulated flow rate.
The data processing work was conducted in CFD-Post (ANSYS, Canonsburg, Pennsylvania) to get contour visualization and value calculation. We created 5 coronal planes in 3-dimensional models to assess the velocity and temperature contours. The coronal planes were positioned at the nasal valve (plane 1), head of the inferior turbinate (plane 2), head of the middle turbinate (plane 3), midportion of the middle turbinate (plane 4), and mid-nasopharynx (plane 5). Indices such as flow partition, total nasal resistance, airflow velocity, and temperature were analyzed and compared among the various types of septal deviation.
Results
The average age of participants in this study was 27.88 years of age with 50% (4/8) male (Table 1). First, we assessed the airflow redistribution in the nasal cavities of normal and each type of the septal deviation. The airflow was almost evenly partitioned between both nasal cavities in the control, type 1 and type 5 deviations. However, the volume of airflow distribution in the nondeviated side was higher than that of the deviated side in patients with type 2, 4, 6, and 7 deviations (Figure 1).
Demographic Data for Normal People and Patients With Septum Deviation.
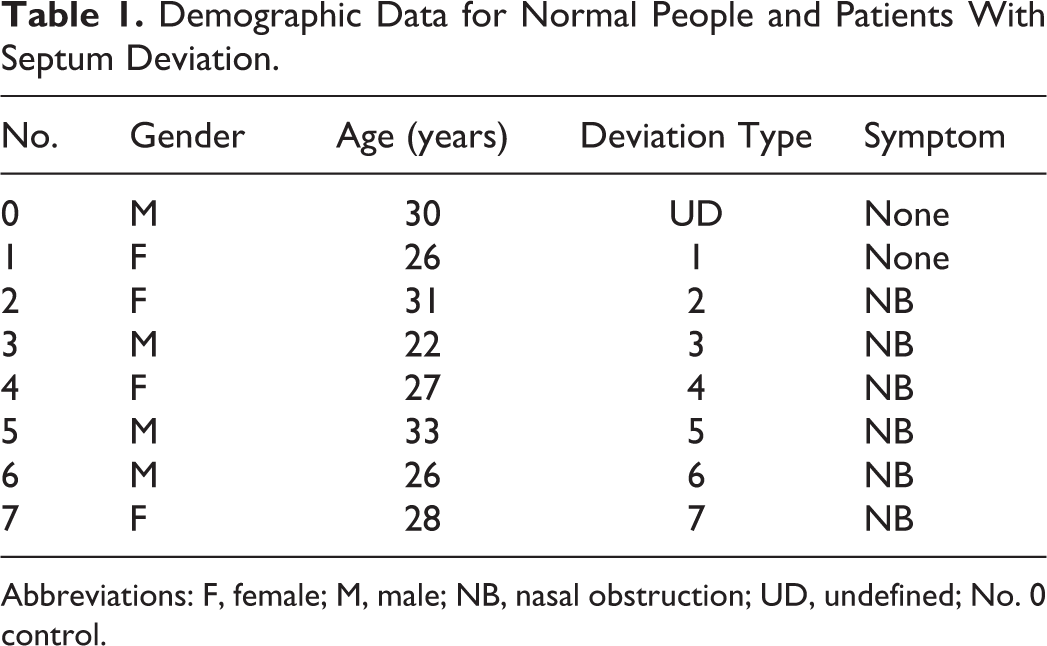
Abbreviations: F, female; M, male; NB, nasal obstruction; UD, undefined; No. 0 control.
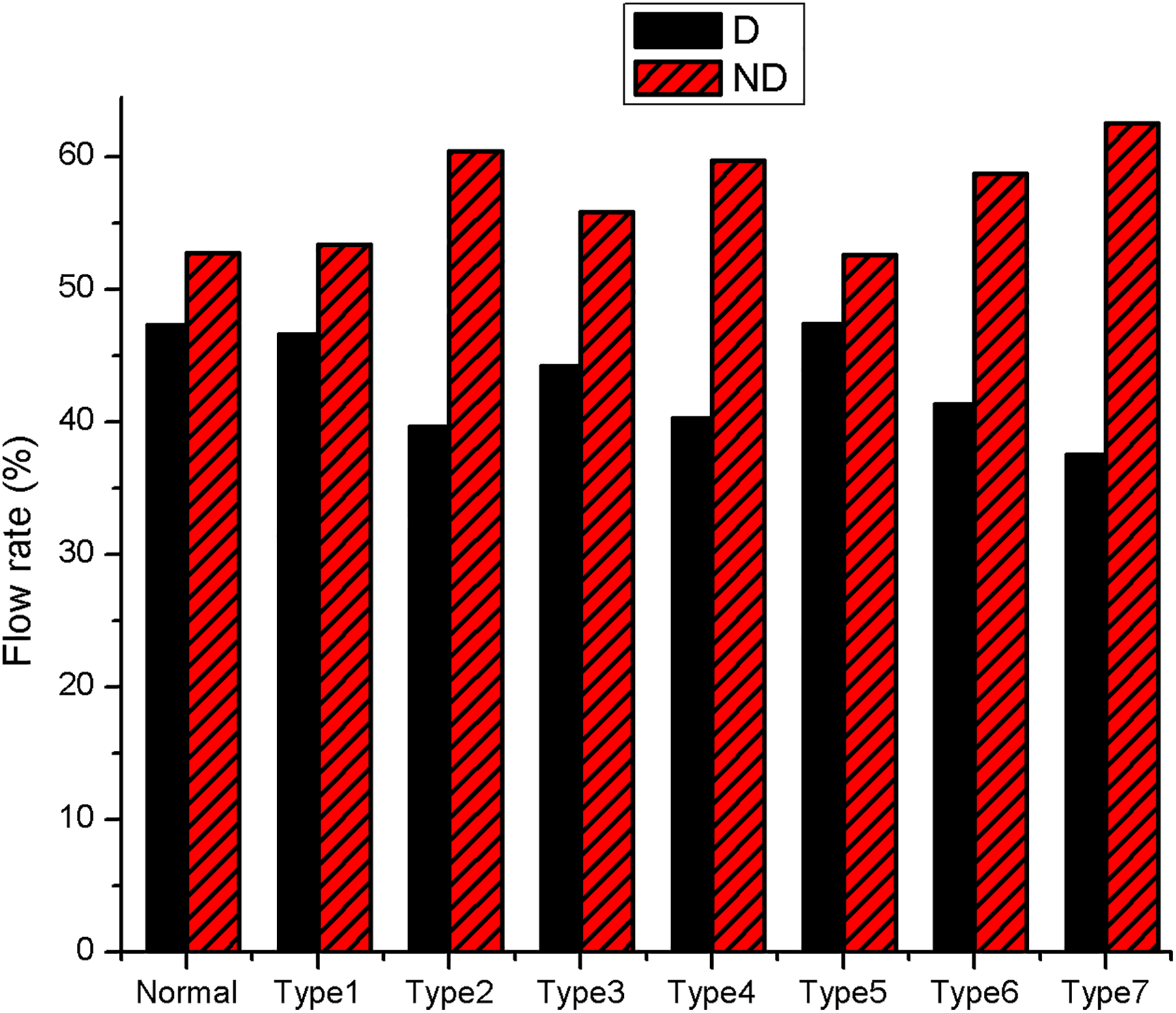
Computational fluid dynamics (CFD) simulation of flow partition in bilateral nasal cavities in control and patients with septal deviation. D indicates deviated side; ND, nondeviated side.
Next, we simulated the maximal velocity and total nasal resistance in each type of septal deviation. The maximal velocity and total nasal resistance in patients with type 4 (6.42 m/s) and type 7 (6.61 m/s) deviations were higher than that in other categories (type 1, 2, 3, 5, and 6), which were more similar to the control (3.72 m/s, Figure 2). The maximal velocity also correlated well with total nasal resistance in the simulations of patients with septal deviation.
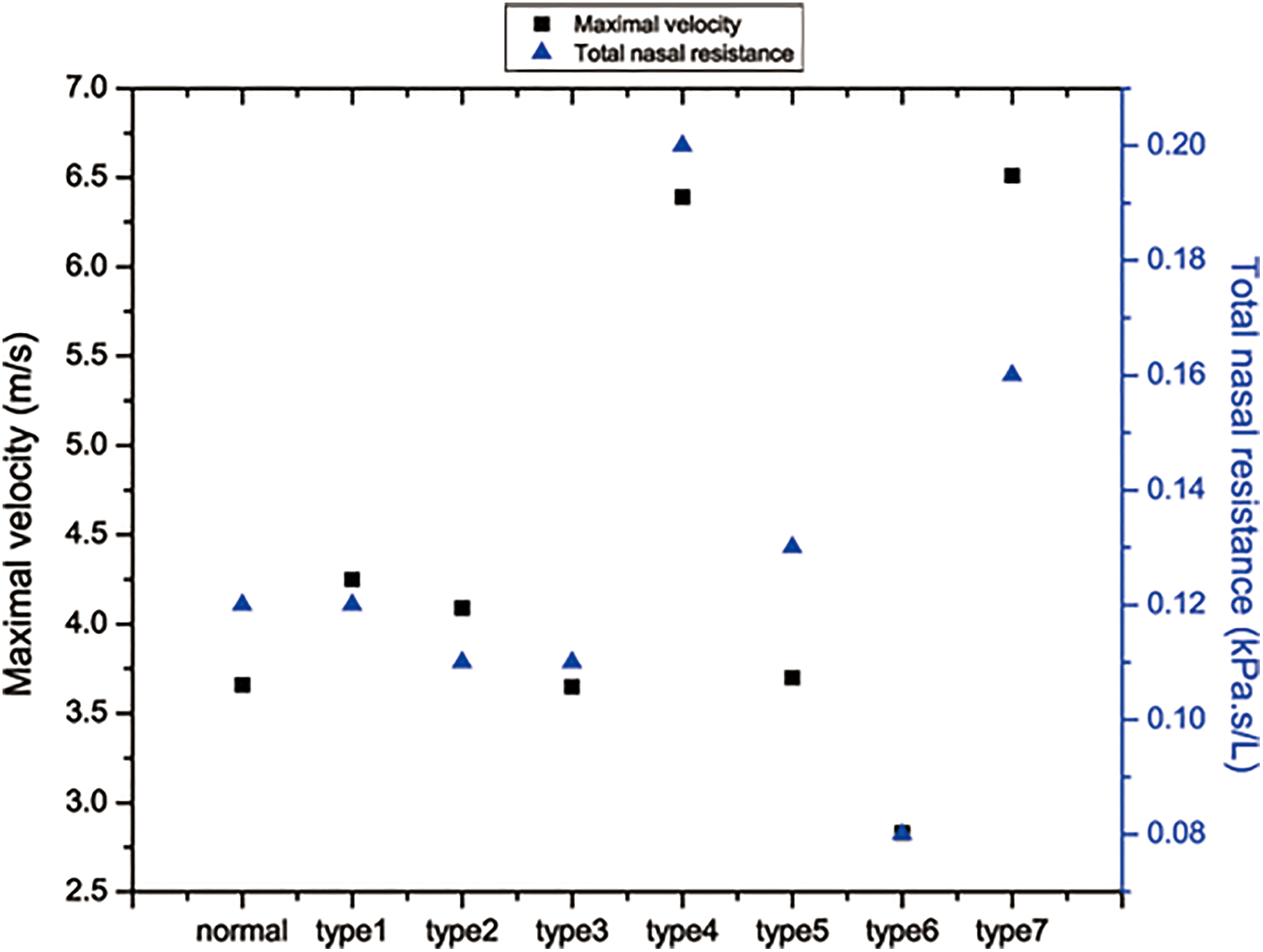
The value of maximal velocity (left y-axis) and total nasal resistance (right y-axis) in control and patients with septal deviation.
We then investigated the average velocity at coronal planes along the spectrum of the nasal cavity as described previously. 6 The highest average velocity was located at the nasal valve and gradually decreased when moving from anterior to posterior. In the anterior portion of the nasal cavity, the average velocity in type 2 (1.43 m/s), type 4 (1.66 m/s), and type 7 (2.48 m/s) deviations were higher than the control (1.24 m/s) or other septal deviation types (plane 1 in Figure 3). However, the difference was no longer observed at more posterior coronal planes.
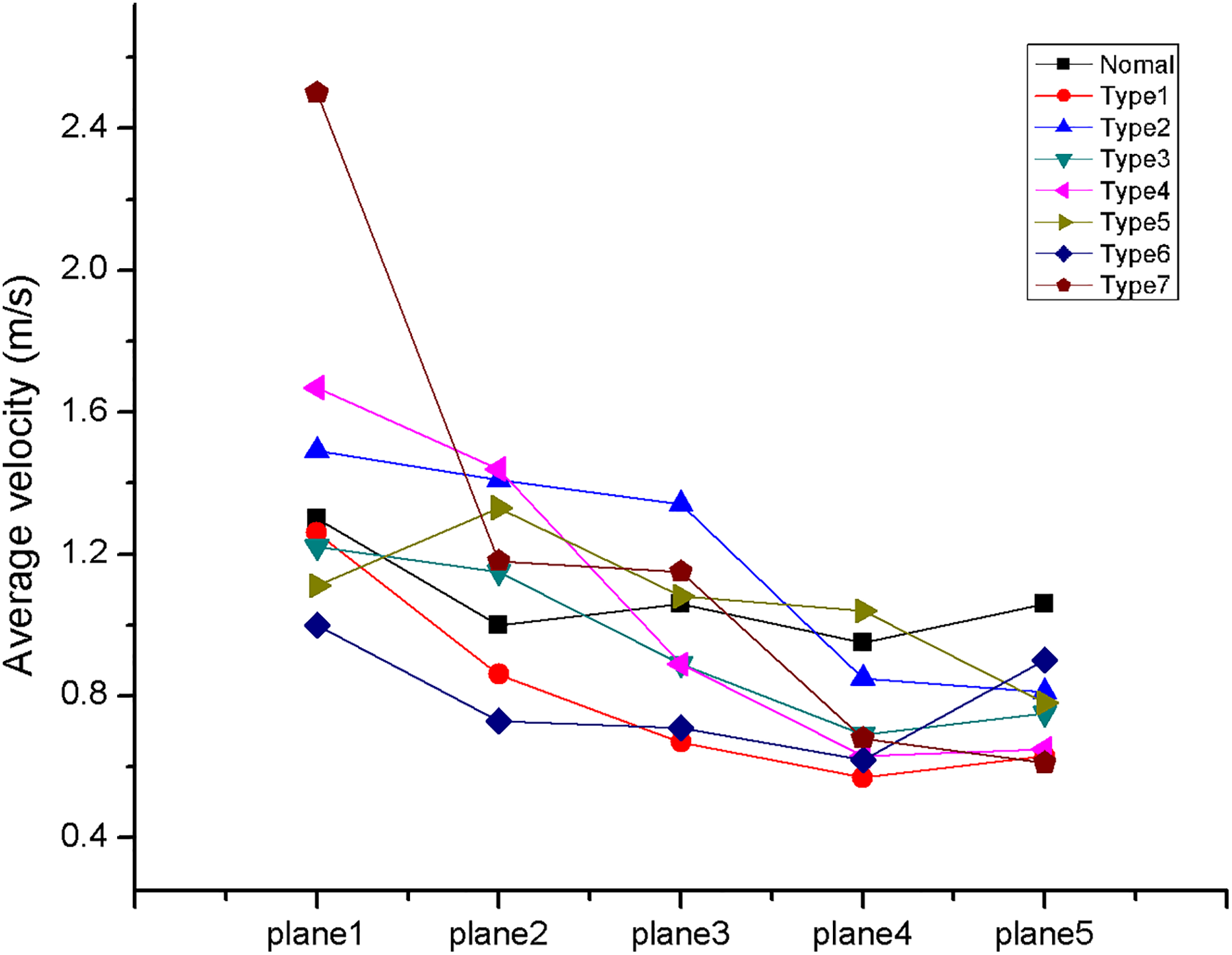
The average velocity in 5 coronal planes from anterior-to-posterior direction in control and patients with septal deviation. The vertical axis represents average velocity in the corresponding plane, and the horizontal axis represents locations.
The simulation of airflow velocity contours of normal control and patients with various NSD was then analyzed (Figure 4). Airflow velocity was found to be evenly distributed, and the maximal velocity was located at nasal valve area in the control (normal, arrow). The overall and peak velocity in the deviated side was higher than that in the contralateral side in all patients with septal deviations (Figure 4). One exception was at the anterior portion (type 4, arrows), there was another region with high velocity locating at midportion in the type 4 deviation (type 4, triangles). The relatively wide cavity without compensatory action of the inferior turbinate induced the formation of low velocity area (type 6 and 7, arrows), which corresponded to the “dead space” mentioned by Grutzenmacher et al. 15
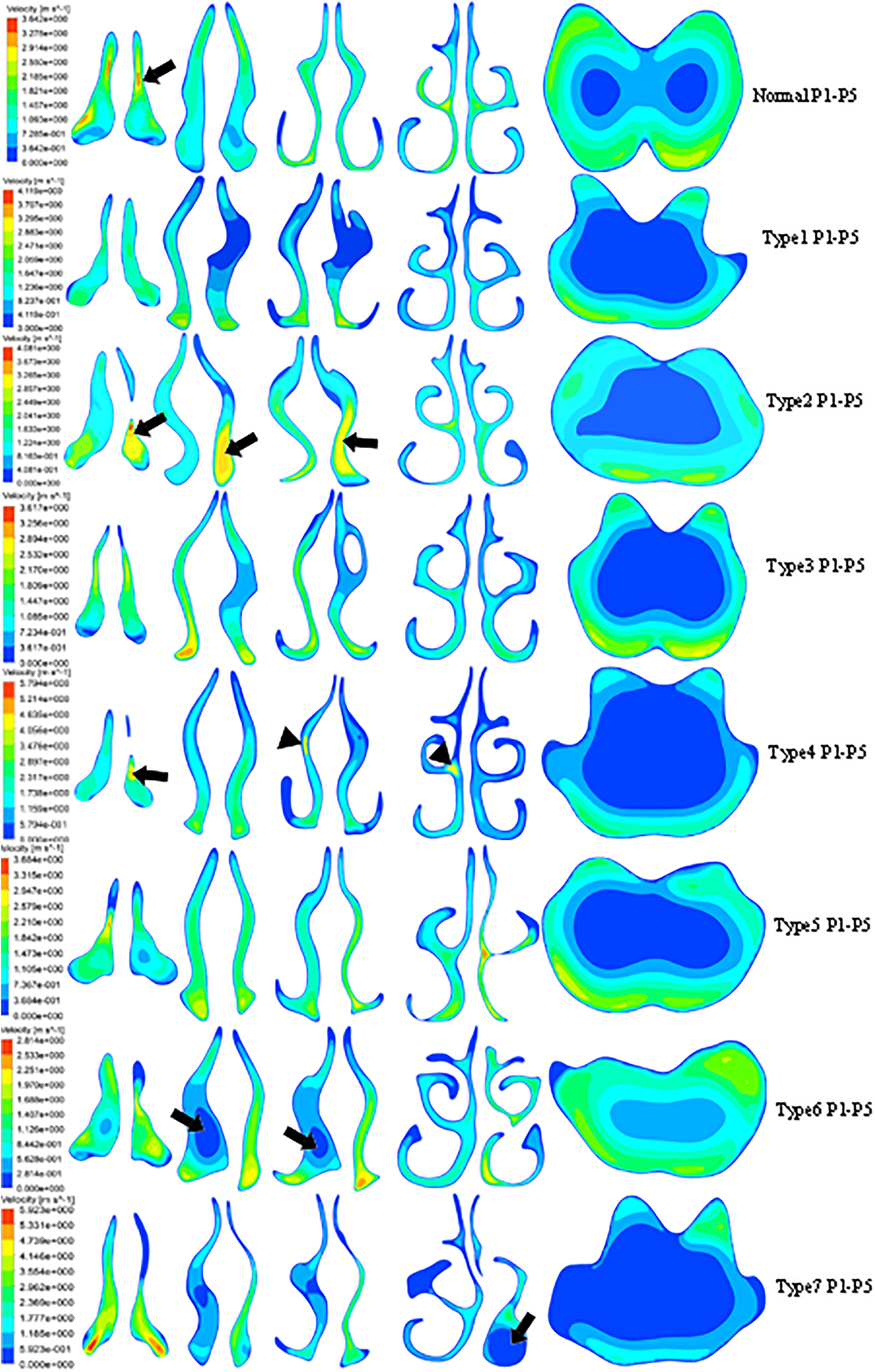
The velocity contours in normal people and patients with septal deviation. P1 to P5 represents plane 1 to plane 5. Arrow in normal people points at high velocity in nasal valve area, and arrows in type 2 and type 4 deviations point at high velocity area in deviated side. Triangles in type 4 deviation point at the high velocity area in nondeviated side. Arrows in type 6 and type 7 deviations point at low velocity area. Red represents the highest velocity, and blue represents the lowest velocity.
Next, we simulated and calculated the airflow temperature at each of the aforementioned coronal planes using CFD-Post (Figure 5). Overall, the average temperature in all participants was increased gradually from an anterior to posterior trajectory. From the midportion of the middle turbinate (plane 4) to the mid-nasopharynx (plane 5), however, the average temperature changed little (Figure 5). Little overall difference in average temperature between the control and patients with septal deviation could be detected.
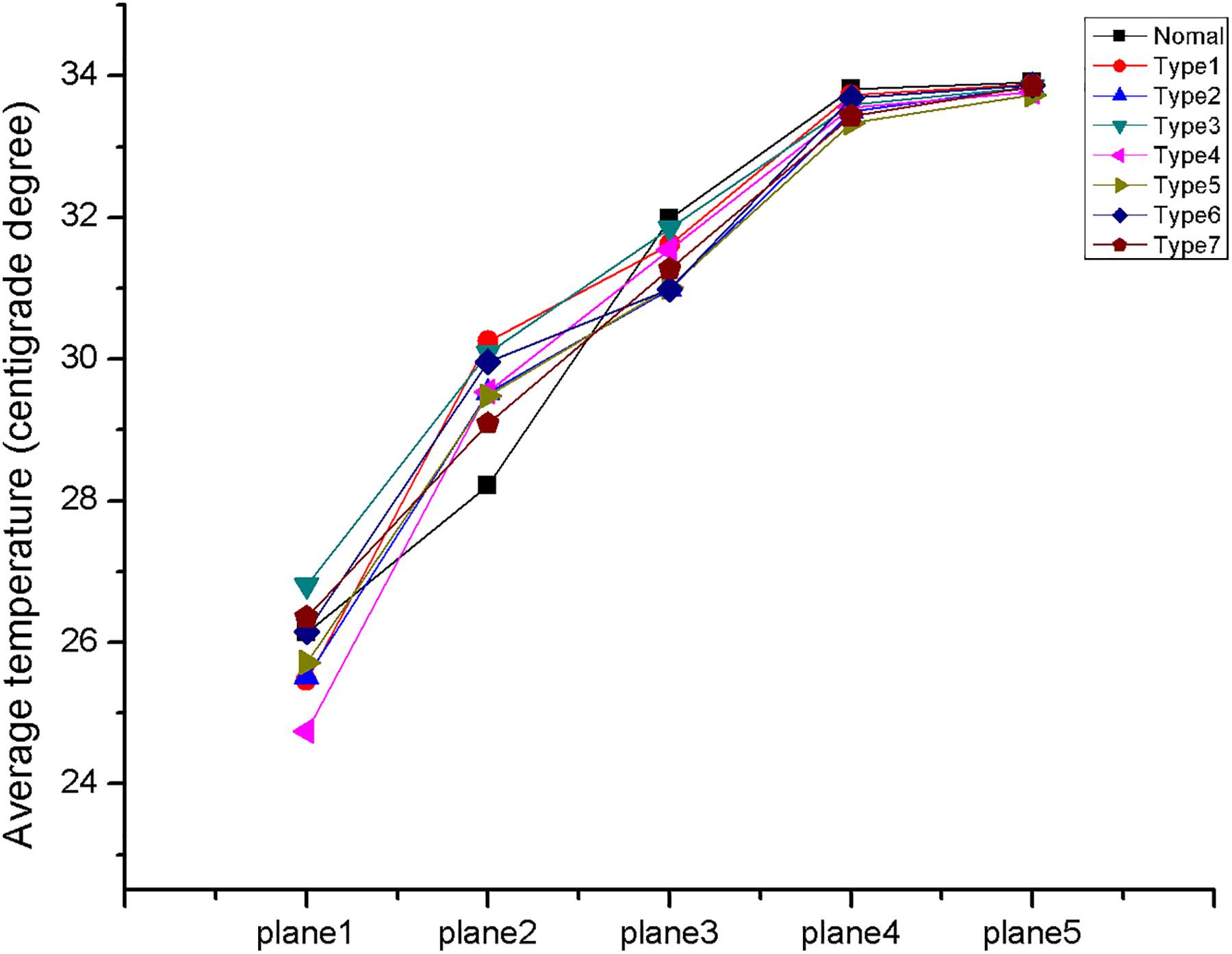
The average temperature in 5 coronal planes from anterior-to-posterior direction in normal people and patients with septal deviation. The vertical axis represents average temperature, and the horizontal axis represents locations.
The temperature contours in the control and patients with various septal deviations were then analyzed (Figure 6). In the control, airflow was fully warmed at the midportion of middle turbinate during inspiration (normal, plane 4). The same phenomenon occurred in patients with type 1, 3, 5, 6, and 7 deviations. Airflow temperature at midportion of middle turbinate in the deviated side of type 2 and type 4 deviations was slightly lower than that in the contralateral nostril (type 2 and type 4, arrows). Corresponding to the low velocity area in Figure 6, the airflow temperature in “dead space” was lower in the anterior portion (type 6, arrows) and higher in posterior portion of nasal cavity (type 7, arrow).
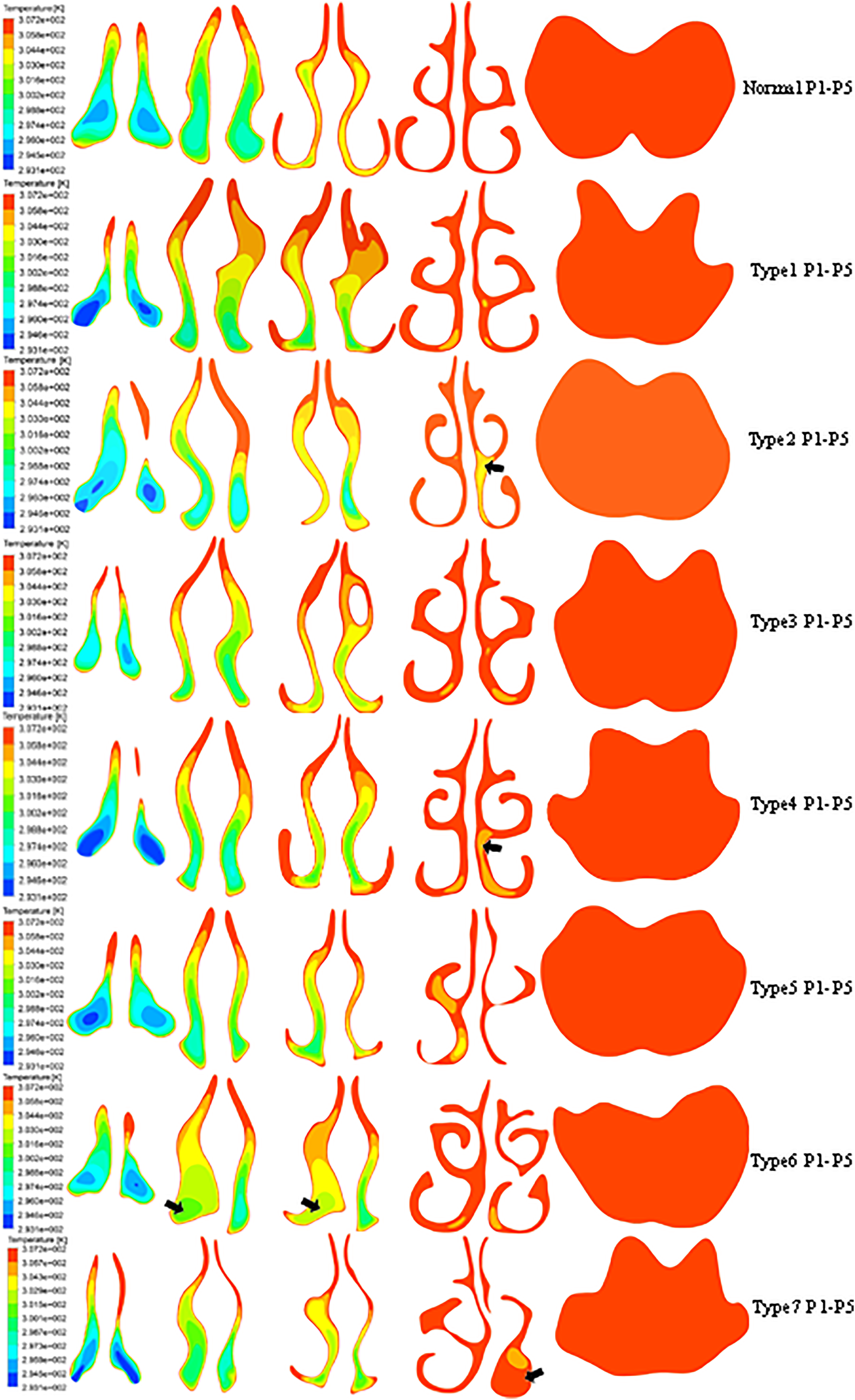
The temperature contours in normal people and patients with septal deviation. P1 to P5 represents plane 1 to plane 5. Arrows in type 2, type 4, and type 6 deviations point at low temperature regions. Arrow in type 7 points at high temperature area. Red represents the highest temperature, and blue represents the lowest temperature.
Discussion
Although the effect of NSD on airflow pattern has been previously assessed with method of CFD, just one single case with the most common type (“C” type) was selected for analysis. 7 Nasal septal deviations are highly variable, 9 and the extent of impact of each particular type of deflection on airflow pattern has not been well defined. In this study, investigation of the impact of NSD considering a particular deviation type on airflow pattern and warming function was assessed with CFD. 6,16 The CFD technique is powerful, as it allows one to perform a comprehensive analysis of the specific airflow characteristics on a particular point, plane, and volume in the nasal cavity, which might be difficult to acquire through the measurements of rhinomanometry and acoustic rhinometry. 17
Nasal septal deviation altered the symmetry of the nasal cavity, which may induce airflow redistribution. 18 Chen et al demonstrated that flow partition was 38.6% and 61.4% in deviated side and nondeviated side, respectively, in patients with septal deviation. 7 In the study presented here, the relative balance of flow partition was redistributed in type 2, 4, 6, and 7 deviations. In type 1, 3, and 5 deviations, however, the airflow redistribution was unchanged. Moreover, the decreased flow rate in the deviated side of type 2 and type 4 also highlights the importance of nasal valve in airflow regulation. Therefore, the assessment of the impact of NSD on airflow distribution may be dependent on the specific deviation type.
The airflow velocity is another index to assess the airflow characteristics, and the relatively rapid airflow velocity induced by a narrow cavity might contribute to the sense alteration of nasal airflow. 6,19,20 In this study, we detected that the difference in airflow velocity between bilateral nostrils was particularly obvious in type 2, 4, 6, and 7 deviations. However, no obvious alterations could be detected in type 1, 3, and 5 deviations. Moreover, the local airflow characteristics were also altered, which was manifested as the overall airflow velocity in the deviated side and was higher than that in nondeviated side.
The sense of nasal obstruction is impacted by multiple factors, 21 such as mechanical obstruction, innervation, and inflammatory status, 22 and the total nasal resistance is just one factor contributing to nasal obstruction. Chen et al demonstrated that total nasal resistance in the patient with NSD was almost twice of that of the healthy participant. 7 The same phenomenon was detected in type 4 and type 7 deviations in our study, and other types of septal deviation had the similar value of total nasal resistance compared to the normal control. Therefore, the impact of septal deviation with type 1, 2, 3, 5, and 6 on total nasal resistance deserves further evaluation.
Lindemann et al demonstrated that the anterior portion of nasal cavity was important for heating, and structural alteration in this section would impair the warming function of the nasal cavity. 14 The reduced airflow temperature in the deviated side of type 2 and type 4 deviations in this study might correlate with the decreased nasal valve angle and limited flow distribution. Moreover, the low temperature in the anterior “dead space” in type 6 deviation and high temperature in posterior “dead space” in type 7 deviation also highlighted the importance of the anterior portion of nasal cavity in warming function. Although local difference in airflow temperature existed in all categories of NSD, the overall warming function was ultimately similar in all settings. The disturbed airflow pattern and the narrowed nasal cavity in patients with septal deviation strengthened the contact between the airflow and nasal mucosa 16 ; however, its impact on warming function of the nasal cavity was little in our study.
There are several limitations to this study. First, the impact of NSD considering the degree of deflection on nasal airflow and warming function was not included in this study. Moreover, the sample size on each category of NSD was small for analysis, and future studies with increased sample size or investigation toward a specific deflection type (2, 4, 6, 7) may demonstrate the most substantial difference. Additionally, as the studies presented here were computational in nature, additional studies are required to assess the applicability of these results in vivo.
In conclusion, the variation in septal deviation types may contribute to altered airflow pattern from a CFD approach. However, warming function was little altered between septal deviation types. Future studies will help to ascertain the functional importance of septal deviation types and the applicability of these computational studies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.