
Abstract
A 2-month-old male with a prior diagnosis of laryngomalacia (LM) presented to the emergency department in respiratory distress with worsening inspiratory stridor, suprasternal retractions, and a dry cough. A chest X-ray and lateral neck radiograph were performed and demonstrated no abnormalities. Flexible laryngoscopy revealed the same, previously observed moderately prolapsed arytenoids and an omega-shaped epiglottis with shortened aryepiglottic (AE) folds. He also had a right lower neck mass. He was scheduled for a direct laryngoscopy and bronchoscopy (DLB) and supraglottoplasty. During the DLB, LM (Figure 1A) and anterior compression of the midtrachea (Figure 1B) was noted. Lysis of the AE folds was performed in cold-steel fashion, and the infant was then taken for further imaging.
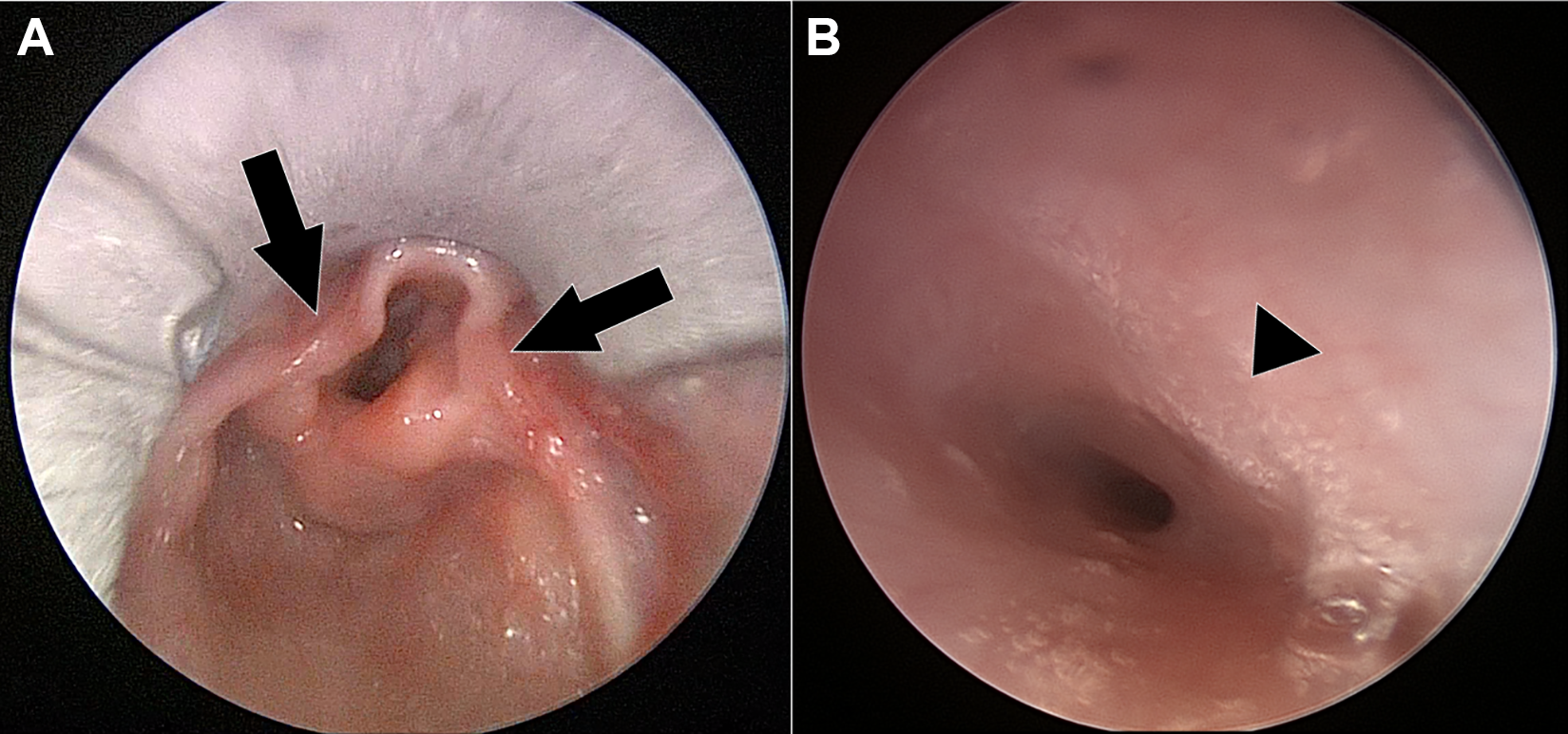
Intraoperative DLB photographs demonstrating (A) shortened aryepiglottic folds (black arrows) and (B) anterior tracheal wall compression (black arrowhead). DLB indicates direct laryngoscopy and bronchoscopy.
Computed tomography angiography of the chest demonstrated a 2.6 × 5.1 cm heterogenous anterior mediastinal soft tissue mass contiguous with the thymus. The mass contained calcifications and there was incompletely evaluated cervical extension. Magnetic resonance imaging of the neck and chest demonstrated a right-sided complex solid and cystic mass at the base of the neck (likely arising from the thymus) crossing midline and projecting posteroinferiorly posterior to the manubrium, measuring 4.4 cm × 2.3 cm × 4.0 cm (Figure 2A-C). The mass caused a leftward posterior mass effect on the trachea and right thyroid lobe; it contained cystic lesions as well as fat complements. No major vessels were seen supplying the mass.
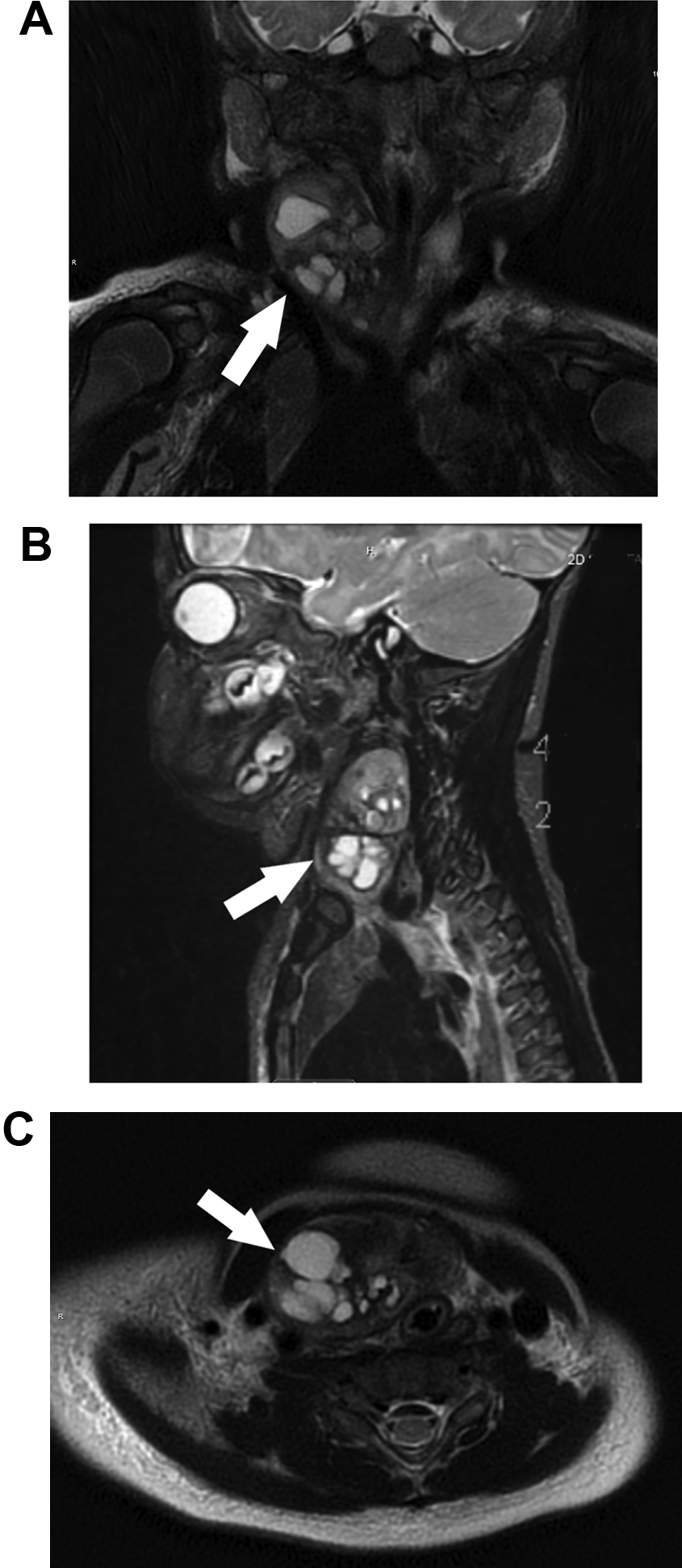
Magnetic resonance imaging (MRI) of the neck/chest with contrast (T2 weighted) demonstrating right lower neck mass with cystic and solid components, substernal extension, and resultant mass effect (white arrow). (A) Coronal section, (B) sagittal section, and (C) axial section.
The patient was taken for excisional biopsy. This revealed a large heterogeneous mass located in level IV of the neck with partial substernal and subclavicular extension. Clean planes of dissection were noted, and the mass was able to be easily excised. The patient was extubated on the first postoperative day and weaned to room air with no further stridor noted. Pathologic analysis demonstrated areas of varying differentiation derived from multiple germ cell layers including squamous epithelium, ciliated columnar epithelium-lined cysts, intestinal mucosa, brain tissue, cartilage, thyroid and thymic tissue, all consistent with a mature teratoma. The mass measured 5.2 cm × 3.5 cm × 2.1 cm.
The most common sites of teratomas are the sacrococcygeal region followed by the mediastinum, while head and neck (cervical) teratomas comprise 2% to 9% of all teratomas. 1 Cervical teratomas can cause compression distally into the mediastinum or displace the trachea and even result in pulmonary hypoplasia. 1 Although 95% of all teratomas are benign, the cervical teratoma, if not properly treated, has resulted in death in 80% of cases due to obstructive respiratory distress. 2
Laryngomalacia is the most common cause of inspiratory stridor in infants. The prevalence of coincidental secondary airway lesions (SALs) has been reported to be 7.5% when excluding patients with conditions known to be associated with airway anomalies and 10% without excluding those patients. 3 The most common SALs include subglottic stenosis, tracheomalacia, bronchomalacia, and vocal fold paralysis. No reports could be found on the incidence of teratomas in patients with LM. This prevalence of SALs results in a debate for advocating full airway endoscopy for all patients with LM or restricting this to only severe cases.
The case presented herein represents a patient who was diagnosed with LM, yet was found to have a second, more insidious cause for inspiratory stridor. Cervical teratomas rarely extend into the mediastinum and it is even more rare for this extension to present with stridor. The practicing otolaryngologist must always be mindful of an SAL as a cause for stridor in patients with LM. Considering the relatively uncommon prevalence of SALs, and the scarcity of SALs requiring surgical management, the practice of a full endoscopic airway evaluation in patients with LM should be advocated for cases that present atypically.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.