
Abstract
The main aim of our study is to evaluate whether the effect of smoking on the auditory system shows gender differences. Another aim is to evaluate whether smoking has any influence on the absorbance of sound. There were 236 volunteers including 90 nonsmokers (42 females and 48 males) and 146 smokers (72 females and 74 males) in the study. Smokers were grouped according to pack-years of smoking as 5 to 10 pack-years, 11 to 20 pack-years, and more than 20 pack-years. Pure tone audiometry and wideband tympanometry were performed in all individuals. Both female and male smokers who consume more than 20 pack-years had significantly higher hearing thresholds at 4 and 6 kHz and significantly lower sound energy absorbance rates at 4, 6, and 8 kHz. Moreover, female smokers with a consumption of 11 to 20 pack-years had significantly higher hearing thresholds at 6 kHz and significantly lower sound energy absorbance rates at 6 and 8 kHz. Smoking causes hearing loss at high frequencies in both females and males, especially in a dose-dependent manner affecting individuals with a consumption of more than 20 pack-years. The sound energy absorbance is significantly reduced at 4, 6, and 8 kHz. In addition, these effects may occur in women with even less exposure.
Introduction
Smoking can affect the auditory system by direct and indirect ways. It directly causes damage on the hair cells by increasing reactive and free oxygen radicals. Indirectly, it increases the ratio of carboxyhemoglobin and affects the perfusion of the auditory system. This situation reveals as sensorineural hearing loss at high frequencies. 1 Provided that the risk of exposure to professional noise and age-related hearing loss are excluded, the probability of hearing loss development is 1.69 times higher in smokers than in nonsmokers. 2 In addition, there are both laboratory and clinical studies showing that smoking has harmful effects not only on the middle ear but also on the eustachian tube. Animal studies revealed that smoking caused histopathological changes in the middle ear and the eustachian tube; similarly clinical studies demonstrated increased frequency of otitis media. 3 –6
There are several clinical studies evaluating the effects of smoking on inner and middle ear with pure tone audiometry (PTA), 226 Hz probe tone tympanometry, and otoacoustic emission (OAE). 7 –9 The acoustic absorbance measurement is sensitive to minor changes in both the middle and the inner ear, which enables evaluation of 2 systems together. Acoustic absorbance data can be measured easily through a wide frequency range (0.25-8.0 kHz) with wideband tympanometry (WBT). Thus, the transfer function of the sound to the inner ear and the ability to be absorbed by the inner ear may be evaluated mutually. Absorption and back reflection of the delivered energy both at ambient pressure and various pressures generated by the probe may be measured. Absorbance of energy is called absorption, and back reflection is called reflectance. The sum of these 2 values is equal to 1. In normal functioning ears, wideband absorption has the highest value in the range of 1.0 to 4.0 kHz, which are the frequencies the middle ear absorbs the sound energy. 10,11
To the best of our knowledge, there are no studies evaluating the effect of smoking on the absorbance of the sound. Previous studies evaluating the influence of smoking on the auditory system evaluated only male participants. 1,7,8,12,13 Therefore, the main aim of our study is to evaluate whether the effect of smoking on the auditory system shows gender differences. Another aim is to evaluate whether smoking has any influence on absorbance of sound.
Patients and Methods
Local ethical committee approved this study (protocol no: 2018/100). This prospective study was conducted in the department of ear, nose, and throat diseases of our tertiary care hospital.
Patients
We randomly selected volunteers aged 20 to 50 years. Patients older than 50 years were not included to exclude age-related high-frequency hearing loss. 14 Initially, patients were questioned about their stories related to the ear and hearing. None of the patients included in our study had a history of otologic surgery and trauma, noise exposure, ototoxicity, and familial hearing loss. We also excluded patients with tinnitus or hearing loss due to any drug use or noise exposure. The external ear canal and tympanic membranes were normal in their otoendoscopic examination. First of all, auditory evaluation of all the participants was performed using PTA, and hearing thresholds were recorded. The demographic data (age and gender) of the patients, smoking status, and number of cigarettes per day were recorded. Taking into account that a package consists of 20 cigarettes, pack-years calculation was made for all the patients according to the total years of smoking. Individuals who had less than 5 pack-years of smoking history and who had previously smoked were excluded from the study. The auditory data (PTA and WBT) of the right ears of the individuals were used in analysis. While nonsmokers were divided into men and women only, smokers were grouped according to gender and duration of smoking (Table 1).
Age and Smoking Data of Groups According to Gender, Smoking Status, and Pack-Years Smoking.
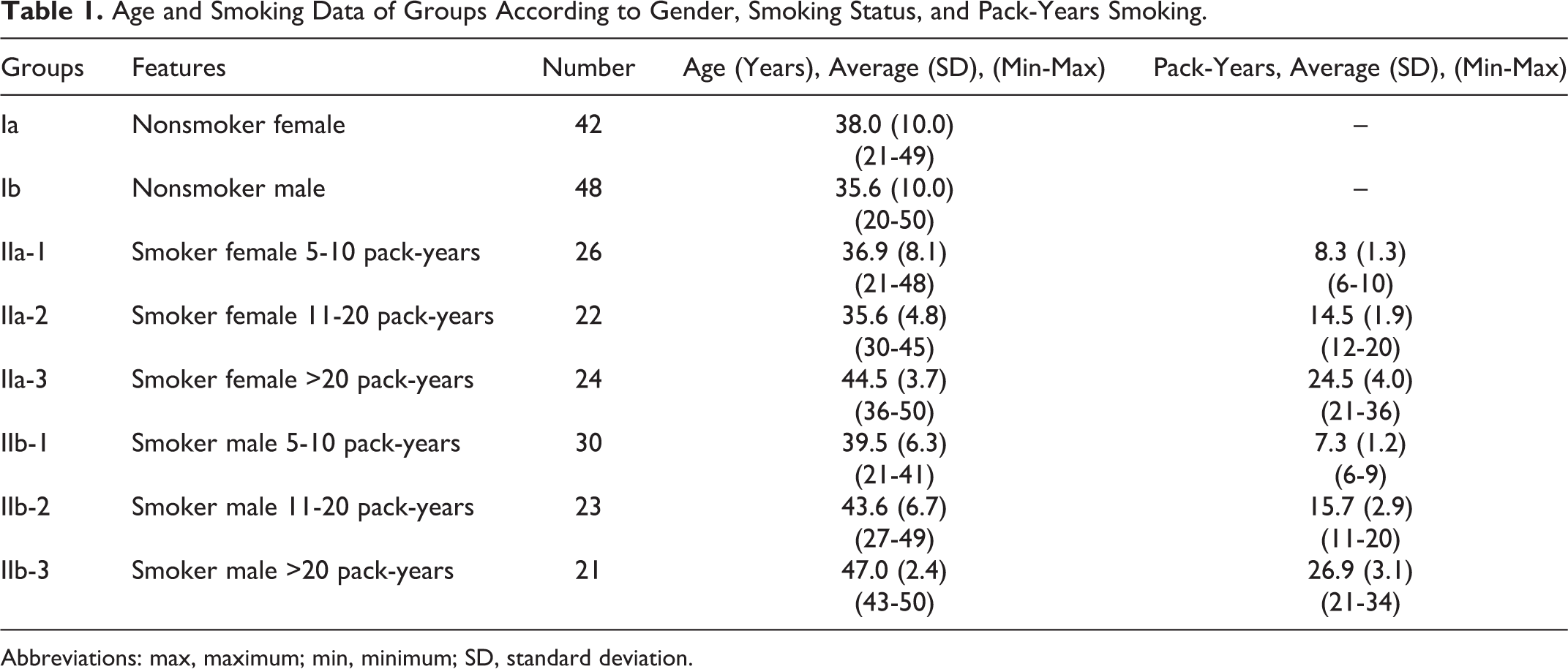
Abbreviations: max, maximum; min, minimum; SD, standard deviation.
Hearing Evaluation
Pure tone audiometry test was performed with an AC40 (Interacoustics, Assens, Denmark) device in a soundproof room. Air conduction thresholds were measured with the Telephonics TDH39 headset at the 0.25 to 6.0 kHz range. Bone conduction thresholds were measured with a B71 bone vibrator at the 0.25 to 6.0 kHz range. The thresholds obtained were recorded separately at 0.5, 1, 2, 4, and 6 kHz. Patients with conductive type hearing loss were excluded from the study.
Wideband Tympanometric Evaluation
Wideband tympanometry was evaluated with Titan Suite device (Interacoustics). Measurements were performed at 0 pressure (daPa) and using a 90 ± 3 dB sound stimulus. Wideband absorbance values were measured in the frequency range of 0.25 to 8.0 kHz at ambient pressure. Absorbance rates at ambient pressure range from 0 to 1. The higher the amount absorbed by the middle ear, the closer it is to value 1. These values between 0 and 1, that is, the absorbance rate, can be evaluated as percentage. To calculate the data, OtoAccess 1.2.1 software (Interacoustics) was used. The first 2 digits after 0 provide the percentage value of the sound energy absorbed by the middle ear.
Statistical Analysis
Statistical analysis was performed using Statistical Package for Social Sciences version 20.0 (SPSS Inc, Chicago, Illinois). Data of the groups were compared using 1-way analysis of variance at each frequency for both WBT and PTA. Statistical significance was considered P < .05.
Results
There were 236 volunteers participating in the study. While nonsmokers were grouped as men and women, smokers were stratified according to gender and duration of smoking. Age and smoking data of groups according to gender, smoking status, and intensity are presented in Table 1.
Hearing thresholds obtained at 5 different frequencies in PTA were evaluated. There was no difference between the groups at 0.5, 1, and 2 kHz (P > .05). However, significant differences existed at 4 and 6 kHz (P < .05). The hearing thresholds of group IIa-3 and group IIb-3 at 4 kHz were significantly higher than the other groups. At 6 kHz, the hearing thresholds of group IIa-2, group IIa-3, and group IIb-3 were significantly higher than the other groups. The hearing thresholds of these groups at both frequencies were statistically significant compared to the other subgroups (Table 2).
Mean PTA Hearing Thresholds of the Groups at 5 Different Frequencies.a
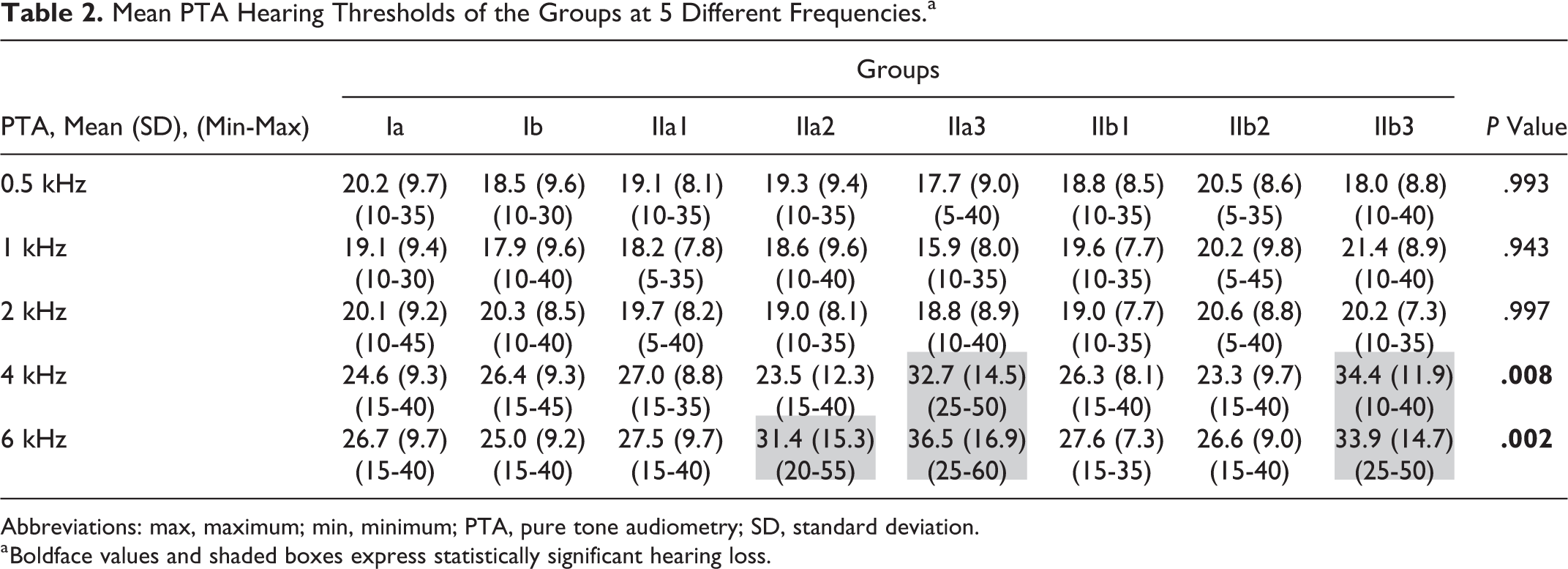
Abbreviations: max, maximum; min, minimum; PTA, pure tone audiometry; SD, standard deviation.
a Boldface values and shaded boxes express statistically significant hearing loss.
Frequency-specific absorbance values at ambient pressure were evaluated at 10 different frequencies (0.25, 0.5, 0.75, 1, 1.5, 2, 3, 4, 6, and 8 kHz; Figure 1). The absorbance peaked at 3 kHz in all groups. The data were not significantly different between the groups under 4 kHz as in the PTA (P < .05). However, there was a significant difference at 4, 6, and 8 kHz (P < .05). The absorbance rates of group IIa-3 and group IIb-3 were significantly lower at 4 kHz. At 6 and 8 kHz, the absorbance rates of group IIa-2, group IIa-3, and group IIb-3 were significantly lower. The absorbance of these groups at the 3 frequencies was statistically significant compared to the other groups (Table 3).
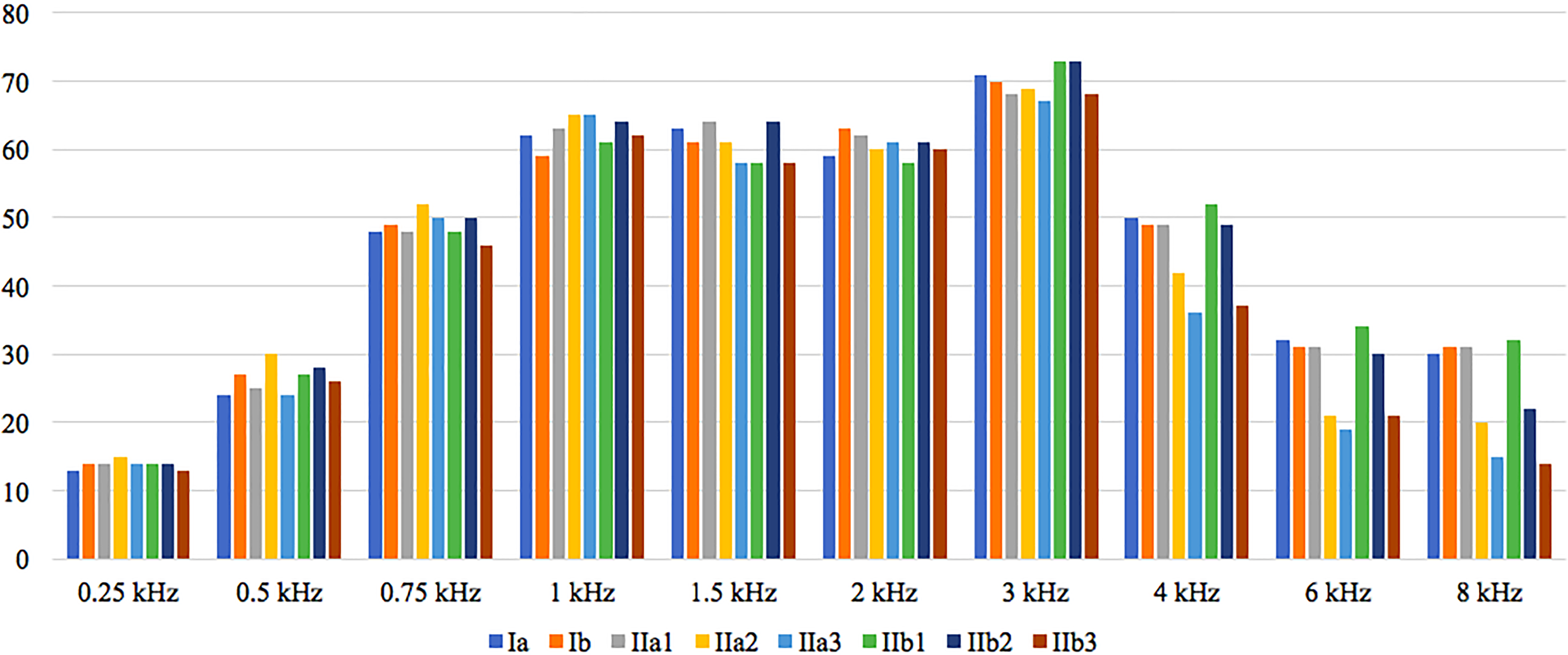
Frequency-specific absorbance values (%) at ambient pressure.
Absorbance Values of the Groups Obtained at 10 Different Frequencies in Wideband Tympanometry.a
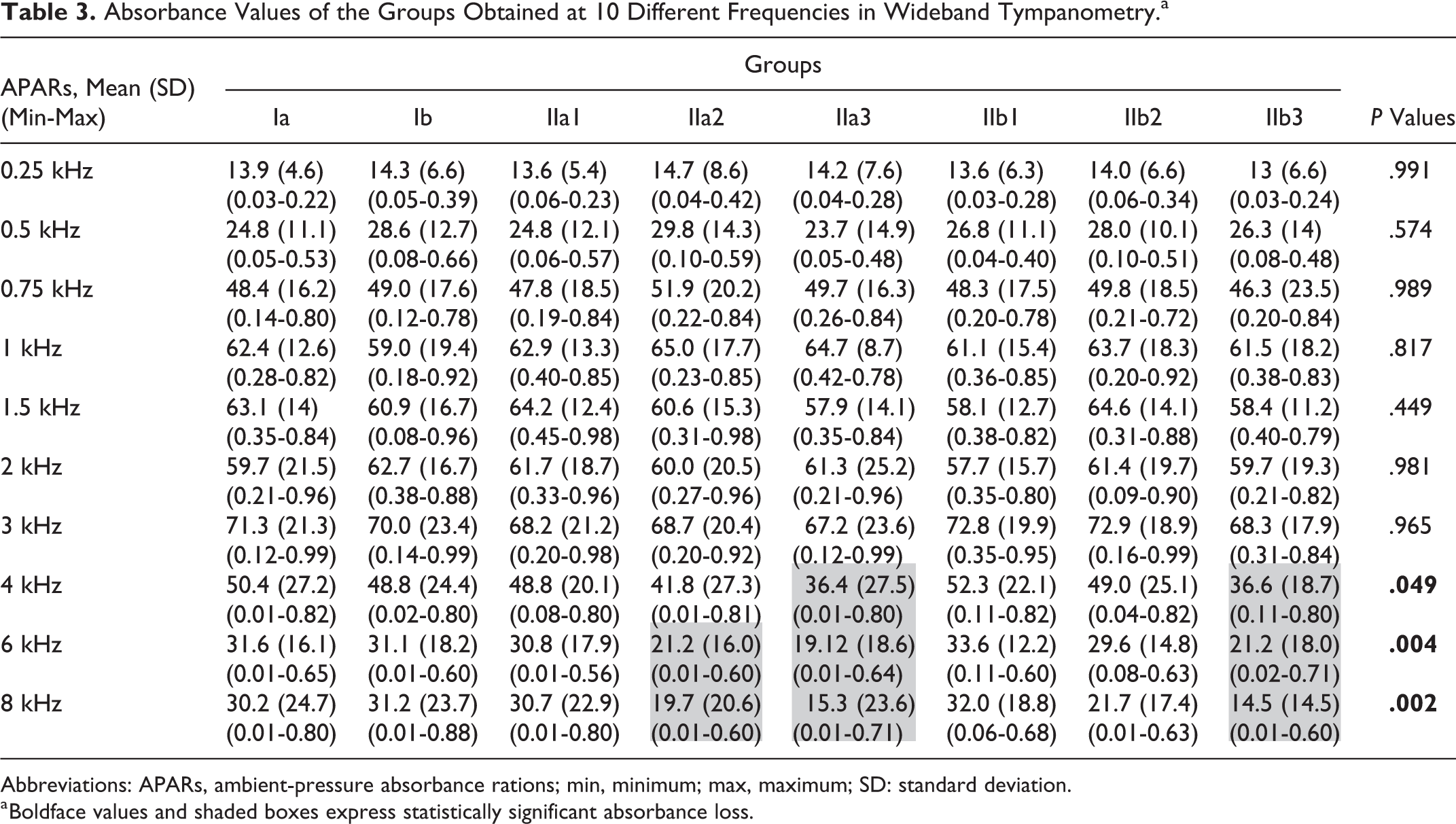
Abbreviations: APARs, ambient-pressure absorbance rations; min, minimum; max, maximum; SD: standard deviation.
a Boldface values and shaded boxes express statistically significant absorbance loss.
Discussion
Today, smoking is one of the most common addictions. Smoking affects individuals in many ways through damaging many systems. It causes hearing loss due to the toxic effect of heavy metals on the hair cells and nerves in the auditory pathway. 8 The effects of smoking on hearing have been evaluated for several years with various tests. Generally, the influence of smoking on the auditory system has been associated with prolonged and/or intense exposure. Pezzoli et al showed that smoking caused hearing loss at high frequencies. In addition, tympanometric tests revealed tubal dysfunction in smokers. 7 Chang et al evaluated the effects of smoking on hearing with PTA. They stated that both active and passive smoking caused hearing loss at high frequencies due to prolonged exposure, especially more visible after 40 years of age. 9 Uchida et al showed that smoking habits cause hearing disorders at high frequencies (4 kHz), which increased dose dependently. 15 Similarly, Noorhassim and Rampal reported smoking caused hearing loss especially at high frequencies in a dose-dependent manner. There was a significant increase in hearing impairment, especially with more than 20 pack-years of use. 12 Similar to these studies, the harmful effects of smoking on the hearing system increase in a dose-dependent manner in our study. In both men and women with cigarette consumption of more than 20 pack-years, hearing thresholds increased in PTA at high frequencies (≥4 kHz), and the absorbance at WBT decreased significantly. In addition, no effect of 11 to 20 pack-years of cigarette use (averaging 15 pack-years) was observed in men, while in women it was associated with harmful effects.
Vinay showed that less than 5 pack-years of cigarette consumption was associated with decreased amplitudes of transient evoked OAEs even if the hearing of individuals was not affected. In other words, it was found that outer hair cells were damaged in the early stage due to smoking. 13 We did not include individuals with cigarette consumption of less than 5 pack-years. In addition, we could not document any effect in women and men with less than 10 pack-years of consumption.
There are several clinical and laboratory studies showing the influence of smoking on middle ear. Months of exposure to cigarette smoke in rats has been shown to cause squamous metaplasia, goblet cell aplasia, and silica loss in the eustachian tube and middle ear mucosa. 3 In addition, cigarette smoke induces tumor necrosis-α production and causes severe inflammation in the middle ear mucosa. 6 Cigarette smoke, with its both toxic and irritant actions, has been shown to have effects that increase negative pressure such as ear fluid accumulation and mucosal hypertrophy in the middle ear. 16 Clinical studies evaluated the effects of smoking on the middle ear mucosa and eustachian tube by investigating the relationship between smoking and otitis media. This evaluation is generally made in children due to passive smoking. In combination with impaired mucociliary clearance, prolonged exposure to cigarette smoke (longer than 6 months) caused prominent mucosal secretion in the eustachian tube and middle ear, which increased the frequency of otitis media. 4,5,17
Although the effect of smoking on the middle ear was evaluated at microscopic level in laboratory studies, and in relation to otitis media in clinical studies, the anatomical and functional changes of the middle ear were not evaluated with any test previously. Wideband absorbance provides important information about the functional and anatomical structure of the middle ear. To our knowledge, there are no data in the literature regarding the influence of smoking on the acoustic absorbance of the auditory system. Only Pucci et al evaluated the acoustic absorbance in newborns of mothers exposed to tobacco smoke during pregnancy and did not find any difference in newborns whose mothers were exposed and not exposed to tobacco smoke. 18 We included adult patients and took the exposure levels into account. Although we did not document any impairment in patients with short-term use, we observed a decrease in absorbance rates at higher frequencies due to long-term smoking exposure, which started earlier in women. Either internal ear hair cell damage due to chronic exposure or the pressure changes in the middle ear and mucosal hypertrophy may cause this pathology. We may speculate that absorbance loss in higher frequencies may be associated with either earlier age-related hearing loss or decreased discrimination ability due to disruption of distinguishing high-frequency words.
Wideband tympanometry measurements are more popular in the diagnosis and follow-up of both middle and inner ear diseases. Cigarette smoking should be questioned during evaluation of results because overlooking smoking may lead to ignoring the consequences of smoking and misinterpretation of the data.
The limitation of our study may be that OAEs are not preferred as a separate test in evaluation of hearing. With this test, hair cell damage may be more clearly demonstrated. Furthermore, passive smoking can be considered as a separate category by further studies.
Conclusion
Smoking causes hearing loss in high frequencies dose dependently in both men and women, especially in individuals with a consumption of more than 20 pack-years. At 4, 6, and 8 kHz, the acoustic absorbance is significantly reduced. In addition, these effects may occur in women with even less exposure. Although the average use of 15 pack-years does not change the auditory tests in men, it causes a significant decrease in absorption rate and increase hearing loss at high frequencies in women.
Footnotes
Acknowledgments
The authors thank Prof M. E. Durakoğlugil for his contribution.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.