
Abstract
In this study, we evaluated the cochlea, medial olivocochlear system, and brainstem function in autistic children using evoked otoacoustic emissions (OAEs) and a noninvasive contralateral suppression (CLS) test. In total, we included 21 autistic children with normal hearing (study group) and 11 healthy children (control group). Transient-evoked OAEs (TEOAEs) and CLS of TEOAE were evaluated in the left and right ears of all patients. In a silent room, spontaneous, transient, and dP ILO292 were evaluated. The mean age of the study and control group was 9.1 years (range: 6-13 and 6-12 years, respectively). For the study group, there was no statistically significant difference between the OAE and CLS values of the right ear (P > .05). However, for the left ears, OAE values were statistically significantly higher than the CLS values (P < .05). In the control group, the OAE values of both ears were statistically significantly higher than the CLS values (P < .05). In autistic children with normal hearing, the medial olivocochlear system functions more effectively in the right ear than the left ear. Asymmetry between the ears is likely responsible for the peripheral auditory lateralization and independence in auditory function between the left and right ears.
Introduction
Fibers of the medial olivocochlear system (MOS) consist of myelinated neurons. These fibers begin at the medial nucleus of the contralateral superior olivary complex and join the vestibular nerve root at the base of the fourth ventricle, synapsing with the outer hair cells of the organ of Corti.1,2 It was reported that the MOS efferents alter the dynamics of hearing, protect from acoustic trauma, and aid in selective attention.3,4 Studies involving animal models have shown the protective effects of MOS efferents against high sounds. 5 Activation of the MOS fibers that synapse on the outer hair cells of the organ of Corti reduces damage caused by high sounds by protecting the basilar membrane. 6 To evaluate the effect of the MOS on cochlear amplification, total otoacoustic emissions (OAEs) were measured. An OAE is a low-level sound emitted by the cochlea either spontaneously or evoked by an auditory stimulus.3,7
Autism is a neurodevelopmental syndrome associated with impaired social interaction, verbal and nonverbal communication, as well as restricted and repetitive behavior, as defined by the 1994 American Psychiatric Association criteria. In addition, autistic children can have abnormal hearing, ear pain, and auditory hypersensitivity.7-9
Although auditory brainstem response (ABR) studies on autistic children have reported various brain and brainstem abnormalities, few studies have investigated OAEs and contralateral suppression (CLS) of OAEs in these children.
Therefore, in this study, we evaluated cochlea, MOS, and brainstem function in autistic children by measuring evoked OAEs and CLS of OAEs.
Materials and Methods
Ethics Statement
This study was approved by the Istanbul Umraniye Research and Education Hospital Ethics Committee. Informed consent was obtained from the parent of each child prior to the onset of the study.
Study Population and Design
In total, 65 children were enrolled in this study. The study group consisted of 55 children (age range: 6-13 years) with normal hearing and neurodevelopment, but diagnosed as autistic, as defined by the 1994 American Psychiatric Association criteria. The control group consisted of 10 healthy children (range: 6-12 years) with normal hearing.
Prior to the study, all children underwent an ear, nose, and throat examination with tympanometry. Children with serous or acute otitis, perforation of the tympanic membrane, or who had cerumen impaction were excluded. Hearing status of the study group was evaluated using a brainstem auditory–evoked response test. During the test, children were instructed to sit still, be silent, and not chew.
Of the study group, we excluded 3 children with serous otitis, 2 with ear plugs, and 29 who did not fulfill the test requirements. Thus, only 21 autistic children completed the study.
Transient-Evoked Otoacoustic Emission Measurements
All patients underwent OAEs measurement using a screening device (Echoport ILO292 USB-II; Otodynamics Ltd, Hatfield, UK) that measured the transient-evoked OAE (TEOAE) and CLS of TEOAE. Transient-evoked OAE measurements were used to evaluate cochlear activity, and CLS values were used to assess MOS efferent activity. Total time for both tests was approximately 10 to 15 minutes. The signal, noise, and signal-to-noise ratio (SNR) were used as parameters in our study. We used the following test parameters for TEOAE measurements: test frequency (1000, 1400, 2000, 2800, and 4000 Hz), stimulus (84 ± 3 dB), test type (TE, linear, and bilateral), time out (26 stimulus higher than noise level), noise rejection level (49.5 dB sound pressure level), wave reproducibility (>70%), stability of the stimulus (>80%), and a test probe (disposable UGD probe).
For CLS measurements, a bilateral test was used with the abovementioned TEOAE parameters. In one ear, we provided a linear click TEOAE stimulus of 84 ± 4 dB, and in the other ear, 60 dB of white noise was administered using a linear stimulus mode. Bilateral measurements were made to compare TEOAE and CLS values. The signal, noise, and SNR from both tests were recorded as study parameters. The signal and SNR responses from both groups were calculated as the difference in the TEOAE values before and after suppressor noise. The suppression amplitudes were classified as “with suppression” when the signal was positive and “no suppression” when the signal was negative.
Statistical Analysis
Means and standard deviations were calculated for continuous variables. Patient characteristics and demographics were analyzed descriptively. Normal distribution of the variables was analyzed using a Kolmogorov-Smirnov test. χ2 and Student t tests were used to evaluate associations between categorical and continuous variables. The logistic regression method was used to identify risk variables by including all variables in the model and calculating the odds ratio.
Results
The mean age was 9.1 years in the study and control groups (range: 6-13 and 6-12 years, respectively). There was no significant difference between the groups with regard to age (P > .05).
Table 1 and Figure 1 depict the right ear OAE and CLS values. For the study group, we did not observe any significant differences between these values for the right ear (P > .05). However, for the left ear, the OAE values were significantly higher than the CLS values (P < .05). For the control group, the OAE values of the left and right ears were higher than the CLS values for both ears (P < .05).
Left and Right Ear OAE and CLS Values for All Patients.
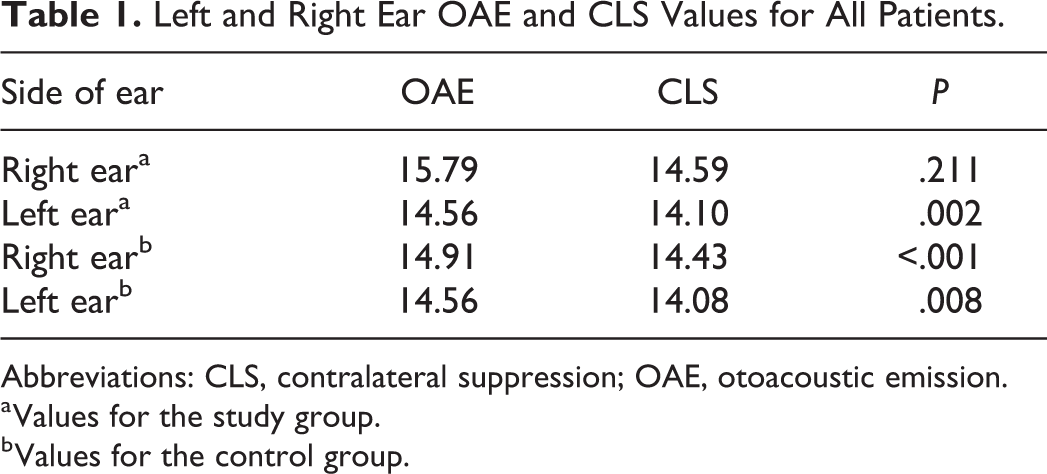
Abbreviations: CLS, contralateral suppression; OAE, otoacoustic emission.
a Values for the study group.
b Values for the control group.
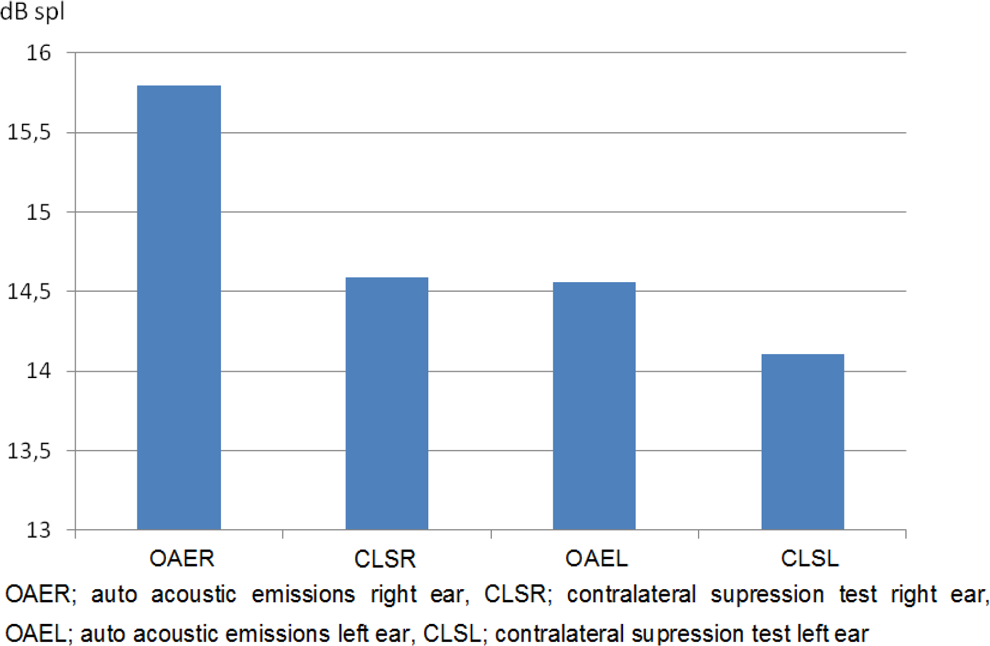
Left and right ear OAE and CLS values for the study group. CLS indicates contralateral suppression; OAE, otoacoustic emission.
Discussion
In this study, we evaluated the cochlea, MOS, and brainstem function in autistic children by using evoked OAE and noninvasive CLS tests. We observed no difference in the mean age of the study and control groups. In the study group, the OAE and CLS values of the right ear were not significantly different (P > .05). However, for the left ear, the OAE values were significantly higher than the CLS values (P < .05). For the control group, the OAE values of the left and right ears were significantly higher than the CLS values for both ears.
Previous studies have reported the relationship between abnormal MOS lateralization and asymmetry of the efferent system and learning disabilities in autistic children. In actuality, in autistic children, language and communication deficiency is related to left hemisphere deficits, and both verbal and nonverbal learning disabilities are related to right hemisphere deficits.10,11
For over 2 decades, ABR has been used to evaluate brainstem disorders. 12 Recently, studies have reported that in autistic children with normal hearing, there are the following 3 ABR abnormalities: third- and fifth-waves with interpeak latency (IPL) elongation, absolute wave latency elongation (first-fifth waves), and abnormal interval time differences. No difference in terms of gender for these abnormalities was reported.12-14 Elongation of the fifth-wave latency with IPL is a sign of brainstem abnormalities. In a study by Rosenhall et al, 15 37% of the cases had such characteristics. In addition, they reported 18% of autistic children with normal hearing had left and right ear abnormalities with ABR latency. They suggested that the deficient auditory fusion was responsible for the ABR abnormalities. Maziade et al16,17 reported that elongation in the first- and third-waves, as well as in the first-fifth and third-fifth IPLs, was indicative of retrocochlear pathologies.
Measuring emissions using a noninvasive method is important for evaluating cochlear function. 18 We chose to use a noninvasive technique to measure OAE instead of ABR. Gravel et al 19 reported no differences between TEOAE and distortion product OAE of autistic and healthy children. Khalfa et al 20 found that in autistic children with normal development, TEOAE amplitude was more asymmetric in left ear stimulation compared to the right ear. Similarly, they performed a study involving 70 right-handed young adults, in which they concluded that asymmetry may externalize the lateralization of the cochlear system, as well as increase the reactivity and amount of outer hair cells in the right cochlea compared to the left. 21
In a study of 14 children with normal hearing and a language deficit, it was reported that they have significantly lower OAE suppression under contralateral acoustic stimulation.10,22 The authors indicated that these children had abnormalities in the inhibitory auditory pathways, which include efferent MOS fibers that reside within the cochlea. Interestingly, these children had greater reduced OAE suppression in the right ear than in the left ear, which was also observed in autistic adolescents. 20 We believe these results indicate that MOS function may be lateralized similar to other brain functions.
In normal hearing autistic and healthy children, we observed no correlation between OAE amplitude and CLS values. Furthermore, the data for each ear were independent from the other ear, in terms of auditory function.20,22 The results of MOS lateralization in autistic children indicated an abnormal arrangement of peripheral fibers. 23
In this study, we found statistically significant differences in TEOAE and CLS of TEOAE in our control group. However, in the study group, we observed no difference in these values in the right ears, but we did observe statistically significant differences in these values for the left ears. Our results also support previous studies by Khalfa et al 20 and Collet et al 22 who showed that OAE had a more continuous suppression in the right ear compared to the left ear. We agree that asymmetry may be responsible for peripheral auditory lateralization in both ears.
In conclusion, in autistic children with normal hearing, MOS functions more effectively in the right ear compared to the left ear. We believe asymmetry may be responsible for peripheral auditory lateralization and the differences between the left and right ears. Further randomized controlled studies with more participants should be designed to have more accurate results on this topic.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.