
Abstract
Objective:
Digastric ridge (DR) is an important landmark to locate facial nerve (FN) and sigmoid sinus for mastoid surgeries and transmastoid approaches. We aim to look for the effect of temporal bone pneumatization on the morphometry of the DR and its relation to the adjoining structures.
Methods:
Temporal bones were harvested from unclaimed cadavers after the approval of the ethical committee. The dissection of the temporal bones was performed under a microscope, and the length of the DR and the distance between the mastoid segment of the FN and the anterior end of DR (FN-DR distance) were measured using a digital caliper. Stata version 14.0 was used to perform the statistical calculations.
Results:
Ninety-three temporal bones were microdissected (right:left = 47:46; well pneumatized:poorly pneumatized = 58:35). Mean length of the DR was 17.1 mm and was significantly longer in well-pneumatized bones (P = .0000). The mean distance between the anterior end of the digastric ridge and the mastoid part of the facial nerve was 4 mm. The distance was significantly more in well-pneumatized bones.
Conclusion:
Prominence and the length of the DR, as well as the FN-DR distance, are significantly more in well-pneumatized bones compared to poorly pneumatized bones. This finding has potential surgical implications with reduced risk of injury to the FN resulting from a conspicuous DR in well-pneumatized bones.
Introduction
Digastric ridge (DR) is a bony elevation present inferiorly in the mastoid cavity at the level of the mastoid process. The DR corresponds externally to the digastric groove at the medial aspect of the mastoid process, from which the posterior belly of digastric muscle originates. 1,2 The DR divides the mastoid tip cells into 2 groups, the lateral and medial (subsinus cells at the sigmoid mastoid terminalis) tip cells. 3,4 Clinically, the DR is an important landmark in the identification of the facial nerve (FN) and sigmoid sinus (SS). 5,6 The morphology of the DR varies from person to person and is usually more prominent in the pneumatized than in the sclerosed temporal bones.
Identification of the FN requires a 3-dimensional understanding of the anatomical course, relations, and variations of the nerve and the surrounding structures. The identification of the nerve becomes a more challenging task in the under-pneumatized (UP) temporal bones. Due to lack of morphometric knowledge about DR surgical anatomy in the literature, we studied the DR anatomy in the cadaveric temporal bones with an objective to measure the anteroposterior length of the DR, its distance from the mastoid portion of the FN, and its comparison with the pneumatization of the temporal bone.
Materials and Methods
Ninety-three fresh wet temporal bones were dissected in our departmental dissection laboratory after approval from the Institute Ethical Committee (IEC-67/03.03.2017, OP-04/03.11.2017), in accordance with the 1964 Helsinki declaration and its later amendments. The microdissections were carried out at a magnification of 6.4, with the assistance of a Leica M320 F12 microscope with attached light-emitting diode, which has an inbuilt 3-megapixel camera plus HD video system (Wetzlar, Germany). A Forte 200 (Zhengzhou Linker Import & Export Co. Ltd., Henan, China) electric micro drill at a speed of 25 000 rpm was used for dissection.
The bones were fixed in the temporal bone holder and after identification of McEwen’s triangle, cortical mastoidectomy was performed. Each bone dissection procedure was recorded, and important pictures were taken separately under the microscope for further analysis. The pneumatization pattern of the bones was categorized as either well pneumatized (WP) or UP/sclerosed by the dissector. All the bones were analyzed for the anteroposterior (A–P) length of the DR (measured from SS to the level of the posterior meatal wall) and the distance between the anterior end of the DR and vertical FN (FN-DR distance; Figure 1).
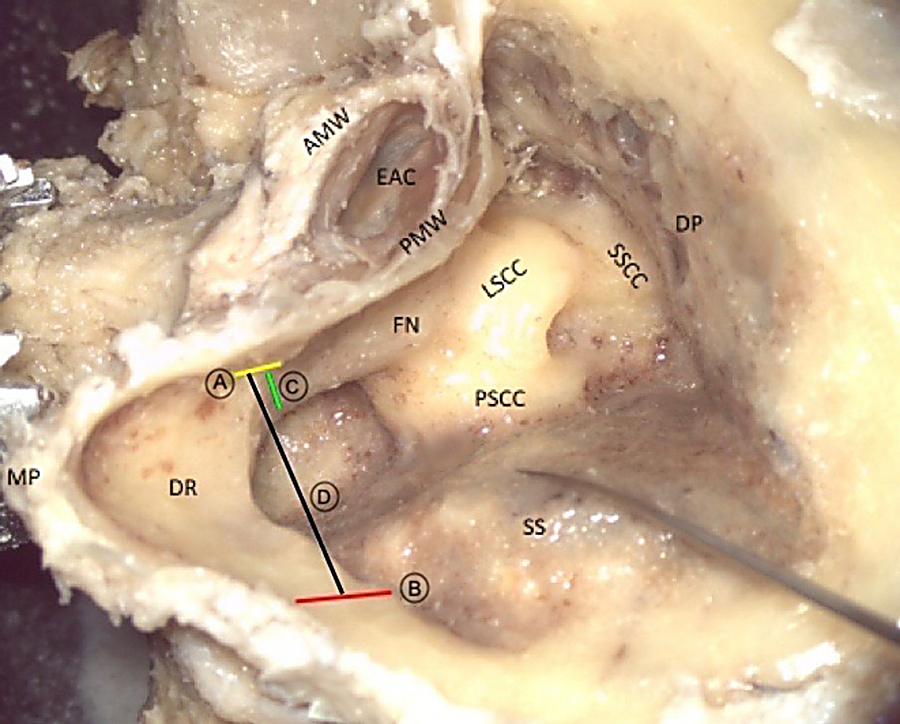
The length of the DR (black line, labeled as D) measured from anterior (yellow line) to posterior (red line) end of the ridge, and the depth of the facial nerve from anterior end of the DR (yellow line) to the nearest point on the mastoid portion of the facial nerve (green line, labeled as C) depicted in a well-pneumatized temporal bone. AMW indicates anterior meatal wall; DP, dural plate; DR, digastric ridge; EAC, external auditory canal; FN, facial nerve; LSCC, lateral semicircular canal; MP, mastoid process; PMW, posterior meatal wall; PSCC, posterior semicircular canal; SSCC, superior semicircular canal, SS, sigmoid sinus.
The length (A–P) of the DR and the FN-DR distance were assessed using a digital caliper. All the measurements were charted in Excel 2007.
Statistical Analysis
The morphometric data were expressed as mean ± standard deviation (SD). The analysis of the length of DR and the FN-DR distance with respect to the pneumatization were performed by unpaired t-test using statistical software Stata version 14.0 (Stata Corp, 4905, Lakeway drive, College Station, Texas). A P value of less than .05 was taken as statistically significant.
Results
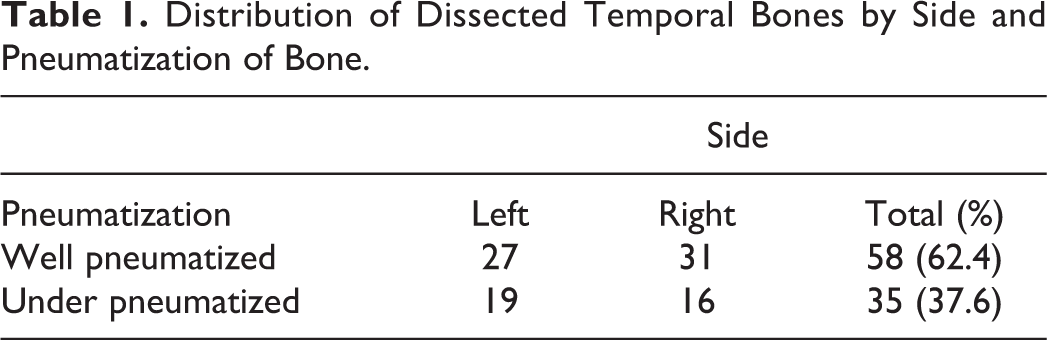
A total of 93 temporal bones were microdissected, of which 46 (49.5%) were left sided and 47 (50.5%) were right sided. The distribution of temporal bones according to the pneumatization and side is mentioned in Table 1.
Distribution of Dissected Temporal Bones by Side and Pneumatization of Bone.
The mean length of the DR was 17.1 mm (SD: 3.2; range: 7.6-25.1 mm). The length of the DR was more in WP bones than in the UP bones, and the difference was statistically significant (P = .0000; Table 2).
The Variability of the Digastric Ridge Anteroposterior Length With Respect to the Pneumatization.a
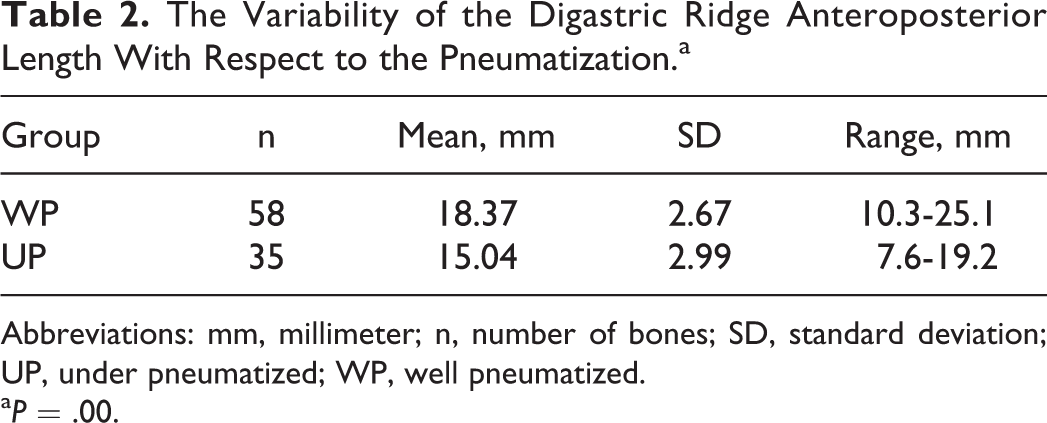
Abbreviations: mm, millimeter; n, number of bones; SD, standard deviation; UP, under pneumatized; WP, well pneumatized.
aP = .00.
The mean depth of the FN from the anterior end of the DR was 4 mm (SD: 1.17; range: 1.3-7.8 mm). The FN was always present medial to the DR at varying depth. The depth varied with pneumatization and was significantly more in WP bones than in UP bones (P = .0000; Table 3).
The Variability of the FN-DR Distance With Respect to the Pneumatization.a
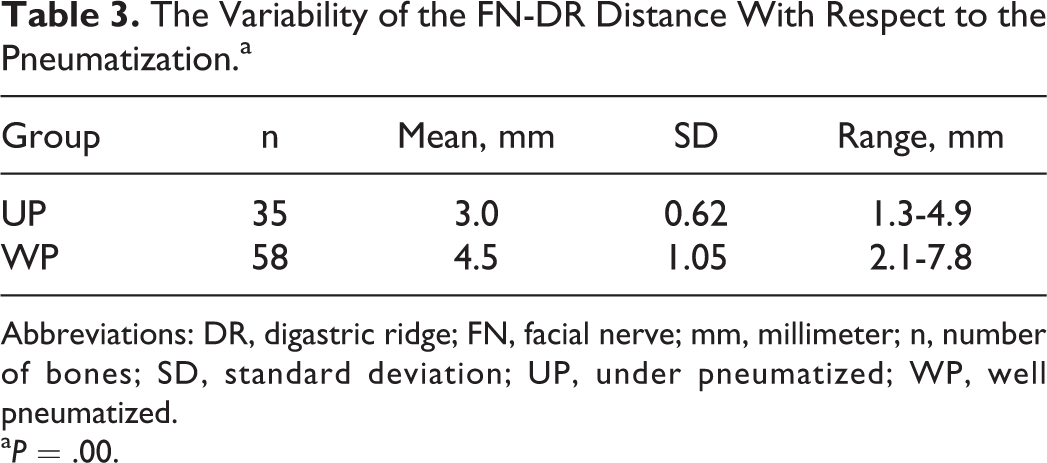
Abbreviations: DR, digastric ridge; FN, facial nerve; mm, millimeter; n, number of bones; SD, standard deviation; UP, under pneumatized; WP, well pneumatized.
aP = .00.
Discussion
Digastric ridge extends from the SS posteriorly to the posterior meatal wall anteriorly. The SS lies posterosuperior to DR and as it advances anteriorly, it comes to lie medial to DR. Considered as a landmark of variable importance in literature, it can act as an excellent guide to locate the mastoid segment of the FN and the SS during the transmastoid and lateral approaches to skull base. 7
The anteroposterior length and prominence of the DR vary from one temporal bone to another. We studied 93 temporal bones, and the average anteroposterior length was found to be 17.1 mm (±3.2 mm). However, this length differed significantly between WP (18.4 ± 2.7 mm) and UP (15.0 ± 3 mm) bones (P = .0000; Table 2).
The anterior end of the DR is one of the landmarks to identify the vertical part of the FN. 6,8 The mastoid segment of the FN lies anteromedial to the anterior end of DR at varying depth. Our results are in concordance with Yadav et al, 9 who found the FN-DR distance to be 3.8 mm (±0.8 mm; range: 2-5 mm). The mean depth in our experience was 4 mm (±1.2 mm). As with the length of the DR, the FN-DR distance was more in WP bones (4.5 mm) than in UP bones (3 mm), and the difference was statistically highly significant (P = .0000; Table 3).
We concur with the notion of development and prominence of DR to be related to the development of mastoid pneumatization. One of the areas of concern for the recurrence of disease (eg, cholesteatoma) is medial to DR. Operating in this narrow area can injure the SS or the FN, and the probability of the injury is more in the poorly pneumatized bones than in the WP bones, given the conspicuity of the DR in the latter, which makes the identification of the vital structures less demanding. This fact is supported by the results of our study showing a longer and more prominent DR with a deeper situated mastoid segment of the FN in WP bones compared with the sclerosed ones. To avoid the dreaded complications resulting from injury to these vital structures, a thorough understanding of the intricate anatomy of the temporal bone through laboratory dissections is indispensable. 10
Conclusion
Digastric ridge is an important landmark to identify FN in mastoid surgeries/transmastoid approaches. Facial nerve always lies medial to the anterior end of the DR, albeit at varying distances. The conspicuousness and length of the DR and the distance of the FN from the anterior end of the DR are significantly more in WP bones than in sclerotic mastoids. A WP temporal bone provides a safer surgical corridor with respect to injury to the FN and SS.
Footnotes
Authors’ Note
Human cadaveric study approved by the institutional review board and institutional ethical committee (IEC-67/3.3.17).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Research Section, All India Institute of Medical Sciences, New Delhi, India, file No. F.8-522/A-522/2017/RS (project code No: A-522) dated September 19, 2017.