
Abstract

An 86-year-old male presented with a 2-year history of a gradually enlarging parotid mass. He denied any facial weakness, numbness, or pain. He was a nonsmoker and occasional alcohol user. The patient had no history of cutaneous malignancy. Examination revealed normal facial nerve function and a 1.5-cm firm, mobile left parotid mass. The remaining head and neck examination was significant for a firm, exophytic, friable mass at the left base of tongue (Figure 1) and a firm, enlarged left level III lymph node. Ultrasound of the parotid was performed, which showed a cystic 2.2 cm lesion with minimal solid components. Fine needle aspiration (FNA) of the parotid demonstrated clusters of epithelial cells and FNA of the level III neck was positive for poorly differentiated squamous cell carcinoma. Positron emission tomography scan showed an fluorodeoxyglucose (FDG)-avid left base of tongue tumor with increased avidity in the left neck levels II and III as well as the left parotid gland (Figure 2). The patient was taken to the operating room and underwent robot-assisted left base of tongue resection, left select neck dissection levels II to IV, and left superficial parotidectomy. The primary base of tongue tumor was a 3.1 cm grade 3 HPV-positive squamous cell carcinoma. Four of 39 lymph nodes in the neck were positive, the largest being 5 cm with extracapsular extension. Surgical margins were negative. Frozen section pathology of the superficial parotid gland was positive for metastatic squamous cell carcinoma. This finding prompted proceeding with total parotidectomy. Two of 7 intraparotid lymph nodes were positive, both in the superficial parotid. The patient recovered well and was treated with adjuvant proton radiotherapy.
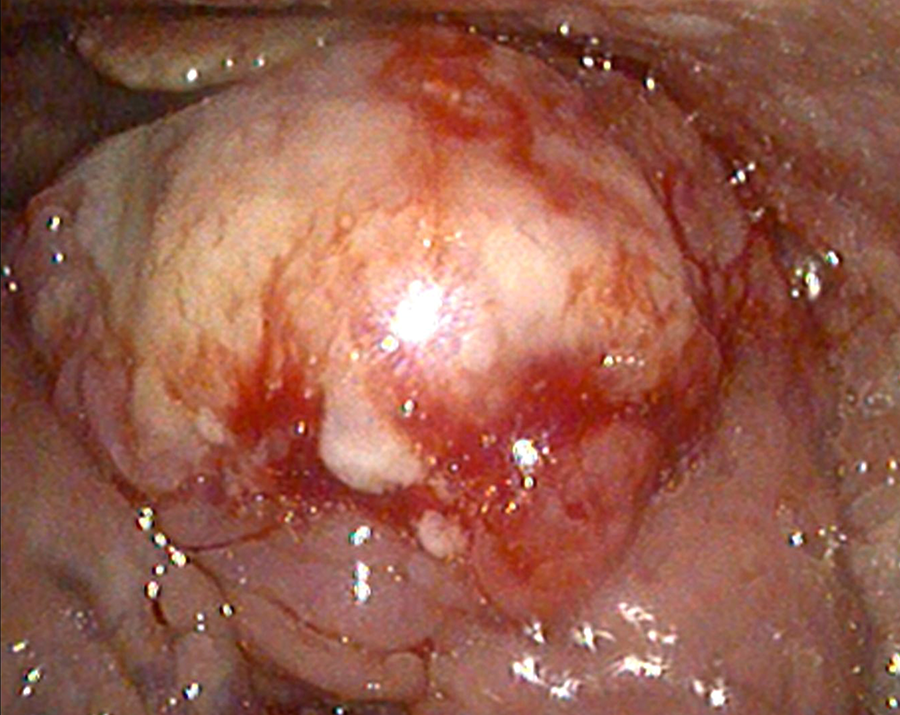
Flexible fiberoptic nasopharyngoscopy showing an exophytic left base of tongue mass.
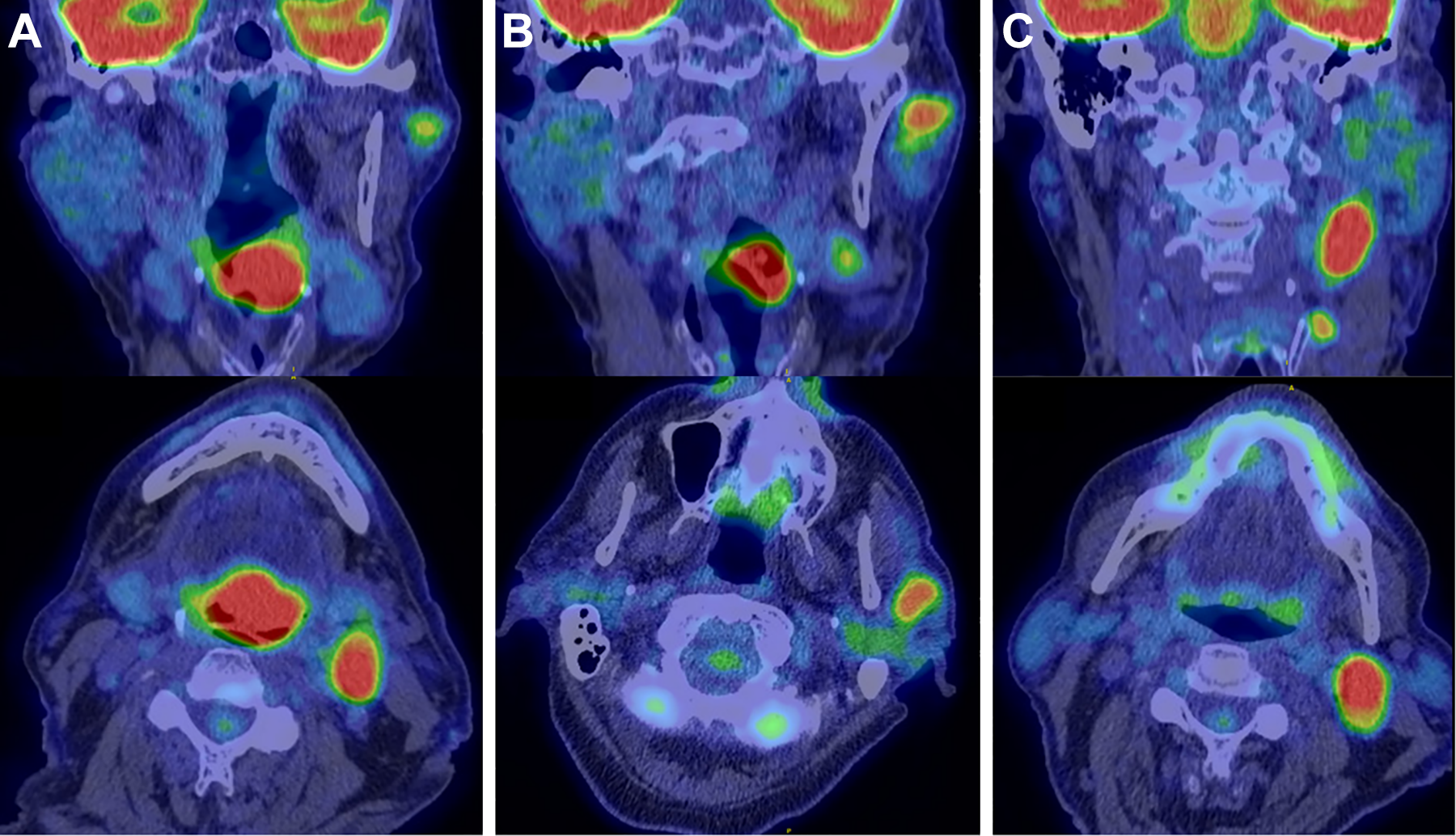
A, Positron emission tomography CT showing a 3-cm left tongue base mass with marked fluorodeoxyglucose (FDG) avidity. B, Positron emission tomography CT showing FDG avid left superficial intraparotid nodule. C, Positron emission tomography CT showing FDG avid left level II and III cervical lymph nodes. CT indicates computed tomography.
Salivary gland tumors represent 5% to 10% of tumors within the head and neck. 1 Of these, 80% arise from the parotid gland. 1 The ability of otolaryngologists to appropriately evaluate and treat parotid masses is vitally important. A broad differential diagnosis must always be considered. Masses of the parotid gland can represent both benign and malignant neoplasms, among other etiologies. Parotid gland neoplasms represent malignancy in 20% of cases, one quarter of which are metastasis from head and neck primary sites. 2,3 The parotid gland has unique embryologic development from ectodermal outpouchings, which encapsulate the mesoderm-derived lymphatic system. 2 This results in a wide lymphatic drainage basin from the head and neck to the parotid gland. Most metastatic lesions arise from cutaneous primary malignancies of the scalp and face. 3 Uncommonly, however, malignancies of the upper aerodigestive tract will metastasize to the parotid gland. 3,4
It has been proposed that spread of malignancy to uncommon sites, such as the parotid gland in upper aerodigestive tract lesions, may be secondary to disruption of normal lymphatic drainage pathways. 5,6 This could occur as a result of previous surgical intervention, radiation therapy, or significant cervical disease burden. 7 Had the primary site and metastatic neck disease gone unnoticed in this case, the oropharyngeal malignancy may not have been identified until significant progression had occurred. This case illustrates the importance of a thorough head and neck examination. Findings can significantly impact management and outcomes. In conclusion, metastatic upper aerodigestive tract malignancies, although rare, should be considered when evaluating patients with parotid masses.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.