
Abstract
Background:
With the extensive development of endoscopic sinus surgery, iatrogenic medial rectus muscle injury should be treated with caution. Traditional methods to repair a ruptured medial rectus need an anterior orbitotomy approach, with more injury and difficulty in finding the posterior end of the ruptured medial rectus.
Objective:
To explore a new method to repair a ruptured medial rectus.
Methods:
Eight cases of iatrogenic medial rectus rupture after endoscopic sinus surgery were reviewed from July 2015 to January 2019. Assisted by image-guided navigation, the ruptured medial rectus was sutured under an endoscopic endonasal orbital approach. Two methods were designed to suture the ruptured medial rectus. Optic nerve and orbital decompression were performed in 5 cases with visual impairment. The extent of exotropia and diplopia were followed up for 5 to 33 months after surgery.
Results:
With the help of image guidance, the posterior and anterior ends of the ruptured medial rectus of all patients were pinpointed, and operations using medial rectus anastomosis were successfully completed in 7 patients. The exotropia of these patients was corrected, and they have recovered. The vision of 2 patients recovered. There were no minor or major complications intraoperatively or postoperatively.
Conclusion:
Assisted by image-guided navigation, medial rectus anastomosis under an endoscopic endonasal orbital approach is a feasible method. The key to preventing orbital complications is strict professional training, including identification of the Onodi air cell and correct application of powered instrumentation.
Introduction
Rupture of the medial rectus is an uncommon event, which is caused by trauma, iatrogenic injury, or tumor. As the paranasal sinuses are situated in close proximity to the orbit, there is a risk of inadvertent orbital entry during endoscopic sinus surgery (ESS). A wide variety of orbital complications following ESS have been reported in the literature. These complications included extraocular muscle injury, optic nerve damage, nasolacrimal duct injury, orbital hemorrhage, and so on. 1 Endoscopic sinus surgery is widely applied for obstructive sinus disorders, particularly for chronic rhinosinusitis with or without nasal polyps. The advances in endoscopic techniques and dynamic systems have greatly promoted the development of ESS. These techniques improve the success rate of operations but also increase complications such as eyeball and skull base injuries. 2 The most severe injuries involve the optic nerve and medial rectus, which cause loss of vision, diplopia, and disorders of eyeball movement. Recently, many cases about injuries of the medial rectus during ESS are reported. 3 -6 Stankiewicz et al reviewed the complications in ESS for chronic rhinosinusitis involving 3402 patients (6148 sides) during a period of 25 years. An overall patient complication rate of 3.1%, or 1.7% per operated side, was noted. 1 In a retrospective cohort analysis involving 78 944 primary ESS cases from 2005 to 2008, Krings et al noted a complication rate of 0.36%. 7 Suzuki et al had data from 50 734 Japanese patients who underwent ESS for chronic rhinosinusitis between 2007 and 2013. The overall complication rate was 0.50%; the rate of orbital complication was 0.09%. 8 Medial rectus rupture results in exotropia and diplopia, which seriously affect the patient’s eye function and appearance.
Medial rectus anastomosis is an optimal therapy. Traditionally, medial rectus anastomosis needs an anterior orbitotomy approach, which may cause incision on conjunctiva and adds more injury. By this approach, it is sometimes difficult to find the posterior end of the ruptured medial rectus. Thus, it is necessary to find a new approach and method to retrieve ruptured medial rectus. A case report by Akiyama et al described a unilateral ruptured medial rectus muscle caused by trauma with an endoscopic endonasal orbital approach. 9 In another report by Lenart et al, lost medial rectus muscles were retrieved in 4 eyes with either a transcutaneous medial orbitotomy approach or an endoscopic endonasal approach. These combined techniques from both ophthalmology and otorhinolaryngology were adopted to help solve the problem. 10
From July 2015 to January 2019, 8 patients with a medial rectus injury in either the left or right orbit after ESS were referred to the ENT department of the Tongji Hospital for treatment with an endoscopic endonasal orbital approach under image-guided navigation. In this article, we mainly describe the surgical approach, the medial rectus anastomosis method, and the intended purpose for this technique.
Patients and Methods
Clinical Data
This is a retrospective, case series study. The medical records of 8 cases of iatrogenic medial rectus rupture were reviewed from July 2015 to January 2019. These patients underwent medial rectus anastomosis with image-guided navigation through an endoscopic endonasal orbital approach at the Department of Otolaryngology–Head and Neck Surgery, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology. Data were collected from operative reports, hospital charts, and preoperative and postoperative ophthalmologic examinations, including the angle of exotropia. The patients’ demographics are displayed in Table 1. The 8 patients were sorted by admission time.
Clinical Data.
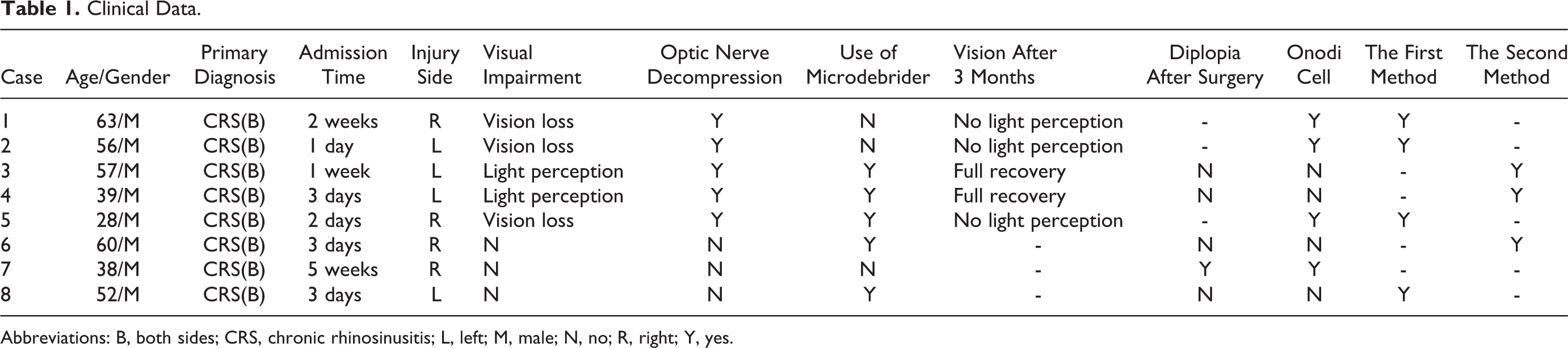
Abbreviations: B, both sides; CRS, chronic rhinosinusitis; L, left; M, male; N, no; R, right; Y, yes.
All patients had an iatrogenic medial rectus rupture. The time to visit our department was from 1 day to 35 days after ESS. Each patient had the medial rectus rupture on one side, and 5 of them simultaneously had optical nerve damage on the same side. The injured eye was in the abduction position, and this eye could not be adducted yet. The broken papyraceous lamina and medial rectus are clearly seen on thin-layer paranasal sinus computerized tomography (CT; Figure 1). The thickness of sinus CT slices should be less than 1 mm, which was helpful to precisely locate and characterize even minimal lesions and was able to be reconstructed as a 3-D image by a Fusion image-guided navigation system (Medtronic Navigation, Inc, Louisville, Colorado). This study was approved by the ethical committee of our hospital, and a written informed consent was obtained from each subject.
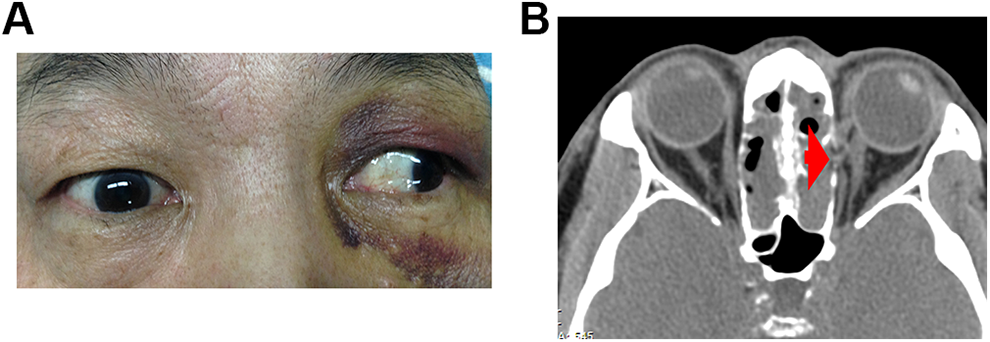
Clinical photographs of case 3. A, The abduction position of the left eye. B, Paranasal sinus computerized tomography scan showed a left orbital wall fracture and a ruptured medial rectus (arrow).
Surgical Procedure
In all patients, surgery was performed under general anesthesia through orotracheal intubation. Each patient was supine with the head in a neutral position and a 10° to 15° adduction to the patient’s right. The Fusion navigation system was installed and registered preoperatively. Cotton pledgets soaked in xylometazoline solution were placed in the nasal cavity to ensure vasoconstriction.
First, ESS was performed again to clean the stuffing that was used to fill the paranasal sinus and to clean secretions and bone slices. The paranasal sinus that was not opened in the last ESS was opened.
Then optic nerve decompression and posterior orbital decompression were done because 5 of the cases were also accompanied by optical nerve damage on the same side. Assisted by image-guided navigation, the broken point of the papyraceous lamina, orbital apex, and optic canal were pinpointed. The posterior papyraceous lamina was removed from the broken point to the orbital apex to finish the posterior orbital decompression. The bone of the optic canal was carefully removed with a diamond burr and the optic nerve sheath was not incised.
And last, a medial rectus anastomosis under an endoscopic endonasal orbital approach was performed. The orbital periosteum, orbital fat, and medial rectus were carefully identified using the nasal endoscope with image guidance. Especially, the posterior end and anterior end of the ruptured medial rectus should be identified. This was the key to a successful medial rectus anastomosis. There were 2 different surgical strategies for a medial rectus rupture or a defect. For cases 1, 2, 5, and 8, the medial rectus was ruptured, and the posterior and anterior ends of the ruptured medial rectus were close to each other, so the direct anastomosis method was adopted. The dissociated posterior and anterior ends of the ruptured medial rectus were sutured with 5-0 Vicryl sutures (the first method, Figure 2). For cases 3, 4, and 6, the defect of the medial rectus was too large to be sutured directly, so a knot using a 5-0 Vicryl suture was tied onto the posterior end of the medial rectus and then the suture was led out along the medial rectus to the outside of the eyeball. The ophthalmologist then made another knot to the anterior end of the medial rectus to link it and adjusted the angle of exotropia to place the eyeball in the median position or slightly medial (the second method, Figure 3). A gelatin sponge was placed in the ethmoid sinus to stabilize the eyeball.
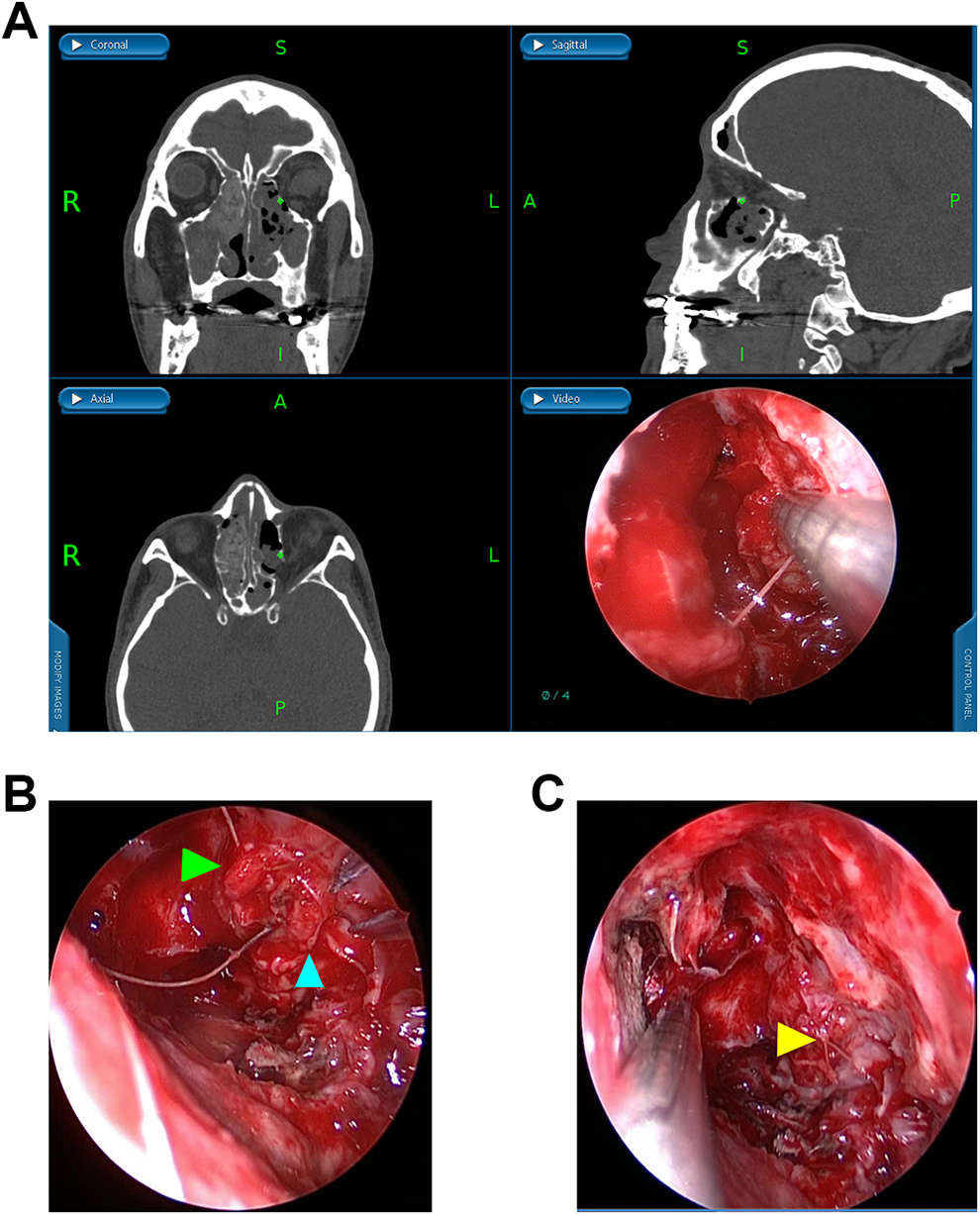
The process of the first method. A, Ruptured medial rectus was pointed out intraoperatively. B, Both ends of ruptured medial rectus (arrows) were sutured. C, The result of suturing.
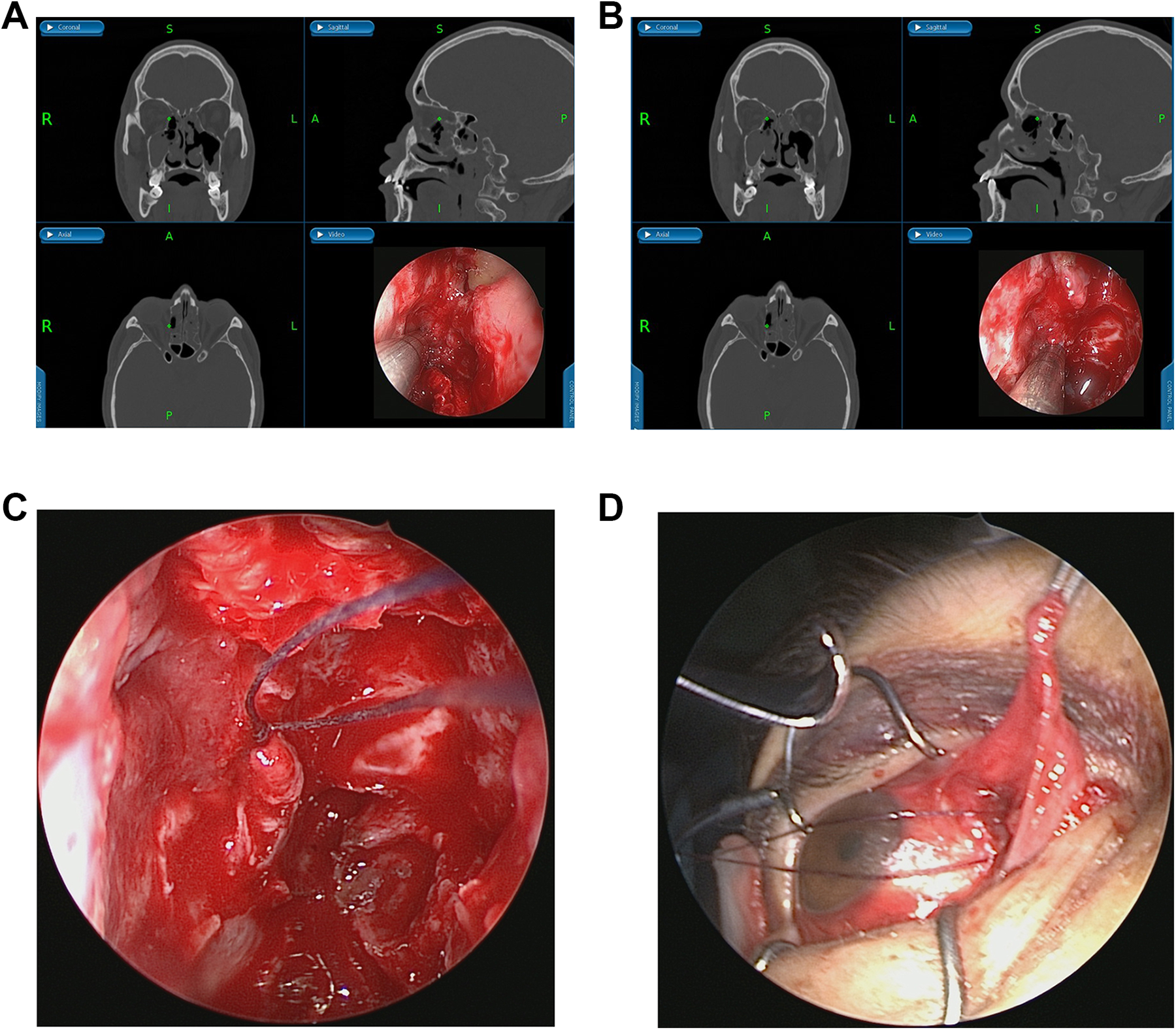
The process of the second method. The anterior end (A) and the posterior end (B) were pinpointed. (C and D) Both ends were linked through endoscopic endonasal and orbital approach.
The postoperative treatment was not eventful, just like the ESS postoperative routine treatment. Patients were treated with antibiotics and nasal irrigating agent. Patients underwent the second method were treated with tobramycin–dexamethasone eye ointment.
Intended Purpose
The purpose of the medial rectus anastomoses was 2-fold: to correct the exotropia and diplopia in patients with vision and to correct the abduction of eyeball and restore the patient’s appearance and balance in patients without vision.
Results
The posterior and anterior ends of the ruptured medial rectus of 8 patients were pinpointed with the help of image guidance, and operations of medial rectus anastomosis were successfully completed in 7 patients. The exotropia of these 7 patients was corrected and their appearance recovered (Figures 4 and 5). Only in case 7, both posterior and anterior ends of the ruptured medial rectus were pinpointed, but the highly edematous muscle tissue was failed to be sutured. Two of the 5 patients with visual impairment improved their vision and did not show diplopia. Diplopia in 4 cases was corrected. No minor or major complication occurred intraoperatively or postoperatively, with a follow-up time of 5 to 33 months.

The position of eyes in case 6. A, The position of right eye preoperatively. B, The position of right eye postoperatively. C, The position of right eye 3 months after operation.
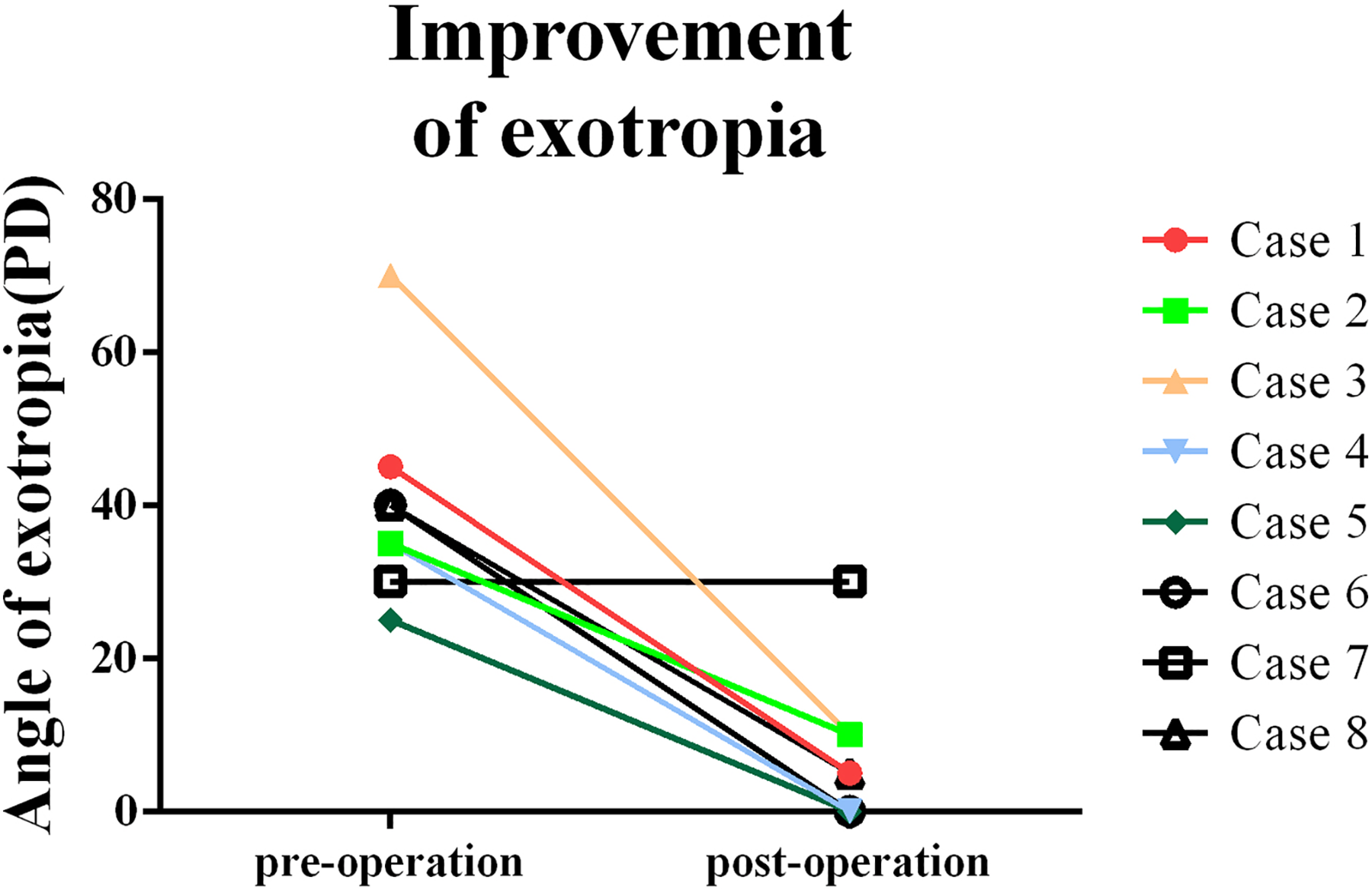
The angles of exotropia of the injured eyes preoperatively and postoperatively (3 months after surgery).
Discussion
Iatrogenic medial rectus rupture is a rare but devastating orbital complication. Chronic rhinosinusitis is estimated to affect 15% of the adult population. Treatment of chronic rhinosinusitis is highly variable. When medical therapy is ineffective, ESS may be recommended to relieve symptoms. However, complications can occur during ESS, including devastating orbital complications such as medial rectus rupture and blindness. A report by Geyton et al showed that in the United Kingdom between 1995 and 2010, there were 65 ear, nose, and throat clinical negligence claims paid by the National Health Service. Fifty claims were related to surgical complications. Claims due to surgical complications from ESS were most successful, involving 11 cases of orbital injury, which included 6 cases of visual loss and 5 cases of diplopia. 11 A study by Svider et al was based on “Jury verdict and settlement” reports to detail factors governing legal outcomes in iatrogenic orbital injury. Twenty cases of iatrogenic orbital injuries were included. Complications coming from ESS were most common (50.0%), and diplopia was the most common medical complaint (50.0%). 12
Once the medial rectus ruptures, the patient will have exotropia and diplopia, which not only affects the eye function but also affects the appearance of the patient. The medial rectus rupture was often accompanied by optic nerve damage during ESS, resulting in visual impairment or even blindness. In this study, there were 5 cases with visual impairment in 8 patients. Medial rectus rupture and blindness may be difficult to recover, resulting in permanent harm to the patient or a high risk of a persistent deficit. Optimal therapy generally involves an initial attempt at targeted exploration with attempted repair of the damaged medial rectus. 13 For those patients with vision loss, a medial rectus anastomosis can restore the appearance. Once ruptured medial rectus could not be repaired or muscle strength of repaired medial rectus is so weak that the patient becomes exotropia again, an alternative adducent force could be created by transposition of partial rectus or oblique muscle insertions to new locations. However, this transposition procedure may cause fusion, resulting in a limited field of binocular single vision. 14 Furthermore, the lamina papyracea was broken in the ESS for infectious sinusitis, and performing this transposition procedure in a short term may increase the incidence of intraorbital infection.
Assisted by image-guided navigation, medial rectus anastomosis through endoscopic endonasal orbital approach is a feasible method. Previously, medial rectus anastomosis was performed by ophthalmologists using an anterior orbitotomy approach. This approach needs the conjunctiva cutting, which increases the injury. Additionally, it is important to find the posterior end of the ruptured medial rectus. Underdahl 14 reported a high retrieval rate using an anterior orbitotomy approach to perform medial rectus anastomosis. However, the posterior terminal position of medial rectus injured in FESS may near orbital apex and the defect of medial rectus is very large in several cases. It is hard to identify the posterior end of the ruptured medial rectus in a limited surgical field without enough light. An endoscopic endonasal orbital approach can provide enough space and light for directly performing medial rectus anastomosis. In this cohort, 7 out of 8 patients were successfully sutured, which also proved the feasibility of this method.
Furthermore, there are 2 additional benefits to this endoscopic endonasal approach: to perform optical nerve decompression and to manage the lesions left over from the previous ESS. The medial rectus rupture may be accompanied by optic nerve damage. In this study, visual impairment occurred in 5 of 8 patients. The optic nerve could be directly injured by surgical instruments or compressed by highly edematous tissue in the last ESS or compressed by bone chips of lamina papyracea and optic canal. Direct or indirect injury results in tissue edema and blood circulation disorder in optic nerve, which is exacerbated by the constraint of the optic canal and eventually leads to optic nerve degeneration and necrosis. 15 The optic nerve decompression is one of the optimal therapies. 16 And also, when a surgeon became aware of an orbital complication, the planned ESS was usually terminated. This moment, before suturing the medial rectus, the lesion that was not treated in the previous ESS was treated first.
Then 2 different surgical strategies were used to perform medial rectus anastomosis. In the process, the identification of the posterior and anterior ends of the ruptured medial rectus is the key to successful medial rectus anastomosis. In addition to a nasal endoscope, image-guided navigation is a useful tool for pinpointing the posterior and anterior ends of the ruptured medial rectus. During nasal endoscopic surgery, the navigation system can accurately locate important anatomical markers, including the medial rectus, orbital apex, optic nerve, and internal carotid artery. 17 In this study, 7 cases of medial rectus anastomosis were successfully completed, and their exotropia was corrected. At the same time, 5 cases of optic nerve decompression were performed and vision was improved in 2 cases. However, the limitation of the navigation system for mobile soft tissue structures should be mentioned. While the navigation system can provide a general location for medial rectus, by its nature, the medial rectus can move, the surgeon must have caution and strong anatomic knowledge as well.
We also observed that as time went on, it was more difficult to identify the ruptured medial rectus. The ruptured medial rectus had an inflammatory reaction, edema, and adhesion to surrounding tissue, which increased the difficulty in finding the exact location of relevant structures. Therefore, surgical treatment should be carried out as soon as possible in case of medial rectus rupture. In case 7, anastomosis was performed 35 days after the last ESS. Both posterior and anterior terminals of medial rectus were adhered to surrounding tissues and were too fragile to be sutured. For this patient, an extraocular muscle transposition surgery after 6 months could be a feasible therapy.
The key to preventing orbital complications is strict training. The training of a nasal endoscopic surgeon is manifold, including radiology and paranasal sinus and nasal cavity anatomy, particularly as viewed through an endoscope. Eloy et al found that appreciating variants in orbital wall anatomy through preoperative imaging was crucial for avoidance of orbital complications. 18 Variant ethmoid cells include the Onodi cells, Haller cells, and agger nasi cells. An Onodi cell is a posterior ethmoidal cell which develops laterally and/or superiorly to the sphenoid sinus. The optic nerve and carotid artery may be located within or nearby an Onodi cell. In this study, of 5 cases of medial rectus rupture with optic nerve injury, 3 cases occurred in the Onodi cell. This phenomenon should be paid great attention.
The introduction of powered instrumentation in ESS has produced undoubtable advances, but the powered instrumentation may put patients at greater risk. Since Graham and Nerad 19 reported 3 cases of medial rectus injury in ESS using powered instrumentation, special care should be taken in using powered instrumentation. In this study, the medial rectus of 5 patients was damaged by powered instrumentation. Part of the medial rectus was removed, which resulted in the defect of the medial rectus being too large to be sutured directly. Therefore, proper use of the powered instrumentation should also be part of nasal surgeons’ training.
Conclusion
Iatrogenic medial rectus rupture is a rare but devastating orbital complication. The medial rectus anastomosis should be carried out as soon as possible in case of medial rectus rupture. Assisted by image-guided navigation, medial rectus anastomosis under endoscopic endonasal orbital approach is a feasible method. The key to preventing orbital complications is strict professional training, including identification of the Onodi air cell and correct use of powered instrumentation.
Footnotes
Authors’ Note
Ying-Xing Wu and Zhi-Yong Li contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Huazhong University of Science and Technology grant 2016082 to Dr Hong-Tao Zhen and National Natural Science Foundation of China (NSFC) grant 81400448 to Dr Xiao-Bo Long.