
Abstract
Introduction:
Ankyloglossia is a congenital condition that restricts tongue mobility. The aim of this study is to evaluate the relationship between gender and pediatric ankyloglossia and evaluate the planning of ideal timing of surgery.
Methods:
The files of pediatric patients in the Turkish population treated surgically for tongue-tie between June 2014 to June 2018 were scanned retrospectively.
Results:
Three hundred and eighty-two pediatric patients were included in the study. Of these, 115 (30.1%) were female and 267 (69.9%) were male. The prevalence of ankyloglossia was significantly higher in males than in females (P < .001). The age of the patients at time of surgery ranged from 1 day to 114 months. The most common indication was sucking/feeding difficulties (82%) in patients younger than 2 years, and the most common symptom was speech problems (67%) in patients aged 2 years and older.
Conclusion:
In our study, the prevalence of ankyloglossia in Turkish society was significantly higher in males. Frenectomy surgery is a safe procedure that can be performed on the first day of life in newborns.
Introduction
Tongue-tie, also known as ankyloglossia, is a congenital anomaly and is caused by a short, nonelastic frenulum that causes restriction of tongue movements. The prevalence of ankyloglossia is 4% to 10%. It is more common in males. Ethnicity is not a risk factor. 1,2 Ankyloglossia can be accompanied by other craniofacial anomalies such as cleft palate and cleft lip. 3 Symptoms associated with ankyloglossia have been reported to include maternal breast pain, difficulty in breast-feeding in infants, low weight gain, dehydration, and short feeding time. 4 Ankyloglossia can cause various mechanical problems such as difficulty in licking ice cream in adolescents and adults and inability to play instruments such as wind instruments not to clean teeth with tongue. 5 There are studies indicating that this congenital disease is rarely symptomatic. 6
The frenotomy performed in ankyloglossia is a minimally invasive surgical procedure with a high success rate. There are reports, which indicate that surgical intervention during infant period will eliminate the difficulty of sucking experienced in children and that nipple pain in the mother will be less and speech problems may be prevented. 7 –9
On the other hand, it is suggested that most of the cases of ankyloglossia may be asymptomatic, and haste is not necessary for surgery. 10,11 There is no consensus on the ideal timing of ankyloglossia surgery in the literature.
In this study, we aimed to evaluate pediatric patients in the Turkish population treated surgically for ankyloglossia in terms of gender and to compare the timing of surgery with the literature data.
Materials and Methods
Ethics committee approval was obtained for the study (2018/008). The files of pediatric patients who were treated surgically for ankyloglossia between June 2014 and July 2018 were retrospectively reviewed. The complaints were analyzed for gender, age, surgical procedure, and complications.
Results
The study included 382 children who underwent a frenotomy due to ankyloglossia from June 2014 to July 2018 at the clinics of otolaryngology and pediatric surgery. In all patients, the frenulum was cut with scissors. Two hundred and sixty-seven (69.9%) patients were male and 115 (30.1%) were female. The age of the patients ranged from 1 day to 3459 days (Table 1). The mean age at time of presentation was 476.7 ± 691 days in male children and 465.7 ± 563.7 days in female children. There was no statistical difference between the 2 groups in terms of time of presentation (P > .05).
Number of Patients by Age.
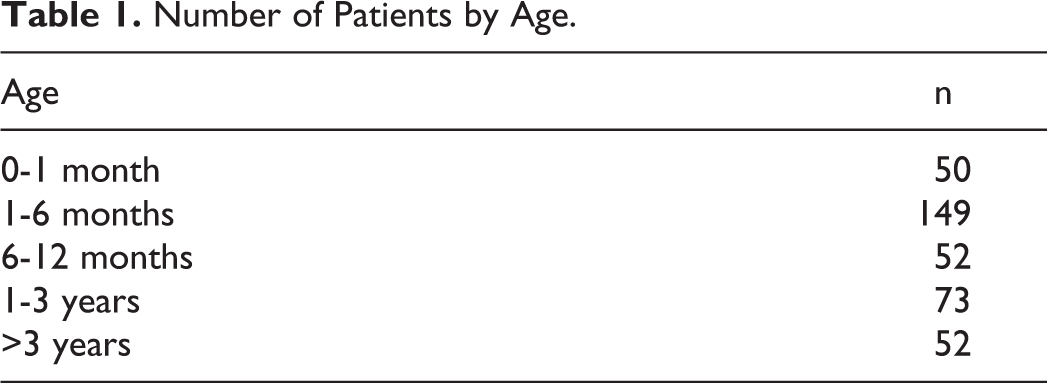
Forty-one patients were younger than 30 days old. Ten of these were given frenotomy on the first day after delivery and 5 on the second day. All the patients who underwent a frenotomy in the first 2 days were diagnosed with ankyloglossia due to difficulty in sucking and evaluated for surgery prior to discharge from hospital.
The most frequent cause for presentation in patients younger than 2 years was sucking/feeding difficulty (82%), and the most common cause in those aged 2 years and older was of speech disorder/inability to pronounce certain letters (67%). In 75.9% (n = 290) of the patients, the procedure was performed without anesthesia or with local anesthesia, while 18.3% (n = 70) patients were sedated. General anesthesia was preferred in 5.8% of the patients (n: 22) because of adenoidectomy / tonsillectomy, hernia, and circumcision being performed in addition to the frenotomy. While most of the patients (81.1%) did not require any intervention as a result of cutting the frenulum with scissors, in 76 (19.9%) patients, bleeding was controlled by bipolar cauterization or suturing following the frenotomy. Wound site infection was not observed in any of the patients, and 9 (2.35%) patients underwent revision frenotomy surgery due to continuance of frenulum.
Discussion
This study showed that congenital tongue tie is more common in males in the Turkish population. In our study, the male–female ratio was 2.32:1. In the literature, it is reported that the prevalence of ankyloglossia was more frequent in males. 1 –11
Karabulut et al reported that 70.2% of 127 pediatric patients with ankyloglossia were male, and the rate of male–female gender was 2.6:1 in their study. 12
In the literature, it has been reported that ankyloglossia is more common in male patients by around 1.6- to 3-fold. 1,10,13,14 Literature also reported different opinions in terms of the ideal timing of ankyloglossia surgery. Some authors have argued that surgery should be performed prior to the newborn being discharged from the hospital. In contrast, some authors reported that when diagnosed in newborns, they should be followed and treated when they become symptomatic. There are publications, which state, as in our study, that if there is nutritional deficiency in the newborn and if ankyloglossia is detected, frenotomy can be performed safely on 1-day-old newborns. 4,5,10,15
The authors who advocated the wait-and-see method reported that ankyloglossia is asymptomatic in many children and that tongue movements can recover spontaneously or that the affected children can compensate for reduced tongue mobility. Therefore, they advocate waiting until a speech disorder develops in pediatric patients and usually recommend surgery after the age of 4 years. 10,16,17
In addition to speech disorders due to the limitations in tongue movement, ankyloglossia can affect the person socially as a result of mechanical problems such as not being able to play wind instruments and not being able to clean the teeth with the tongue. For this reason, surgery should be recommended to parents when ankyloglossia is detected due to possible late-onset symptoms. 5
In a randomized controlled trial by Buryk et al on 30 infants with ankyloglossia aged between 1 and 35 days (mean 6.6 days), frenotomy was reported to correct the feeding immediately and reduce breast pain in the mother. In the same study, no complication was reported in any of the newborns who underwent frenotomy. 15
Different techniques have been defined in the ankyloglossia surgery, and the most common frenotomy and frenuloplasty are applied. Frenotomy is a simple method of cutting the band that prevents the movement of the tongue. In frenuloplasty, in addition to cutting, a limited separation is made in the genioglossus muscle and a horizontal or vertical repair is made. Frenotomy is the most common technique used in infants and is a simple, short, and safe method. It can be performed with local anesthesia or without anesthesia. 18,19 The frenotomy and frenuloplasty operations performed in ankyloglossia surgery are very safe. The most common complication of these procedures is recurrence due to scar formation. Postoperative hemorrhage, infection, and tongue edema have been reported in a few cases in the literature. 10
In a study by Dollberg et al involving 25 infants between the ages of 1 and 21 days, frenotomy decreased pain for the mother and resolved breast-feeding difficulties in infants. In the same study, they reported that none of the patients had any side effects related to the frenotomy, and there was not more than a few drops of external bleeding during the procedure. 4
In a study conducted by Griffiths, 215 infants ranging in age from 0 to 19 days underwent frenotomy, and no significant complication was reported in any of the patients. In the same study, improvement was observed in the first 24 hours in feeding in 80% of patients following frenotomy. 20
Hong et al applied frenotomy to 322 patients aged between 1 day and 24 weeks and reported a revision rate of 3.7%. 21 In our case series, only 9 patients were given revisions. No patient was readmitted to the hospital due to postoperative bleeding, infection, or other complications.
Our study has some limitations. The study being retrospective, the absence of the ankyloglossia grading and the inability to measure the change in symptoms due to ankyloglossia after frenotomy are the disadvantages of the study.
Conclusion
In our study, the incidence of ankyloglossia in male and female patients was found correlate with the studies conducted in Turkey and different countries in the literature. These results indicate that ankyloglossia is more common in males, and there is no racial predilection. Ankyloglossia surgery can be performed in newborns from the first day of life. Frenotomy is a minimally invasive surgical procedure with high efficacy. There is no difference in terms of morbidity or surgical success between performing surgery in the infant period or late period. The correction of ankyloglossia in early ages reduces the risk of subsequent complications. Therefore, surgery should be considered at the time when ankyloglossia is detected due to the patient’s speech, nutrition, or mechanical / social difficulties.
Footnotes
Authors’ Note
Ethical Adherence: Ethics Committee of the KTO Karatay University, School of Medicine (02.11.2018/008).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.