
Abstract
Deep neck infection (DNI) refers to infections in spaces created by superficial and deep cervical fascia around the muscles and organs in the neck. Vitamin D is highly important for an effective immune system. Vitamin D receptors (VDR) have been identified in immune system cells, and particularly in T and B lymphocytes, macrophages, and dendritic cells. Vitamin D deficiency is thought to result in impaired immune response, decreased leukocyte chemotaxis, and an increased disposition to infection. The purpose of this study was to investigate whether vitamin D deficiency is an underlying occult factor in the development of DNI. Sixty-five patients aged 6 to 90, diagnosed with DNI, and 70 healthy age- and sex-compatible cases were included in the study. Serum levels of calcium, phosphorus, parathyroid hormone, and 25-hydroxy vitamin D (25(OH)D) were determined in each case. 25-hydroxy vitamin D levels above 20 ng/mL were regarded as normal, 12 to 20 ng/mL as insufficient, 5 to 12 ng/mL as deficient, and less than 5 ng/mL as severely deficient. Mean serum 25(OH)D levels were 10.4 (6.2) ng/mL in the patient group and 15.5 (6.4) ng/mL in the control group (P < .01). This difference was statistically significant (P < .01). Vitamin D was within normal limits in 9.2% (n = 6) of cases in the study group, insufficient in 29.2% (n = 19), deficient in 35.3% (n = 23), and severely deficient in 26.2% (n = 17). The equivalent values in the control group were 21.4% (n = 15), 48.5% (n = 34), 30% (n = 21), and 0% (n = 0). Serum 25(OH)D levels were significantly lower in patients with DNI compared to the healthy cases; 25(OH)D levels may be a factor in the development of DNI.
Introduction
Deep neck infection (DNI) is defined as infection of potential spaces and fascial planes of the neck. Depending on their anatomical location, these infections are classified as submandibular, submental, peritonsillar, retropharyngeal, pretracheal, parapharyngeal, or anterior visceral. 1 Although the morality rate associated with DNIs has decreased due to widespread use of antibiotics, advanced diagnostic tests, and early surgery, they continue to cause severe and potentially life-threatening complications. These include airway obstruction, deep vein thrombosis, descending mediastinitis, laryngeal edema, and acute respiratory distress. 2 Deep neck infections most commonly derive from dental and upper airway infections. Other etiological causes include lymphadenitis, foreign body traumas, and intravenous drug use. Deep neck infections are typically seen in participants with a history of diabetes, immunosuppression, radiotherapy or chemotherapy, or with HIV and alcohol dependence. However, DNI can also develop in individuals experiencing dental or upper airway infection without these exacerbating factors. The fact that DNI does not develop in all individuals experiencing dental or upper airway infection led us to question the possibility of another underlying etiological factor. We therefore investigated the effect of vitamin D, of critical importance to immune response.
Vitamin D has been shown to be very important for an effective immune system. Vitamin D receptors (VDR) have been identified in immune system cells, and particularly in T and B lymphocytes, macrophages, and dendritic cells. It is thought that in vitamin D deficiency, immune response is impaired, leukocyte chemotaxis decreases, and disposition to infection increases. 3
The purpose of this study was to investigate whether vitamin D deficiency is an underlying occult factor in the development of DNI, by comparing vitamin D levels in patients with DNI and those of a control group.
Materials and Methods
This randomized, single-blind, case–control study was performed at the Ataturk Univeristy, Faculty of Medicine Department of Ear Nose and Throat, after receipt of local ethical committee approval with number 2018:4:9. Consent was obtained from all participants or their families.
In our pilot study, we observed a difference of 5 between the 2 groups in terms of vitamin D levels. The number of individuals required in each group based on 99% power, and a .05 α value with the Russ Lenth Piface Java Module was calculated at 65.
Patients diagnosed with DNI and under monitoring by the ENT Department were included in the study. The control group consisted of healthy participants compatible with the patient group in terms of age and sex. Deep neck infection diagnosis was based on physical examination and radiological imaging findings. Participants with a history of chronic drug use, alcohol use, or kidney or liver disease or with diffuse dermatological disease were excluded from the study. Patients’ age, sex, and location of DNI were recorded. All patients received the requisite urgent medical and surgical therapy.
Venous 10 mL blood specimens were collected from all participants at time of diagnosis, and calcium, phosphorus, parathyroid hormone, and 25-hydroxy vitamin D (25(OH)D) levels were determined in each case.
Serum 25(OH)D levels above 20 ng/mL were regarded as normal, 12 to 20 ng/mL as vitamin D insufficiency, 5 to 12 ng/mL as vitamin D deficiency, and <5 ng/mL as severe vitamin D deficiency. 4 Vitamin D levels as well as calcium, phosphorus, and parathyroid hormone levels were compared between the patient and control groups.
SPSS 17.0 software was used for statistical analysis. Distribution of all data was examined using the Shapiro-Will test. Categorical variables were expressed as percentages, and quantitative data as mean (standard deviation). As the distribution was normal, Student t test was used in analysis. The χ2 test was used to analyze categorical data. P values < .05 were regarded as statistically significant in all methods.
Results
Sixty-five patients aged between 6 and 90 (30 [17]) and a control group consisting of 70 healthy individuals aged between 12 and 72 (34.6 [13]) were included in the study. The patient group consisted of 35 males and 30 females, and the control group of 33 males and 37 females. There was no significant difference between the 2 groups in terms of age or sex (P = .08, and P = .43, respectively).
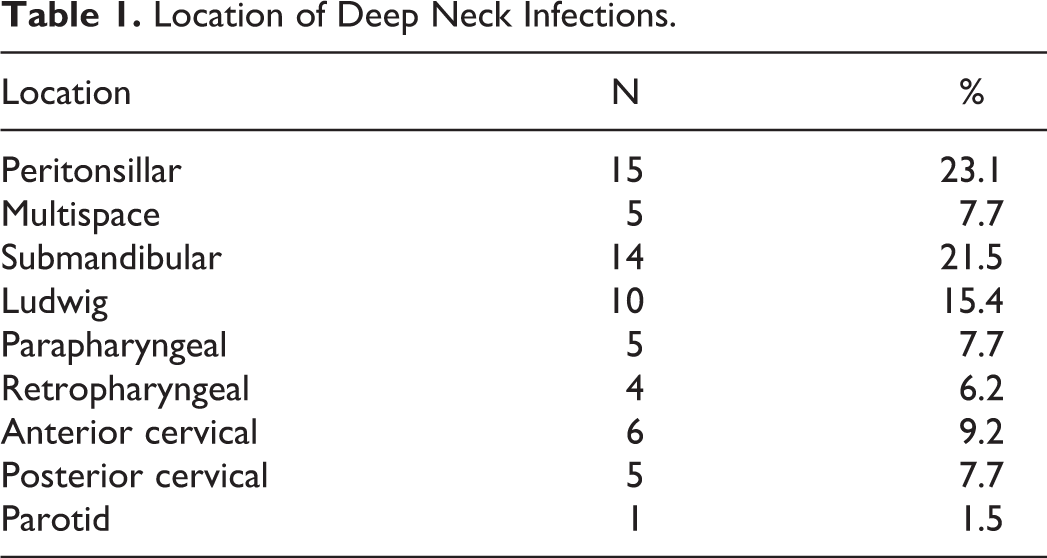
The most common site of infection in the patient group was the peritonsillar region, followed by the submandibular area. Infection sites are summarized in Table 1.
Location of Deep Neck Infections.
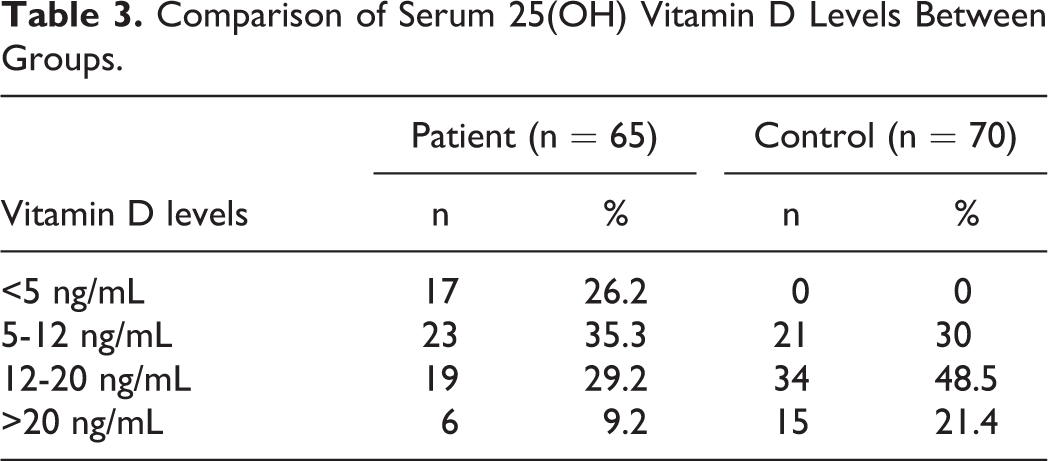
Mean 25(OH)D levels were 10.4 (6.2) in the patient group and 15.5 (6.4) in the control group. This difference between the 2 groups was statistically significant (P < .001). Biochemical results are summarized in Table 2. Severe vitamin D deficiency was observed in 26.2% of the study group, deficiency in 35.3%, and insufficiency in 29.2%, with normal vitamin D levels being determined in 9.2%. The equivalent values in the control group were 0%, 38%, 48.5%, and 21.4%. Vitamin D distributions in both groups are shown in Table 3.
Comparison of Laboratory Parameters Between Study and Control Cases.
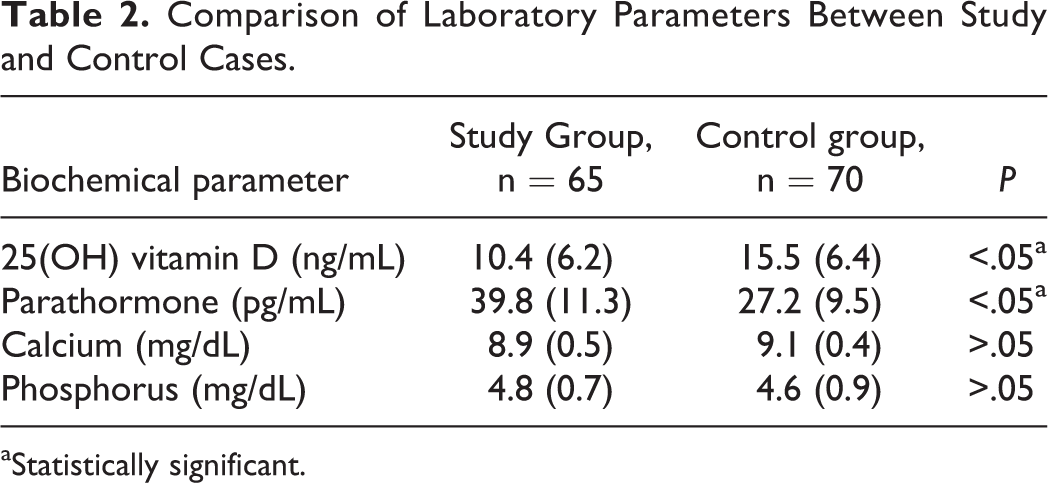
aStatistically significant.
Comparison of Serum 25(OH) Vitamin D Levels Between Groups.
Discussion
Vitamin D, also known as the “sunshine vitamin,” is not only a vitamin but also a prohormone with several functions in the body. 5 There are 2 major forms of vitamin D; these are vitamin D2, known as ergocalciferol, and vitamin D3, known as cholecalciferol. Vitamins D2 and D3 can be synthesized from the skin as a result of exposure to ultraviolet radiation or can also be ingested via various foodstuffs. The level of vitamin D manufactured by the skin represents a large part of total production and is affected by various factors. These include a dark skin coloring, limited exposure to sunlight due to geographical location, and type of clothing worn. The region where our study was performed has a cold climate, and people have to spend much of the year covered up, and this impacts on vitamin D levels. The basic function of vitamin D is to contribute to the development and continuity of the skeletal system through calcium uptake through the intestines. In addition to the skeletal system, it also has effects on the heart, prostate, stomach, brain, and T and B lymphocytes. These tissues contain vitamin D receptors, and vitamin D is thought to play a role in immune system regulation and reducing inflammation by means of these receptors. 6
Vitamin D exhibits regulatory effects on the immune system and inflammatory cascade. It increases VDR expression when the majority of VDR cells are stimulated. Increasing VDR expression raises vitamin D uptake into the cells. Increasing intracellular vitamin D increases the production of several chemokines and cytokines, such as interleukin-6, interleukin-12, and tumor necrosis factor-α. 7 It also increases the production of the antimicrobial peptides cathelicidin and β defensins that are found widely in the body and play a role in immunity with their chemotactic activity and toxin-neutralizing properties. 8
Several studies have shown that vitamin D deficiency can prepare the ground for various infectious diseases. Cayir et al determined a significant decrease in serum calcitriol levels in children diagnosed with acute otitis media (AOM) and reported that vitamin D deficiency plays a significant role in the risk of AOM. 9 Yildiz et al determined lower levels of vitamin D in children with recurring pharyngotonsillitis compared to healthy children and reported that low vitamin D levels may constitute a risk factor for recurring pharyngotonsillitis. 10 Another study revealed that recurring tonsillopharyngeal infections in adults were linked to vitamin D deficiency. 11 Studies have also investigated the association between vitamin D deficiency and lower airway infections, bronchiolitis, pneumonia, and sinusitis. 8 However, no previous studies have investigated the association between vitamin D levels and DNIs.
Deep neck infections have the potential to spread rapidly and cause complications due to the complex links between the fascia and compartments of the neck. Since these complications can be life-threatening, the early diagnosis and treatment of DNI is of very great importance. Previous studies in the literature have generally reported etiological causes of DNI in specific patient groups, the demographic characteristics of patient groups, the neck compartments affected, the agent microorganisms involved, and various complications arising. No vitamin or similar substance increasing the tendency to or underlying DNI has to date been investigated. The present study investigates vitamin D deficiency as a suspected factor increasing disposition to DNI. We determined significantly lower vitamin D levels in patients with DNI compared to the control group. Appropriate doses of vitamin D supplementation were administered to patients with vitamin D deficiency. No recurrence was observed in our patients during 1-year follow-up.
Conclusion
We determined significantly lower levels of vitamin D in patients with DNI compared to healthy individuals. Vitamin D deficiency may be involved in the development of DNI. We therefore think that, in addition to the requisite medical and surgical procedures in patients with DNI, checking vitamin D levels and administering replacement in case of deficiency will reduce the incidence of DNI that may recur in later life.
Footnotes
Authors’ Note
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.