
Abstract
Rhinogenous optic neuritis, which causes neuropathy associated with visual dysfunction, greatly reduces patient quality of life and requires suitable early treatment. This study aimed to analyze visual outcome predictors in patients with rhinogenous optic neuritis and to develop and investigate the usefulness of an algorithm to facilitate early treatment. Prospective and retrospective investigations were conducted at the Department of Otorhinolaryngology. The visual outcomes after sinus surgery of 24 of 53 patients suspected of having rhinogenous optic neuritis were analyzed. Furthermore, the usefulness of the treatment algorithm was evaluated in 27 of these 53 patients. Data from 24 patients who underwent surgery were included in a multiple regression analysis to investigate the associations between visual outcomes and concomitant symptoms and the time from symptom onset to surgery. The mean time from the initial examination to a request for otorhinolaryngological examination to assess the usefulness of the treatment algorithm was compared in 27 patients who did not undergo an initial otorhinolaryngological examination. Visual acuity improved in 23 participants who underwent surgery. Multivariate analysis identified the time from onset to surgery and headache as significant predictors of postoperative visual acuity. The mean time from the initial examination to a request for otorhinolaryngological examination was significantly shorter after the algorithm was introduced (1.13 days, 8 patients; P = .008). Early surgical treatment is essential to avoid further postoperative visual acuity decreases in patients with rhinogenous optic neuritis. Patients who experience headache may have poorer postoperative outcomes.
Introduction
The paranasal sinuses are adjacent to the orbits, optic nerve, and cavernous sinus. Therefore, the spread of inflammation and pressure in the paranasal sinuses causes neuropathy of the optic and oculomotor nerves, resulting in the manifestation of symptoms such as visual disturbance, diplopia, ocular motility disorders, eye pain, headache, eyelid swelling, and ocular deviation. Rhinogenous optic neuritis, which results in neuropathy associated with visual dysfunction, greatly reduces a patient’s quality of life. Accordingly, suitable early treatment is required.
Currently, surgical therapy and conservative therapy with antibiotics and steroids are the 2 options available for the treatment of rhinogenous optic neuritis. Surgical therapy aims to drain inflammation and releases the pressure on the optic nerve. Although surgical treatments are often performed by an otorhinolaryngologist, the initial examination for visual disturbance, a common early symptom of rhinogenous optic neuritis, is often conducted by an ophthalmologist. Therefore, failure to consult an otorhinolaryngologist promptly after the initial examination may delay surgical intervention and affect the outcomes.
To facilitate the early diagnosis of rhinogenous optic neuritis and multidisciplinary surgical intervention and treatment, we introduced our newly developed rhinogenous optic neuritis treatment algorithm in our department in January 2017 (Figure 1). In this study, we examined the usefulness of this algorithm as well as the predictors of rhinogenous optic neuritis.
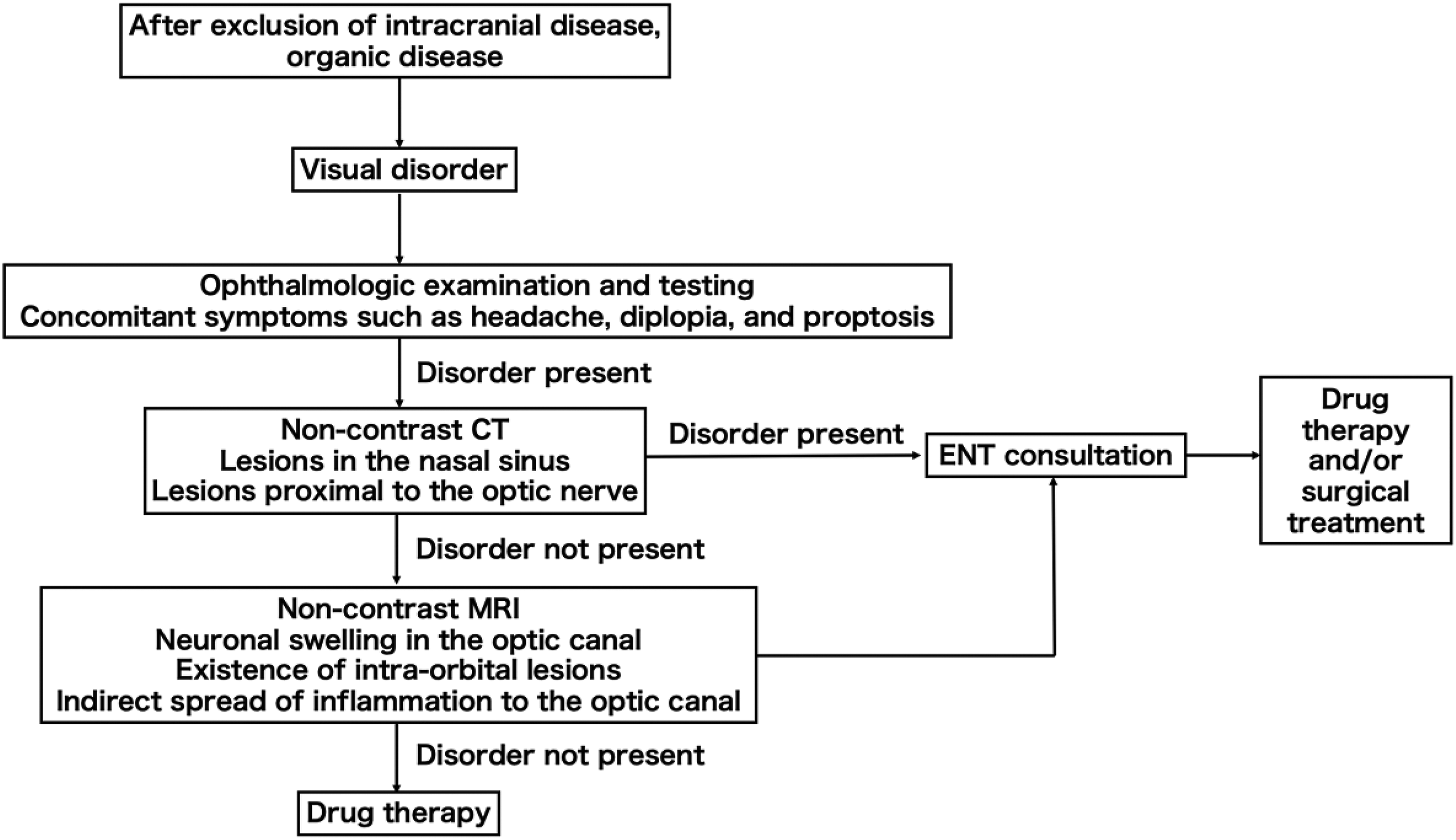
Treatment algorithm for rhinogenous optic neuritis. CT indicates computed tomography; ENT, ear, nose, and throat; MRI, magnetic resonance imaging.
Patients and Methods
The current study was approved by the appropriate institutional review board. Fifty-three patients were examined at the Department of Otorhinolaryngology due to suspicion of rhinogenous optic neuritis between January 2011 and January 2018. We applied the existing definition of rhinogenous optic neuritis as damage to the optic nerve caused by ipsilateral sinusitis, cysts, or mucoceles in the paranasal sinus or orbital cellulitis, orbital abscess, or subperiosteal abscess of the orbit adjacent to the optic nerve. 1 Of these 53 patients, 24 who underwent surgery for sinusitis (acute sinusitis, acute exacerbation of chronic sinusitis, orbital abscess, and subperiosteal abscess of the orbit), and paranasal sinus mucoceles were selected as participants in the present study. Fifteen and 9 of these participants were male and female, respectively, and their ages ranged from 15 to 84 years (median, 57.8 years). Eleven participants had paranasal sinus mucoceles (primary paranasal sinus mucoceles, 7; postoperative mucoceles, 4) and 13 had sinusitis. Patients who lacked light perception at the time of the examination were excluded because of the relative absence of evaluable visual function. Patients who had not undergone a postoperative examination and those with immune diseases such as comorbid tumor lesions, eosinophilic sinusitis, and antineutrophil cytoplasmic antibody–associated diseases were also excluded.
All patients underwent endoscopic sinus surgery (ESS) and subsequently received antibiotics (ampicillin/sulbactam 6 or 12 g or second-generation cephalosporins for 5 days) and steroid therapy (methylprednisolone sodium succinate 1 g for 3 days or hydrocortisone sodium succinate 500 mg for 5 days). During ESS, the entire paranasal sinus was opened to release pressure on the infraorbital optic nerve and optic canal, relieve optic nerve inflammation, and enable effective postoperative nasal irrigation. In cases with an orbital abscess or subperiosteal abscess of the orbit, Draf IIb procedures were performed and the abscess was drained by removing the medial wall of the orbit and making a periorbital incision. Our department used the following indications for optic nerve decompression or optic nerve sheath incision: rhinogenous optic neuritis with localized bone breakdown around the optic nerve canal, concomitant optic nerve canal fracture, and idiopathic optic neuritis resistant to conservative therapy.
The usefulness of our treatment algorithm was examined as follows. In the initial pool of 53 patients, 27 who were suspected of having rhinogenous optic neuritis based on an initial examination were identified; of these patients, some were subsequently deemed not to have the condition. The initial examinations were not performed by an otorhinolaryngologist. Nineteen and 8 of the 27 patients were examined before and after the introduction of our algorithm, and the times to otorhinolaryngological examination in each group were compared.
For the statistical analysis, the decimal visual acuity (d) assessed using Landolt rings, a standard unit of visual acuity used in Japan, was converted to the logarithm of the minimum angle of resolution (logMAR) as follows: logMAR = log (1/d), logMAR = −log (d).
Finger counting, hand motion, light perception, and no light perception cannot be represented as (d) and were calculated as 1.9, 2.3, 2.7, and 3.0, respectively, in accordance with a previous study. 2 The values were calculated to the second decimal place. Recovery of visual acuity was defined as an improvement of ≥2 lines in logMAR. Multiple regression analyses were conducted to examine the associations of visual outcomes with age, sex, visual field defects, diplopia, headache, and time from onset to surgery and thus determine whether the recovery of vision was associated with subjective symptoms in the initial examination and/or patient demographics. The level of statistical significance was set at a P value < .05. Statistical analyses were conducted using SPSS version 24 (IBM, Armonk, New York).
Results
Table 1 presents the background and symptom data of the 24 participants who underwent ESS. Optic nerve decompression was not indicated in any patient. Aside from visual disturbance, the symptoms included visual field defects (n = 15), diplopia (n = 4), and headache (n = 7). The time from onset to surgery ranged from 1 to 88 days (median: 14 days), with a mean of 23.5 days. The mean preoperative logMAR was 1.15.
Clinical Data of the Patients With Rhinogenous Optic Neuritis.
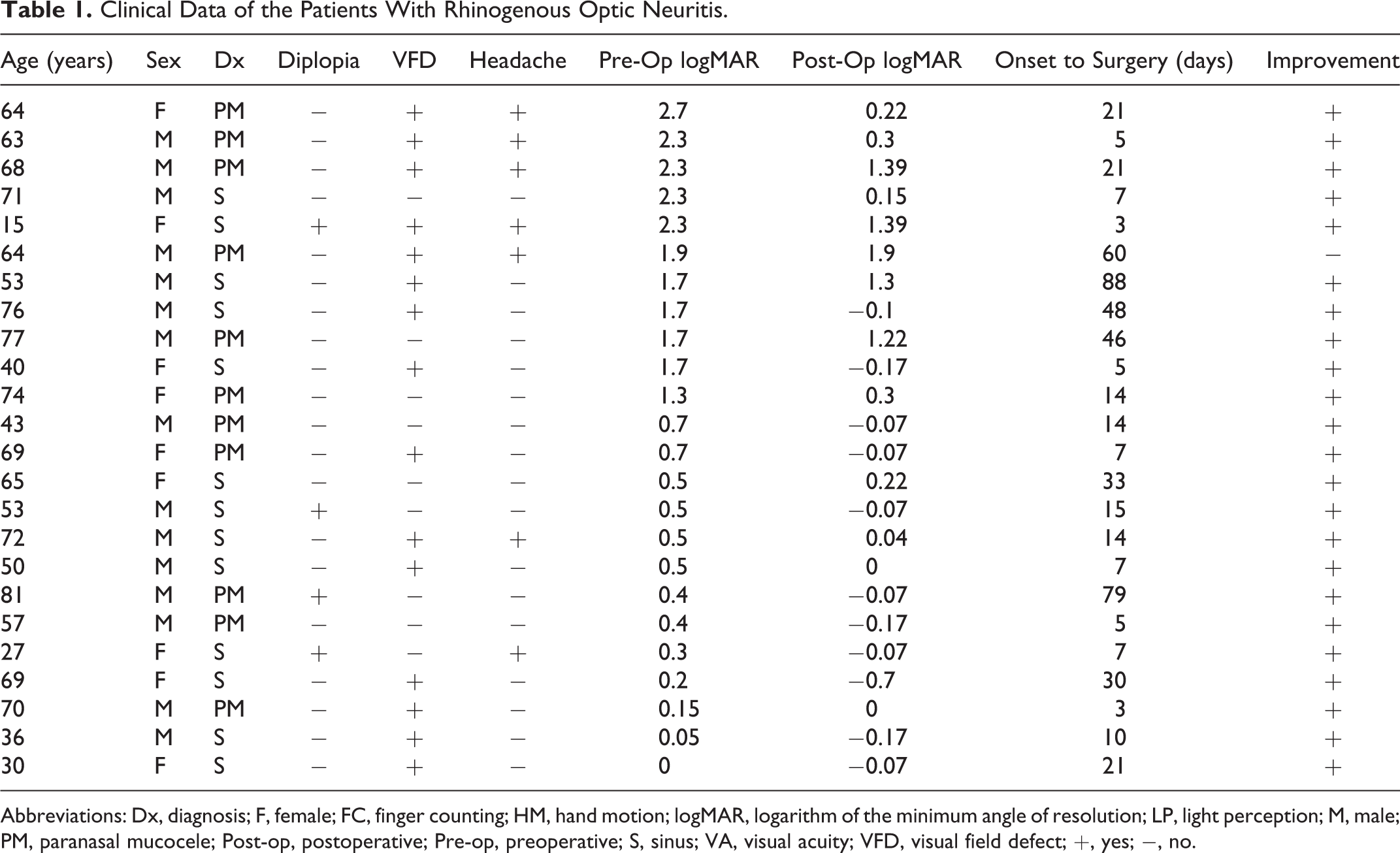
Abbreviations: Dx, diagnosis; F, female; FC, finger counting; HM, hand motion; logMAR, logarithm of the minimum angle of resolution; LP, light perception; M, male; PM, paranasal mucocele; Post-op, postoperative; Pre-op, preoperative; S, sinus; VA, visual acuity; VFD, visual field defect; +, yes; −, no.
Visual acuity improved in 23 (96%) of 24 participants who underwent surgery; 1 (4%) participant experienced no change in visual acuity. The mean preoperative logMAR was 1.12 in 23 participants with improved visual acuity and 1.90 in 1 participant with no change. The mean time from onset to surgery was 21.9 days in the 23 participants with improved visual acuity and 60 days in the participant with no change. All 13 participants with sinusitis and 10 (90.9%) of 11 participants with paranasal sinus mucoceles exhibited improvements in visual acuity. The mean preoperative logMAR values were 0.94 and 1.32 in participants with sinusitis and paranasal sinus mucoceles, respectively (P = .934, Student t test).
In the multivariate analysis of the relationships of postoperative visual acuity with the time from onset to surgery and concomitant symptoms, the time from onset to surgery (P = .014, 95% confidence interval [CI]: 0.003-0.023) and headache (P = .008, 95% CI: 0.239-1.378) was identified as significant factors (Table 2). However, postoperative visual acuity was not significantly associated with age or sex. The mean time from examination at another department to consultation with an otorhinolaryngologist was significantly shorter after the introduction of our algorithm (1.13 days, 8 patients) than before (11.16 days, 19 patients; P = .008, Student t test, Figure 2). Of the 8 patients assessed after the introduction of the algorithm, 5 were diagnosed with rhinogenous optic neuritis (Table 3).
Multiple Regression Test.
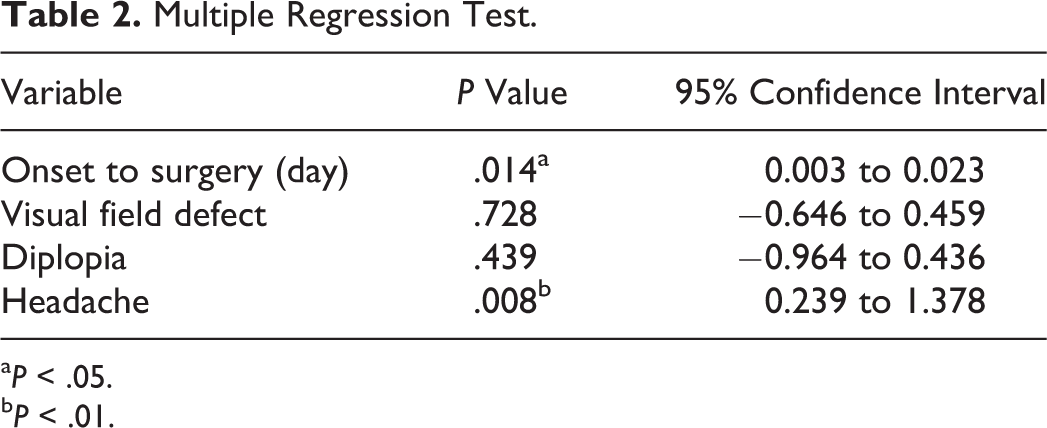
a P < .05.
b P < .01.
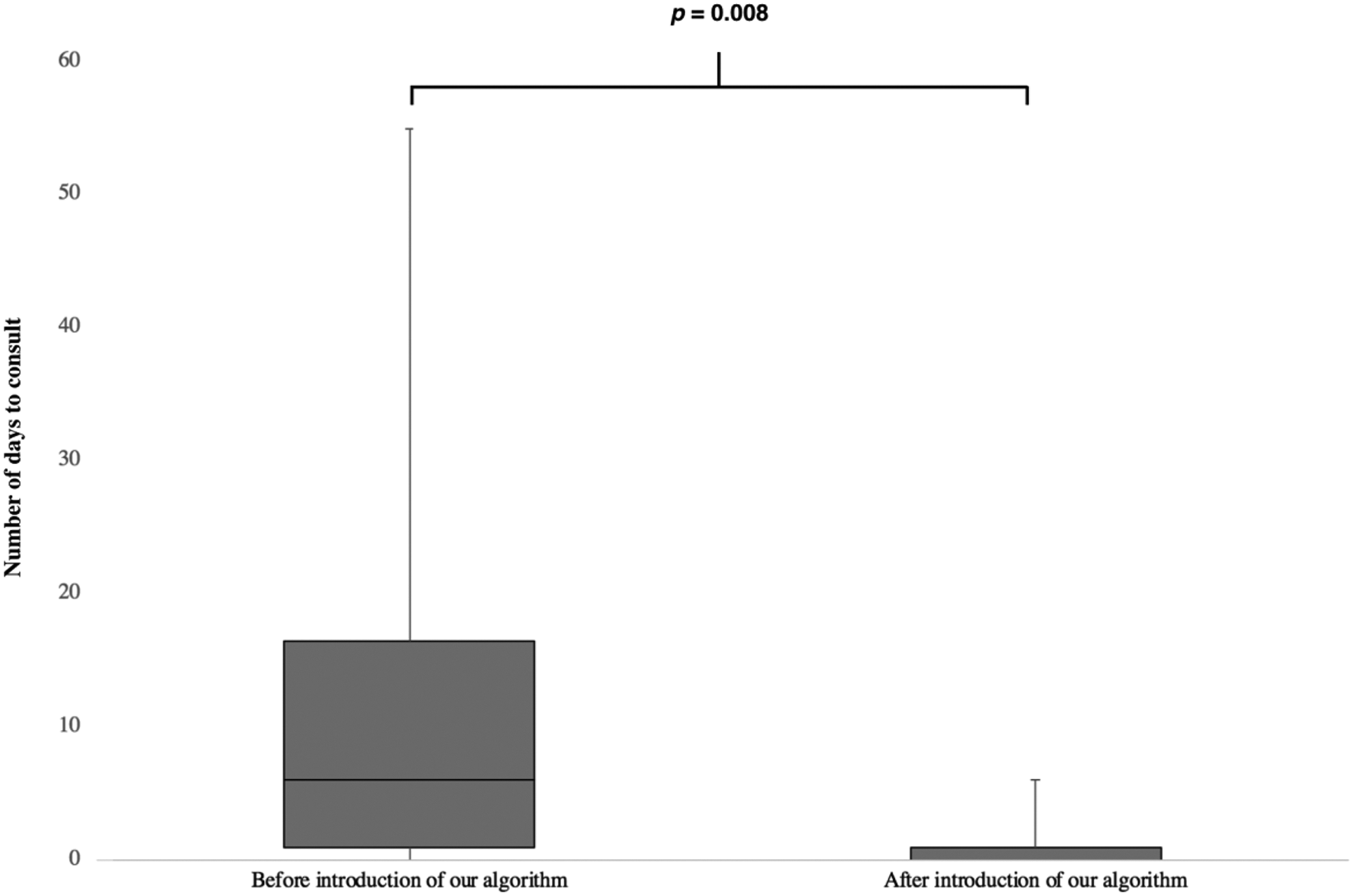
Comparison of the numbers of days to consultation with an otolaryngologist reported before and after the introduction of the algorithm. *Student t test.
Cases and Diagnoses After the Introduction of the Algorithm (Including MRI Findings).
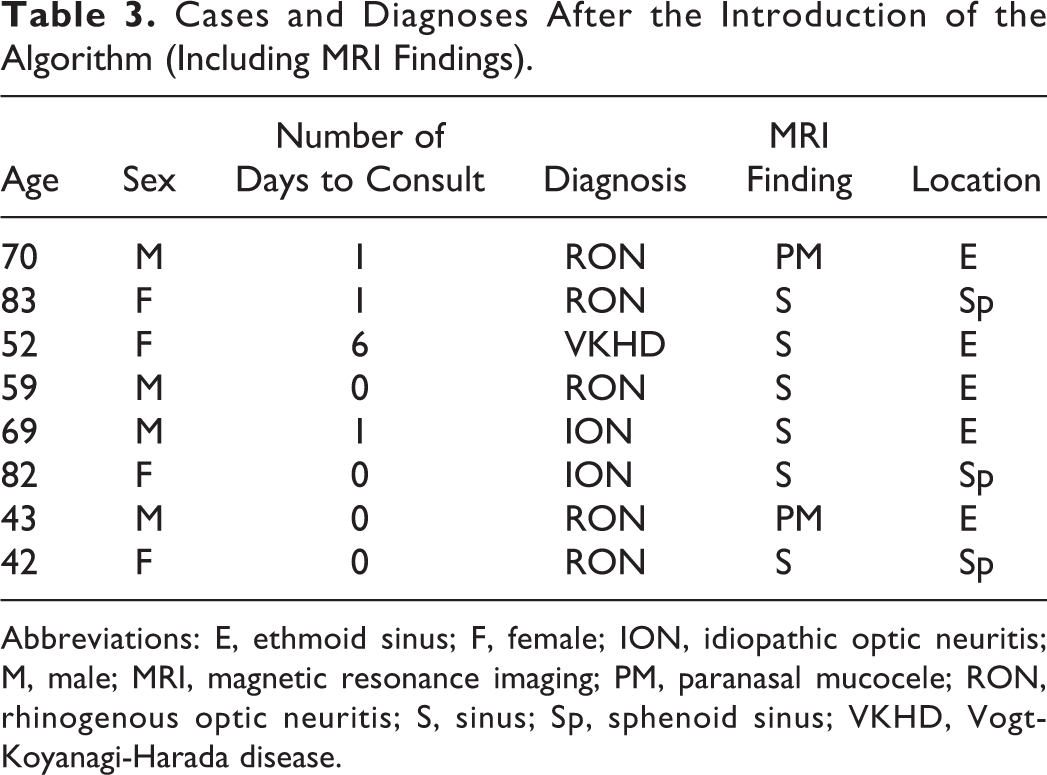
Abbreviations: E, ethmoid sinus; F, female; ION, idiopathic optic neuritis; M, male; MRI, magnetic resonance imaging; PM, paranasal mucocele; RON, rhinogenous optic neuritis; S, sinus; Sp, sphenoid sinus; VKHD, Vogt-Koyanagi-Harada disease.
Discussion
Rhinogenous optic neuritis describes the manifestation of visual field defects, ocular motility disorder, and visual disturbance associated with paranasal sinus disease. Various theories regarding the mechanism by which paranasal sinus disease causes visual disturbance have been proposed. The 3 most convincing theories involve optic neuritis due to an adjacent inflammatory process, venous congestion of the optic nerve due to increased infraorbital pressure or thrombophlebitis within the valveless orbital veins, and increased infraorbital pressure resulting in occlusion of the central retinal artery. 3,4 Although visual disturbance is typically induced by acute sinusitis and paranasal sinus mucoceles, reports have also described visual disturbances induced by conditions such as allergic fungal sinusitis and Wegener granulomatosis (ie, granulomatosis with polyangiitis). 5,6 Although visual disturbances induced by acute sinusitis are often irreversible, 7,8 decompression of the mucocele is considered to yield favorable outcomes in cases involving paranasal sinus mucoceles. 4 Notably, in the current study, visual acuity improved in all participants with sinusitis and in 10 (90.9%) of 11 participants with paranasal sinus mucoceles.
As noted previously, rhinogenous optic neuritis can be treated surgically or conservatively. In a previous study by Beck and Gal 9 that compared intravenous steroids, oral steroids, and a placebo for the treatment of optic neuritis, oral steroids were associated with more frequent recurrence, and the only significant difference in vision recovery was observed between the placebo group and intravenous steroid group. In our department, steroids are administered intravenously to all patients.
In a meta-analysis of 85 reports (comprising a collective total of 207 patients) on visual disturbance involving paranasal sinus mucoceles, a time from onset to surgery of <6 days was associated with improved visual acuity outcomes, indicating the importance of early surgical intervention. 2 Moriyama et al 10 also noted that in patients exhibiting a gradual progression from mild to moderate visual disturbance, the recovery of visual acuity depends on the time from onset to surgery. In the current study, the time from onset to surgery for rhinogenous optic neuritis was identified as a significant predictor of postoperative visual acuity. This finding underscores the importance of early surgical therapy for rhinogenous optic neuritis induced by sinusitis and paranasal sinus mucoceles.
The optic nerve is unmyelinated within the globe of the eye but becomes covered by a central myelin sheath produced by oligodendrocytes upon exiting the globe. Although the optic nerve is a cranial nerve, histologically, it is considered part of the central nervous system. Although regeneration is unlikely in cases of severe damage, vision may be recoverable if the optic nerve has not become completely necrotized and irreversibly damaged. Therefore, surgical therapy should be administered early. In a previous study, early surgery led to recovery of vision (including hand motion and counting fingers) even in severe cases, 2 while another study found that if performed within 24 hours, surgery enabled the recovery of vision even in patients with no light perception. 10 Still, multiple factors associated with acute bacterial inflammation in the paranasal sinus cause rapid inflammation of the optic nerve, and the associated visual loss is occasionally irreversible. 4 Therefore, inflammatory visual loss may require particularly prompt drainage.
At our hospital, we created a treatment algorithm focused on early surgical intervention and the administration of steroids and antibiotics in cooperation with the ophthalmology department, where the initial examinations are often conducted. If visual disturbance is found to be accompanied by symptoms such as exophthalmos or headache, the patient will undergo ophthalmological examination and testing, as well as computed tomography of the paranasal sinuses, to check for the presence of intracranial lesions and lesions around the optic canal. The otorhinolaryngology department is promptly consulted if lesions are detected in the paranasal sinuses surrounding the optic canal or in the orbit, while the neurosurgery department is promptly consulted if intracranial lesions are detected. Emergency surgery is performed if there is an apparent association between the sinus lesions and visual disturbance.
Since its introduction, our algorithm has dramatically reduced the time from the initial examination in another department to examination in the otorhinolaryngology department, thereby facilitating earlier surgical intervention. However, it has been difficult to reduce the time from onset to examination at the otorhinolaryngology department. Therefore, we must educate not only other clinicians and patients in our own hospital but also those at nearby ophthalmology clinics.
Patients with rhinogenous optic neuritis accompanied by headache may have poor outcomes. In the current study, preoperative physical symptoms, examination findings, and visual acuity were examined, leading to the identification of a significant difference pertaining to headaches. In paranasal sinus disease, mucosal inflammation in the paranasal sinuses irritates the trigeminal nerve or meninges to cause pain. 10 Anatomically, the entrance of the optic canal is formed by the 3 meningeal layers (dura mater, arachnoid mater, and meninges of the middle cranial fossa), while an optic nerve sheath is formed around the optic nerve axon in the orbit. Therefore, the spread of meningitis not only causes optic neuritis but also episcleritis, orbital apex syndrome, orbital myositis, and orbital keratitis. 11 The spread of localized inflammation beyond the paranasal sinus to the dura mater and optic nerve results in visual disturbances and is believed to trigger headaches via the same mechanism. Thus, a headache may indicate that inflammation has spread beyond the paranasal sinuses. Moriyama et al 10 reported that 16 (64%) of 25 patients with paranasal sinus mucoceles with visual disturbance also reported experiencing pain. 10 As headache is a subjective symptom, related information can be obtained via diagnostic interviews, without the need for complex tests or instruments. Therefore, information pertaining to headaches may be crucial for determining the need for surgery when the initial examination is performed at night or in any other setting where testing is not possible.
Conclusion
Rhinogenous optic neuritis may cause blindness and, therefore, requires rapid diagnosis and treatment via multidisciplinary examinations. Early surgical therapy has yielded improvements in vision even in severe cases (no light perception or worse). However, patients with rhinogenous optic neuritis accompanied by headache may have poor postoperative outcomes. Finally, the introduction of our rhinogenous optic neuritis treatment algorithm at our hospital resulted in the earlier administration of surgical interventions by our otorhinolaryngology department.
Footnotes
Authors’ Note
All procedures were in accordance with ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Written informed consent was obtained by every patient. Institutional Board approval was obtained.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.