
Abstract
The objective is to report 3 cases of vocal fold cysts treated with thulium laser in an office setting under local anesthesia. The surgical technique, which consists of surgical marsupialization, is described in detail with emphasis on the laser setting. All 3 patients had complete regression of the lesion and marked improvement in voice quality and good closure of the vocal folds during phonation. The authors review the literature on the application of laser therapy in an office setting and advocate this as an alternative treatment option for patients with vocal fold cysts who are at high risk for general anesthesia or unwilling to undergo the conventional microsurgery.
Introduction
Vocal fold cysts are well-localized subepithelial sac-like structures that arise at the mid-membranous portion of the vocal folds. The etiology is multifaceted and includes infection, phonotraumatic behavior, and/or congenital malformation. Vocal fold cysts can be stratified either as mucus retention cysts ciliated epithelium and containing glandular secretions or as epidermoid cysts with stratified squamous epithelium and containing caseous material. The mucus retention cysts are usually secondary to obstruction to glandular ducts following an upper respiratory tract infection, whereas epidermoid cysts are the result of epithelial cell entrapment following a phonotraumatic behavior or repeated cough. 1,2
Vocal fold cysts account for up to 13% of laryngeal lesions and may lead to vocal symptoms similar to those observed in patients with exudative lesions of the vocal folds. 3,4 Affected patients usually complain of change in voice quality described as diplophonia, vocal instability, and loss of power. These phonatory symptoms are often substantiated by an increase in the acoustic perturbation parameters and a decrease in the fundamental frequency. Aerodynamic measures may show an increase in the mean flow rate and a reduction in maximum phonation time. 4,5 On laryngeal examination, vocal fold cysts are usually unilateral and can be present either on the free edge or the upper lip of the vocal fold. Videostroboscopic examination reveals incomplete glottic closure with a decrease in the mucosal wave on the affected side. If rupture of the cyst occurs, intracordal scarring may develop leading to marked impairment in the vibratory behavior of the vocal folds. Excessive intra- and extralaryngeal muscle tension may be observed as a compensatory behavior. 6
The mainstay treatment of vocal fold cysts is surgical excision using the microflap technique. The surgery aims at total removal of the cyst while preserving the overlying mucosal lining. Steroid injections following excision have been advocated to reduce postoperative inflammation and scar formation. 7 With the reform in laryngology practice toward office-based surgical procedures, laser therapy has gained popularity as an alternative treatment option. The reviews in the literature are primarily confined to lesions like papillomas, polyps, Reinke’s edema, and granulomas with the use of photoangiolytic lasers, 8 –13 which modulate fibroblast proliferation and impair the local microcirculation at the site of the lesion.
The authors of this article report their experience with office-based thulium laser therapy of vocal fold cysts. The details of the procedure and long-term follow-up are described.
Patients and Surgical Technique
Technique
With the patient fully awake and in the upright sitting position, local nasal anesthesia and decongestion were applied to both nasal cavities by placing 1% lidocaine HCl with 1:100 000 epinephrine-soaked sponges. The fiberoptic laryngoscope was then introduced through the nasal cavity and topical anesthesia to the hypopharynx and larynx was then administered by dripping 2% lidocaine HCl while the patient was asked to phonate simulating laryngeal gargle. After complete anesthesia to the laryngeal mucosa was ensured, a 0.55 mm thulium laser glass fiber was advanced through the working channel of the fiberoptic nasopharyngoscope until the tip of the fiber was visualized. The laser beam was applied to the vocal fold cyst overlying mucosa using a pulsed mode, power 4.5 W, duration 70 to 300 milliseconds, repetition 5 Hz, and aiming beam 65%. A 2 to 3 mm mucosal incision was made at the upper surface of the vocal fold cyst following which a suction catheter was introduced into the cavity of the vocal fold cyst and the retained mucus was suctioned (see Figure 1). No complications were encountered during surgery. Following the procedure, patient was instructed to remain nothing (per os and resume oral intake only 1 hour) after the procedure in order to avoid risk of aspiration.

Thulium laser fiberglass in contact with the cyst overlying mucosa.
Case 1
A 40-year-old male patient, 1 pack per day smoker otherwise healthy, presented to the Voice Clinic with the chief complaint of dysphonia and dry cough of 1-year duration. He had a positive history of reflux that was treated with proton pump inhibitors. Patient also had a positive history of phonotraumatic behavior. Perceptual evaluation revealed moderate dysphonia grade 2 and laryngeal examination using the fiberoptic nasopharyngoscope showed a mucus retention cyst at the midmembranous portion of the right vocal fold. Patient elected to undergo unsedated office-based laser therapy as a treatment modality. An office-based laser marsupialization procedure of the vocal fold cyst was performed as described in the section on surgical technique (see Figure 2A and B). On follow-up two years following the procedure, the patient had marked improvement in voice quality with complete regression of the lesion. Laryngeal videostroboscopic examination postoperatively showed adequate malleability and closure of the vocal folds during phonation with normal mucosal wave.
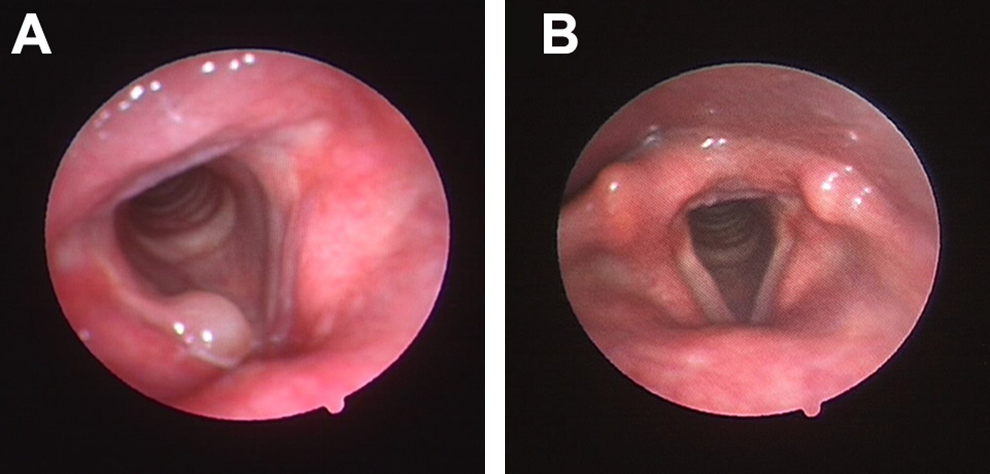
A, Laryngeal endoscopic examination showing right vocal fold cyst. B, Laryngeal endoscopic examination 2 years after the procedure showing complete regression of the right vocal cyst.
Case 2
A 60-year-old female patient, nonsmoker, with history of diabetes mellitus and hypertension presented to the Voice Clinic with a few months’ history of progressively worsening dysphonia. Patient had also history of globus sensation and heartburn. There was no previous history of phonotraumatic behavior or laryngeal manipulation. On perceptual evaluation, patient had dysphonia grade 2 with mild breathiness. Flexible laryngoscopy in clinic revealed a left vocal fold mucus retention cyst (see Figure 3A). On laryngeal videostroboscopy, there was incomplete closure of the vocal folds during phonation with decrease in mucosal waves on the affected side. Patient elected to undergo office-based laser therapy as a treatment modality. An office-based laser marsupialization procedure of the vocal fold cyst was performed as described in the above section on surgical technique. On follow-up 3 months and 1 year after the procedure, patient reported a normal voice. Perceptual evaluation revealed no dysphonia. On laryngeal endoscopic examination, there was complete regression of the lesion (see Figure 3B).
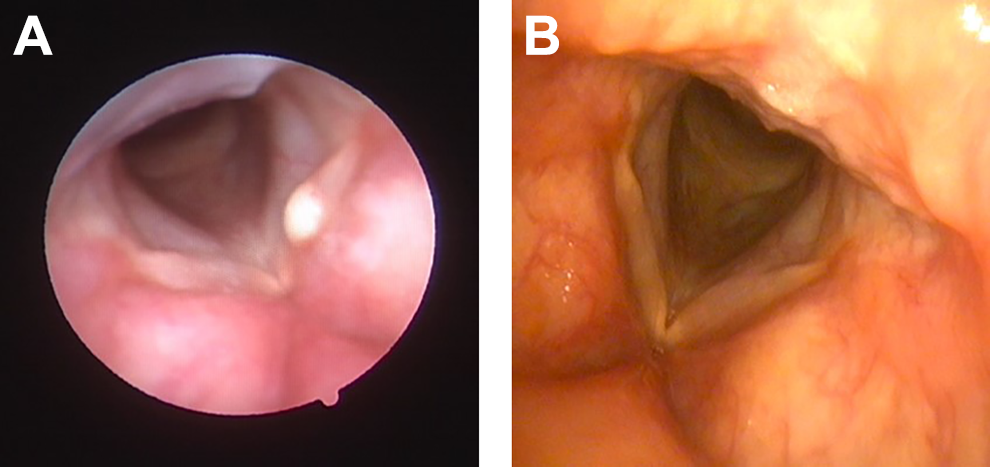
A, Laryngeal endoscopic image showing left vocal fold mucus retention cyst. B, Complete regression of the lesion 1 year following surgery.
Case 3
A 57-year-old male patient with coronary artery disease, hypertension, and diabetes mellitus presented to the Voice Clinic with a long-standing history of dysphonia that has had worsened over the last 2 months. Patient was not a smoker and denied any history of reflux or swallowing symptoms. There was no history of previous laryngeal manipulation or surgeries.
Perceptual evaluation of his voice revealed grade 3 dysphonia with mild breathiness and straining. Laryngeal endostroboscopic evaluation revealed a true left vocal fold mucus retention cyst with incomplete closure of the vocal folds during phonation and decrease in mucosal waves on the affected side (see Figure 4A). In view of his medical condition, patient elected to undergo unsedated office-based laser therapy. The procedure was performed as described in the above section on surgical technique. On follow-up 5 months postsurgery, patient had a normal voice with evidence of complete regression of the lesion and adequate malleability and closure of the vocal folds on laryngeal examination (see Figure 4B).
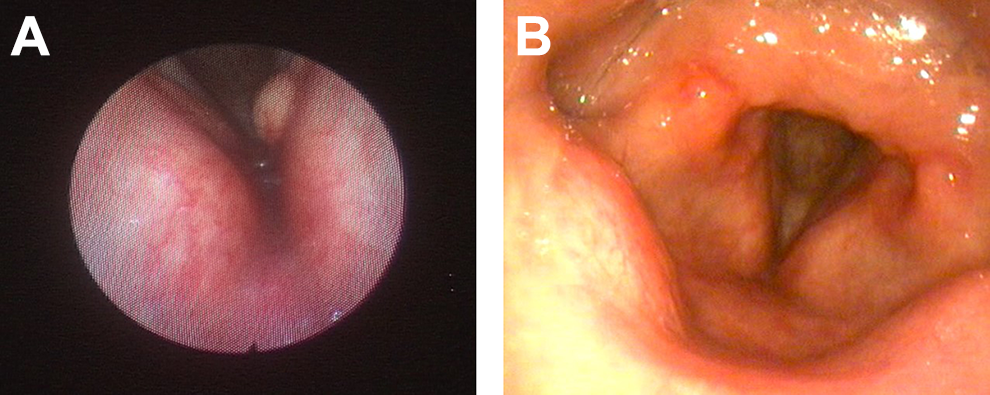
A, Laryngeal endoscopic examination showing left vocal cord cyst. B, Laryngeal endoscopic examination 3 months following surgery showing complete regression of the lesion.
Discussion
Unsedated office-based laser therapy is gaining ground as a viable alternative to phonomicrosurgery in the management of benign and premalignant lesions of the vocal folds. Several authors have reported successful usage of different types of lasers in the treatment of various laryngeal pathologies, most common of which are recurrent respiratory papillomatosis, polyps, granulomas, Reinke’s edema, and less commonly vocal fold cysts. In the multi-institutional review by Sheu et al on the efficacy of potassium titanyl phosphate (KTP) laser in the treatment of benign vocal fold lesions, the authors reported improvement in vocal fold closure and mucosal waves in 90% of the cases. 8 The review included 2 patients with vocal fold cysts out of 102 cases. In another study of 36 cases by Mallur et al on the quantification of benign lesion regression using the KTP laser, the study group included only 1 case of cyst/pseudocyst. 9 In the large review of 443 patients treated with office-based laser surgery by Koufman et al, the case series did not include any case of vocal fold cysts. 10 In the reports by Zeitels et al on the application of different lasers under local anesthesia, the patients were primarily cases of papillomatosis, early carcinoma, supraglottic lesions, and granuloma. 11,12 In the review by Wellenstein et al on office-based laser procedures, the main indications were again respiratory papillomatosis, laryngeal cysts, granulomas, hemorrhagic polyps, and malignant tumors. 13
The scarcity of reports on office-based laser therapy of vocal fold cysts is in keeping with the consensus that total surgical excision of the sac using the standard microflap technique is the mainstay treatment of these lesions. 13 Tibbetts et al have reported successful microflap excision of 21 cases of vocal fold cysts with improvement and/or normalization of mucosal waves in more than 90% of the cases. 14 Similarly, Johns et al have demonstrated significant improvement in self-reported measures in 13 patients who underwent surgical excision of vocal fold cysts. 15 Despite the high success rate of surgical excision using the microflap technique, there are cases where the patient is either at a high risk for general anesthesia or simply is unwilling to undergo the conventional surgery in the operating room. The successful treatment of the reported 3 cases of vocal fold cysts in this review substantiates the potential but not conclusive role of laser therapy in an office-based setting in the management of these patients. The improvement in the self-reported voice quality and perceptual evaluation of all 3 cases of laryngeal cyst in this review can be attributed to the complete regression of the disease and normalization of the vocal fold closure during phonation as shown on fiberoptic endoscopic examination in all 3 cases and to the improvement in the vibratory behavior of the vocal folds as seen in 2 patients (patient 1 and 3). Unlike photoangiolytic laser therapy where the emitted radiation is selectively absorbed by oxyhemoglobin leading to photoablation and regression of the lesion, the effect of the thulium laser is thought to be mediated via nonspecific thermal injury to the targeted tissues. The response, namely complete disappearance of the lesion, may be the result of a nonspecific inflammatory reaction induced by heating of the perivascular stromal tissue. 8
The procedure described within this review falls within the large spectrum of unsedated office-based procedures performed using thulium laser for patients with other exudative lesions of the lamina propria. Koufman et al in 2007 have reported the successful usage of thulium laser in the management of laryngeal cysts, amyloidosis, and granulomas. 10 The authors indicated that thulium laser may be used interchangeably with pulsed dye laser (PDL) in these cases. 10 In that report, the authors described the power setting of PDL as ranging between 0.502.0 J with a mean number of pulses of 236 + 240 and the power setting of flexible carbon dioxide ranging between 8 and 17 W. Zeitels et al have also advocated the usage of thulium laser in the treatment of various laryngeal pathologies in particular laryngeal tumors, with superior hemostatic properties in comparison to the carbon dioxide laser. 11 In their report on office-based application of thulium laser, the power setting was between 4 and 7 W using 0.365 nm fiberglass, which is comparable to the setting we have used in this report. The authors of this article have also previously described the efficacy of in-office thulium laser in the treatment of vocal fold polyps with complete or partial regression in the size of the lesion in all 20 cases. The decrease in the size of the polyps was also associated with improvement in the subjective voice evaluation and self-reported symptoms. 16
This review has 2 main limitations: one is the small number of reported cases (only 3) and second probably the limited duration of follow-up which did not exceed 1 year in one of the 3 cases (patient 3). Nevertheless, this report describes an alternative treatment option to patients with vocal fold cysts. The office-based setting spares the patient the risk of general anesthesia and the well-known morbidity of suspension microlaryngoscopy.
Conclusion
Unsedated office-based laser therapy of vocal fold cysts may be an option for patients who are unable to undergo surgical excision using the conventional microflap technique. Though it is not the treatment of choice, it is advocated for patients with high risk for general anesthesia or those who are unwilling to have undergone conventional microsurgery. Long-term follow-up on a large group of patients will allow better phonatory evaluation of the surgical outcome of such a procedure.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.