
Abstract
Bilateral vocal fold paralysis is a disabling condition that results in airway symptoms, dysphonia, and sometimes difficulty swallowing. Various types of glottal widening procedures have been described in the literature, all of which are performed in the operating room under general anesthesia. The aim is to report laser partial arytenoidectomy as an office-based treatment modality in a patient with bilateral vocal fold paralysis. Using Thulium laser fiber introduced through the working channel of fiberoptic nasopharyngoscope, a posterior cordectomy followed by resection of the vocal process of the right arytenoid was performed. The laser was used in a pulsed mode, power range 3.5 to 4.5 W, duration 70 to 300 milliseconds, repetition 2 to 4 Hz, and aiming beam 65%. The procedure was well tolerated and the patient was successfully decannulated 3 weeks later. Unsedated office-based laser arytenoidectomy might be considered a safe alternative to the commonly practiced glottal widening procedures in patients with a preexisting tracheotomy.
Introduction
Vocal fold–impaired mobility remains to be a common disabling condition encountered in laryngology practice. It is usually secondary either to neurologic or non-neurologic etiologies with the former being more common. Non-neural etiologies include intubation-induced injury, radiation-induced injury, and inflammatory diseases of the cricoarytenoid joint. Neural etiologies include idiopathic viral neuritis, neoplastic lesions, and iatrogenic injury to the vagal or recurrent laryngeal nerve along its course in the neck and chest. 1 -4 Based on a study by Remacle 1996, thyroidectomy still account for up to 58% of vocal fold paralysis. 4 A major vulnerable point to injury is the extralaryngeal splitting of the recurrent laryngeal nerve, the incidence of which varies from 0% to 88% with trifurcation being reported in 34.3% on the left and 65.7% on the right. 5,6
In cases of bilateral recurrent laryngeal nerve injury, airway symptoms often arise in addition to difficulty in swallowing and change in voice quality. Patients invariably complain of shortness of breath, decease in exercise tolerance and stridor. Though many of these patients may recover spontaneously without the need for surgical intervention during the course of a year, a good percentage may require either a tracheotomy to secure the airway or vocal fold suture lateralization as reported by Lichtenberger 1999. 7 Invariably, a glottal widening procedure is mandated as a permanent treatment modality. This latter consists primarily of widening the posterior third of the glottis in order to secure a patent airway. To that end various types of glottal widening procedures have been described in the literature using both external and internal approaches. These include laser arytenoidectomy, 8 laser posterior cordotomy, 9 endoscopic laryngoplasty using microtrapdoor flap with suturing, 10 transverse cordotomy, 11 endoscopic medial arytenoidectomy, 12 subtotal laser arytenoidectomy, 5 laser posterior ventriculocordectomy, 13 and bilateral transverse cordotomy. 14
All the aforementioned surgeries are performed in the operating room under general anesthesia with or without endotracheal intubation. The authors of this manuscript report laser partial arytenoidectomy as an office-based treatment modality in a patient with bilateral vocal fold paralysis.
Case Report
A 54-year-old female nonsmoker presented to the Voice Unit with 1-year history of bilateral vocal fold paralysis following a total thyroidectomy, which necessitated the performance of a tracheotomy with the insertion of Shiley fenestrated tube (size 6). On laryngeal endoscopic examination, patient had fixation of both vocal folds with a 2 to 3 mm glottal chink. She had a breathy phonation with a Voice Handicap Index-10 of 20. Given that the airway was secured via tracheostomy, the patient was offered office-based laser partial arytenoidectomy via the transoral fiberoptic approach. Using Thulium laser power 3.5 to 4.5 watt pulsed mode, a right transverse cordotomy followed by ablation of the posterior third of the vocal fold and vocal process of the arytenoid cartilage were performed under local anesthesia. The patient tolerated well the procedure with no complication. Three weeks postoperatively, patient had marked improvement in her dyspnea with no history of aspiration. The tracheostomy was capped for 48 hours with no shortness of breath. On laryngeal examination, there was widening of the glottal chink posteriorly (see Figure 1). Postoperatively, patient had worsening of her voice with a Voice Handicap Index-10 (VHI-10) of 26.
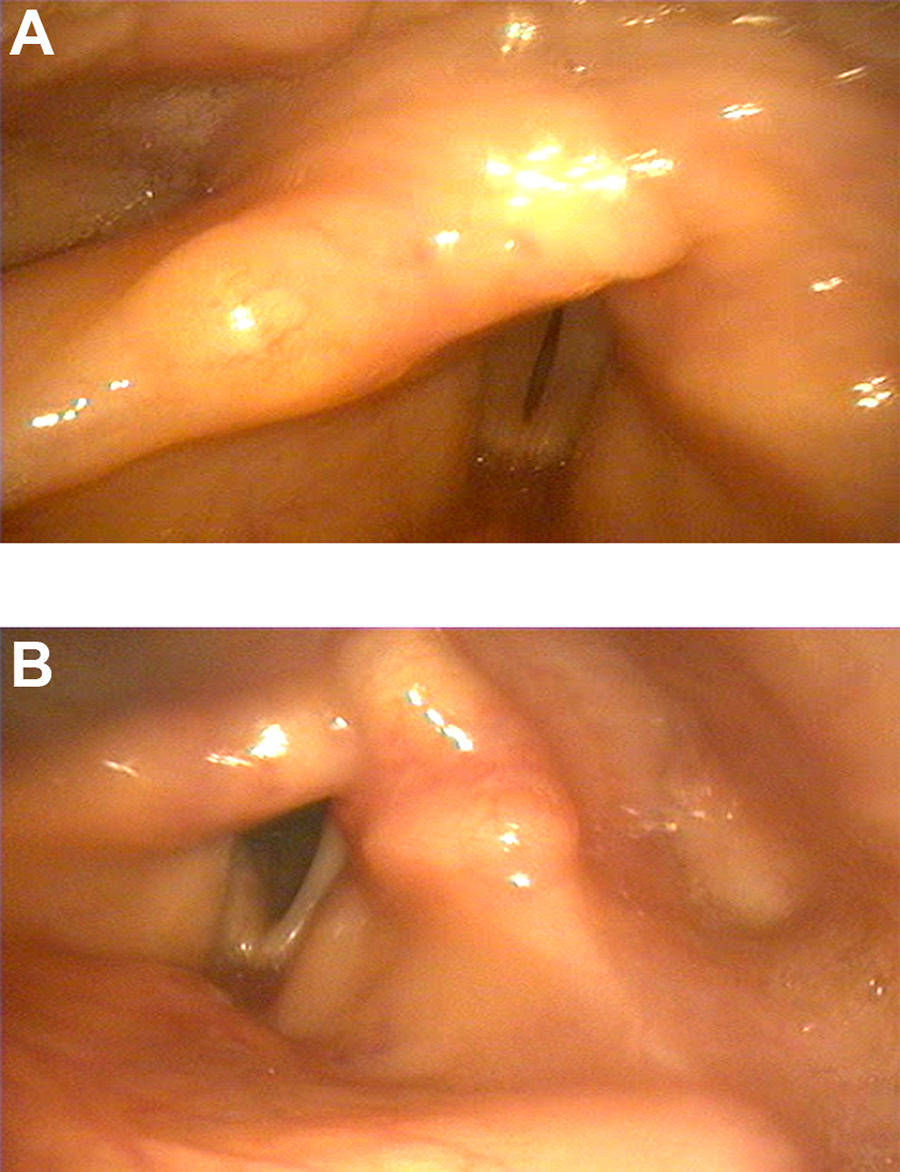
A and B, Laryngeal examination before and after laser arytenoidectomy showing posterior widening of the glottic region.
Surgical Technique
Technique
With the patient fully awake and in the upright sitting position, local nasal anesthesia and decongestion were applied to both nasal cavities by placing 1% lidocaine hydrochloride (HCL) with 1:100 000 epinephrine and 0.1% xylometazoline HCL-soaked sponges. The fiberoptic nasopharyngoscope was then introduced through the left nasal cavity and topical anesthesia to the hypopharynx and larynx was then administered by dripping 2% lidocaine HCL while the patient was asked to phonate (Ref 11001UD1 by Karl Storz). After complete anesthesia to the laryngeal mucosa was ensured, a 0.55-mm thulium laser glass fiber was advanced through the working channel of the fiberoptic nasopharyngoscope until the tip of the fiber was visualized. The laser beam was applied in both contact and noncontact fashion using a pulsed mode, power range 3.5 to 4.5 W, duration 70 to 300 milliseconds, repetition 2 to 4 Hz, and aiming beam 65%. A transverse cordotomy starting at the tip of the vocal process was carried all the way laterally to the thyroid cartilage. Following that, the posterior third of the vocal fold and vocal process of the arytenoid with its overlying mucosa were ablated using the contact and noncontact mode until a posterior chink of 5 to 7 mm was achieved. No complications were encountered during surgery. Following the procedure, patient was instructed to remain nothing per os and resume oral intake only 1 hour after the procedure in order to avoid risk of aspiration.
Discussion
The larynx carries 3 important cross cutting functions, namely breathing, phonation, and swallowing. Injury to the recurrent laryngeal nerve disturbs the intricate interplay between these functions leading to marked disabilities affecting the patient’s quality of life. In cases of bilateral vocal fold paralysis, the surgeon is faced with the challenge to secure the airway and prevent aspiration while marinating an acceptable voice quality. The procedures commonly performed consist primarily of posterior thyro-arytenoidectomy with or without resection of the vocal process. 8 -14 Alternatively, a transverse cordotomy extending to the ventricular fold may be performed. 14 Following numerous reports on external and endoscopic approaches using cold steel instruments. 15,16 Ossoff et al in 1984 described total arytenoidectomy using the carbon dioxide laser. 8,15,16 The surgery which consists of removal of the arytenoid and corniculate cartilages, vocal process, and part of the thyroarytenoid muscle offered several advantages such as superior hemostasis, precision in excision, and minimal morbidity. 8 Few years later, Dennis and Kashima reported laser partial posterior cordotomy, a procedure that leaves a crescent shape defect posteriorly. 9 Crumely in 1993 described the endoscopic medial arytenoidectomy which consisted primarily of medial resection of the body of the arytenoid while preserving both the vocal and muscular processes. 12 The procedure was intended for patients in need for marginal increment in the airway with no jeopardy on phonation. Remacle et al in 1996 reported subtotal arytenoidectomy as a treatment alternative that preserves a posterior shell of the arytenoid. The maintained rigidity of the posterior larynx reduced the risk of aspiration while maintaining a patent airway and good voice quality. 4 Yılmaz et al modified the technique and sutured the posterior mucosal lining in order to avoid leaving any denuded mucosal lining. Anchoring the sutures of the vocal ligament to the posterior glottis help maintained tension within the vocal fold. 17
All the aforementioned procedures are performed in the operating room while the patient is under general anesthesia. This preliminary report of partial arytenoidectomy under local anesthesia concurs the wide emerging frontier of office-based laryngology practice commonly performed for benign and premalignant mucosal lesions. 15 -20 The main advantage of office-based laser arytenoidectomy, similar to other office-based procedures, includes sparing the patient the risk of general anesthesia and the morbidity associated with suspension microlaryngoscopy, namely tongue paresthesia, tooth injury, and inadvertent mucosal injury to the pharyngeal mucosa. From the physician’s perspective, the operating field is in its neutral position and the surgical time is managed more efficiently. The preexisting tracheotomy in the reported patient has no doubt mitigated the risk of potential airway complication and control of hemostasis. Inadvertent aspiration secondary to bleeding could have been easily controlled by inflating the tracheotomy cuff. While this latter is kept inflated, the distal end of the laser glass fiber can be distanced from the bleeding site in order to achieve hemostasis using the defocused mode. In case there is persistent bleeding, the procedure must be aborted and the patient must be transferred to the operating room for better control using suspension microlaryngoscopy under general anesthesia.
Conclusion
Un-sedated office-based laser arytenoidectomy has been successfully performed on a patient with bilateral vocal fold paralysis. It might be considered as a safe alternative to the commonly practiced glottal widening procedures in patients with a preexisting tracheotomy. However, a larger series of cases is needed in order to draw the guideline for proper patient selection, limitations of this technique, and optimal surgical outcome.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.