
Abstract
Purpose:
Upper airway foreign body is one of the most encountered clinical situations in otolaryngology practice. In rare conditions, a living organism may be a foreign body in the upper airway. In this study, we demonstrate 19 patients with leech infestations in nose, nasopharynx, and larynx.
Methods:
This study was enrolled with 19 patients between 2012 and 2016 in a regional state hospital. All of the patients were admitted to clinic with these complaints: epistaxis, hemoptysis, coughing, foreign body sensation, and bloody stool.
Results:
There were 12 male and 7 female patients. The leech was in the nose in 12 patients, in nasopharynx in 6 patients, and in the larynx in only 1 patient. All leeches are removed under local anesthesia (except laryngeal presentation). No bleeding and complication were seen after extraction of leech.
Conclusion:
Leech can be easily diagnosed and managed in the upper aero-digestive tract without any complication and leech-associated disease.
Introduction
A foreign body in the upper airway is a common clinical presentation in otolaryngology practice, with the recognition and removal of a foreign body an important part of daily practice for ear, nose, and throat (ENT) residents and otolaryngologists. 1 The most commonly encountered inanimate foreign bodies include beads, pieces of paper, rubbers, legumes, and small parts of toys. 2 In the pediatric population, an upper airway foreign body may be life threatening if it moves to the trachea or bronchi or obstructs the rima glottis. An unusual foreign body, a living organism like a leech, may sometimes be difficult to diagnose in otolaryngology practice. 3
Among animate foreign bodies, leeches, which are commonly encountered in rural areas, may be found in the upper aero-digestive tract. 4 Leeches are water-living, blood-sucking parasites of various colors and lengths. They may enter the body via oral or nasal routes. Thereafter, they adhere to mucosa and suck blood from their host. The host does not recognize the leech as a foreign body, as the saliva of the host contains anesthetic and anticoagulant agents. 3 As the organism grows in size, it may cause various symptoms, depending on its anatomic location. These symptoms include nosebleeds, hemoptysis, a foreign body sensation, and coughing. 3,5 Herein, we describe 19 patients with leech infestations in the nose, nasopharynx, and larynx.
Patients and Methods
This was a retrospective study of 19 patients who were admitted to a regional state hospital between 2012 and 2016. The ethics committee of Samsun Medicana International Hospital approved this study. All patients’ data were obtained from the hospital’s database.
In terms of clinical features, all the patients had complaints of epistaxis, hemoptysis, a foreign body sensation, and bloody stools. All the patients were from rural areas and had a history of contact with polluted water.
All the patients underwent an ENT examination, including anterior rhinoscopy, which revealed the presence of a leech in all cases. Thus, there was no need for a radiological evaluation. Figures 1 to 4 show the worm-like mobile animate organism in the nose, nasopharynx, and larynx.
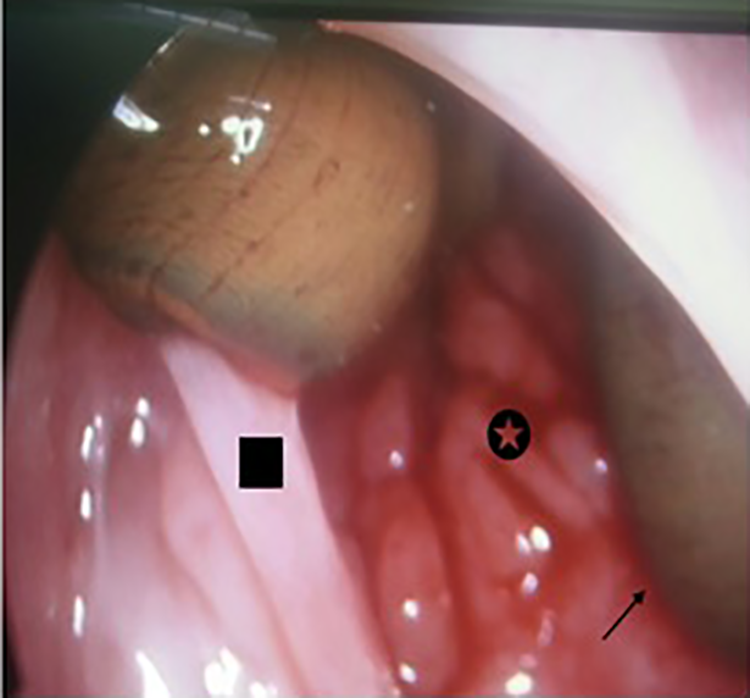
Endoscopic view of a leech in the nasopharynx of a 7-year-old girl. Black arrow: attachment points to the nasopharynx wall. Star: nasopharynx posterior wall. Square: posterior portion of the nasal septum.

An image showing a leech extending from the nasal entrance to the oropharynx.

A leech attached to (what exactly) in the interarytenoid region lying toward the tip of the epiglottis.

Appearance of one of the leeches after removal.
Results
There were 12 male and 7 female patients, with ages ranging from 5 to 60 years. The mean age was 15.7 years. The mean symptom onset time (ie, time of first bleeding) to diagnosis was 3.9 days. In terms of location, the leeches were in the nasal area (n = 12), nasopharynx (n = 6), and larynx (n = 1; Table 1). The laryngeal leech was removed under general anesthesia. In all the other cases, the leeches were removed using a forceps or clamp under local anesthesia with 4% lidocaine spray.
Age, Sex, Symptoms, Localization, and Duration of the Complaints.
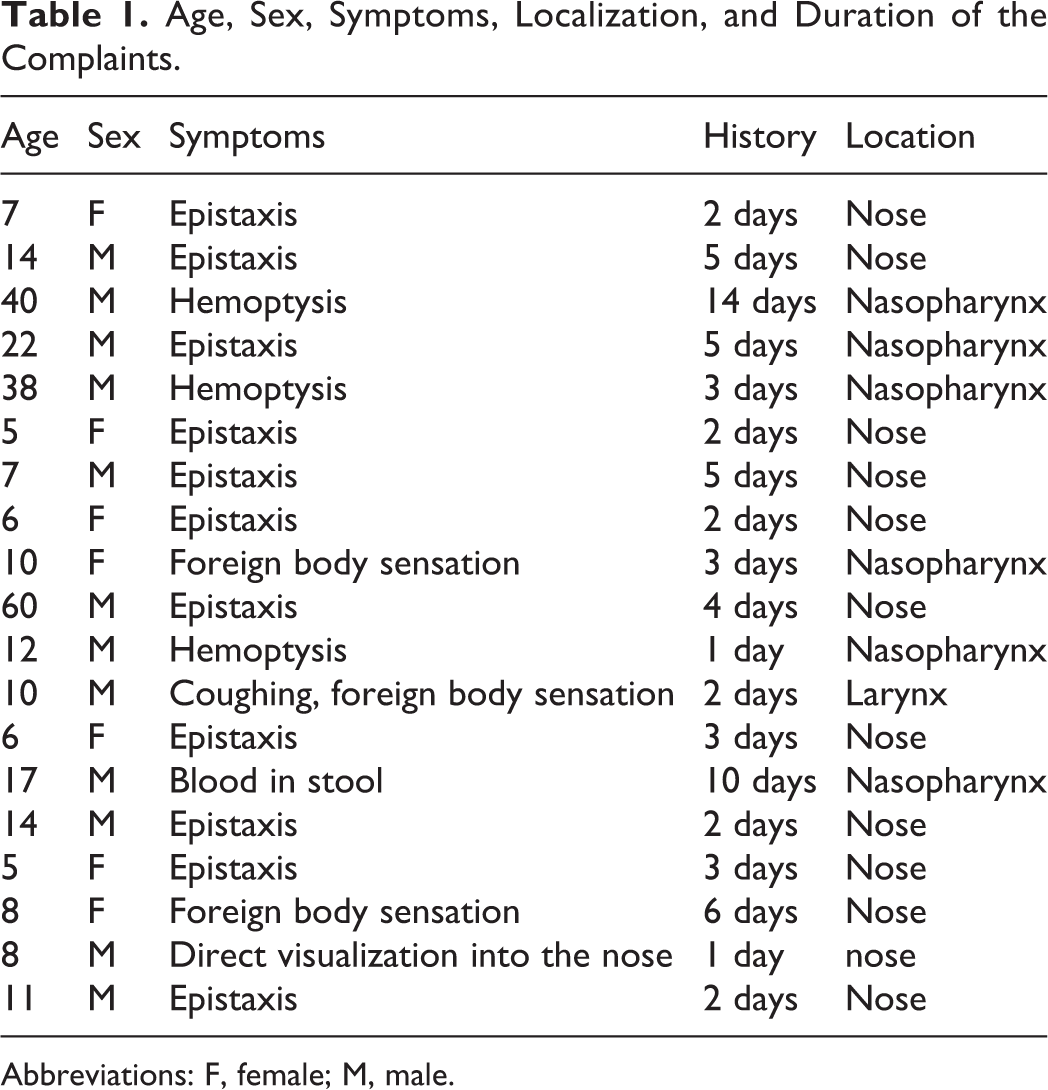
Abbreviations: F, female; M, male.
None of the patients experienced bleeding after extraction of the leeches, and all patient-related complaints improved in a few days. Only 1 patient required an iron supplement due to anemia associated with leech-related bleeding. During the 1-year follow-up period of each case, there were no complications or leech-associated infectious diseases.
Discussion
Among patients who present to otolaryngology clinics and emergency departments with epistaxis or hemoptysis, the cause may be a foreign body in the nose or upper airway. Such foreign bodies are generally seen in the pediatric population but seldom in adults. 1 A living organism is a rare type of foreign body. We described 19 cases of leech infestation and the clinical features.
Leeches that can cause parasitic infestations in humans can be divided into land-based and aquatic-based classes. Land-based leeches have strong jaws and can easily adhere to human skin. In contrast, aquatic-living leeches have weak jaws and require soft tissue to facilitate adherence. After a leech enters the human body, it starts to ingest blood. According to previous research, leeches can ingest blood meals averaging 890% of their weight and ingest about 9 mL of blood within 70.5 minutes. 5,6 A leech bite wound can bleed for several hours. 6 Leeches found in the upper aero-digestive tract are aquatic living organisms and may cause severe anemia as a result of mucous membrane bleeding. 7 Such leeches possess anticoagulant, hirudin, and histamine-like vasodilators, which support bleeding and result in epistasis and haemoptysis. 3,5 Aquatic-living leeches have previously been found in conjunctiva as well as in the vulva, vagina, urethra, esophagus, and trachea. 5,8,9 When located in the nasopharynx, a leech may resemble a neoplasm.
Leech infestations can cause severe anemia, which may require a transfusion. None of the patients in the present study required a transfusion. Cundall et al described 3 cases of severe anemia due to leech infestation, with death due to blood loss in 1 case. 7 Public awareness of leech infestation in endemic areas means that people present to the hospital shortly after symptoms occur. Early presentation can prevent fatal conditions. Recurrent epistaxis, living in an endemic area, or vising endemic areas and contact with polluted water can provide clues for the clinician that a foreign body may be a leech.
There are some case reports and case series in the literature of upper aero-digestive tract infestations, in which various methods were used for leech removal. Chen et al used a forceps to extract a leech in a number of cases and electric shock in 1 case. 5 Other researchers reported the use of hypertonic saline irrigation for leech extraction.
According to local knowledge in southeast part of Turkey, when a leech is squeezed for approximately 5 to 20 seconds at the midpoint of its body, it will spontaneously release its mouthparts from the mucosa to which it is attached. In the present cases, H. K. removed the leeches using this method. In the cases where the leech was in the nasal passage, a nasal polyp forceps was inserted into the nasal passage, and the leech was grasped at the midpoint of its body. As soon as it detached itself from the mucosa to which it was adhered, it was removed through the nasal passage. In the nasopharyngeal infestations, the lower part of the organism’s body extended into the oropharynx. Thus, in an oral cavity examination, it was easily visualized behind the soft palate and lateral to the tonsils. In these clinical presentations, the tongue was depressed using a tongue depressor. The organism was then held using a straight hemostatic clamp and removed via the oral route. This method is simple and easily applicable in the office setting, although the otolaryngologist must take extreme care not to drop the organism in the larynx. No complications were encountered in the present cases.
In conclusion, the present article describes our clinical experience of foreign body leech infestations and provides information on leech removal methods that may be of use to otolaryngologists, emergency department specialist, and ENT residents. Experienced otolaryngologists can easily diagnose a leech infestation in endemic areas and remove the leech from the upper aero-digestive tract. Living in rural areas where leeches are endemic and swimming in or drinking polluted water may provide clues for clinicians. Pressing the organism at the midpoint of its body for 5 to 20 seconds using a forceps will cause the organism to detach from the mucosa and aid extraction.
Footnotes
Author’s Note
This study was presented as oral presentation at International Hippocrates Congress on Medical And Health Sciences on March 1, 2019 to March 3, 2019, Ankara/Turkey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.