
Abstract
Carotid artery pseudoaneurysm is a rare but serious complication of a retropharyngeal abscess in children. We report the first case of treating an unruptured mycotic pseudoaneurysm of the extracranial internal carotid artery (ICA) in a pediatric patient with vascular plugs. A 3-year-old patient presented with airway compromise and signs of neck sepsis. Successful embolization of the pseudoaneurysm was achieved with 2 Amplatzer vascular plugs to close the front and back door. The patient did not have any neurological deficit. Repeat imaging with ultrasound and computed tomography confirmed no recurrence of the pseudoaneurysm.
A 3-year-old boy presented with airway compromise and signs of neck sepsis to a district general hospital and was transferred to our institution’s pediatric intensive care unit for further management. Ultrasound and contrast-enhanced computed tomography (CT) imaging (see Figure 1) revealed a retropharyngeal abscess, complicated by an adjacent large left-sided cervical internal carotid artery (ICA) pseudoaneurysm 4 cm in diameter. The pertinent clinical issue was managing the child’s airway; however, the pediatric anesthetists were concerned about the risk of the pseudoaneurysm rupturing during intubation, as it could be visualized as a pulsatile mass on direct inspection of the pharynx using a laryngoscope. However, given the child’s increasing anxiety and respiratory distress, the multidisciplinary team decided to proceed with intubation, which was successfully carried out by a senior pediatric anesthetist. The child had also been started on intravenous antibiotics.
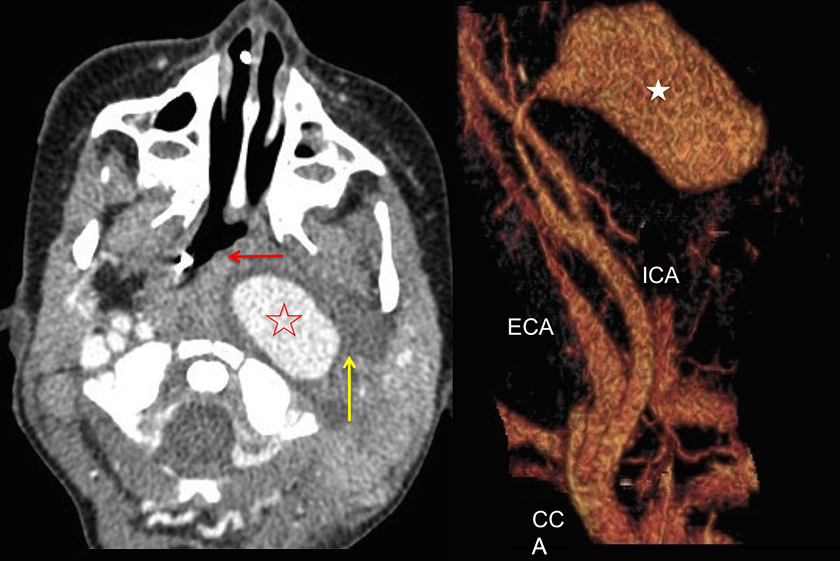
Axial contrast enhanced CT angiogram showing left ICA pseudoaneurysm (open star) causing mass effect and pharyngeal/tracheal compression (red arrow). Low attenuation fluid around the pseudoaneurysm in keeping with retropharyngeal abscess (yellow arrow). Reconstructed CT imaging (with bone removed) shows 3D image of the left internal carotid pseudoaneurysm (star) prior to intervention, which measured 4 cm in maximum length. CT indicates computed tomography; ICA, internal carotid artery; 3D, 3-dimensional.
Carotid angiography was undertaken, confirming massive cervical pseudoaneurysm and spontaneous intracranial cross flow. Due to the size of the aneurysm and concern for risk of rupture and neurological symptoms, the multidisciplinary team elected for immediate intervention. Successful embolization of the left ICA pseudoaneurysm was achieved with a 5-mm and an 8-mm Amplatzer plug (backdoor and frontdoor embolization, respectively), without any complications (see Figures 2 and 3). Both vascular plugs were deployed from the ipsilateral ICA as the ICA pseudoaneurysm was crossed with a microcatheter easily. Perfusion to both cerebral hemispheres was maintained via the right ICA and left vertebral respectively which was checked pre-embolization. The patient was extubated after several days and discharged 2 weeks later following treatment with antibiotics and without any neurological deficit. Repeat imaging with ultrasound and CT confirmed no recurrence of the pseudoaneurysm.
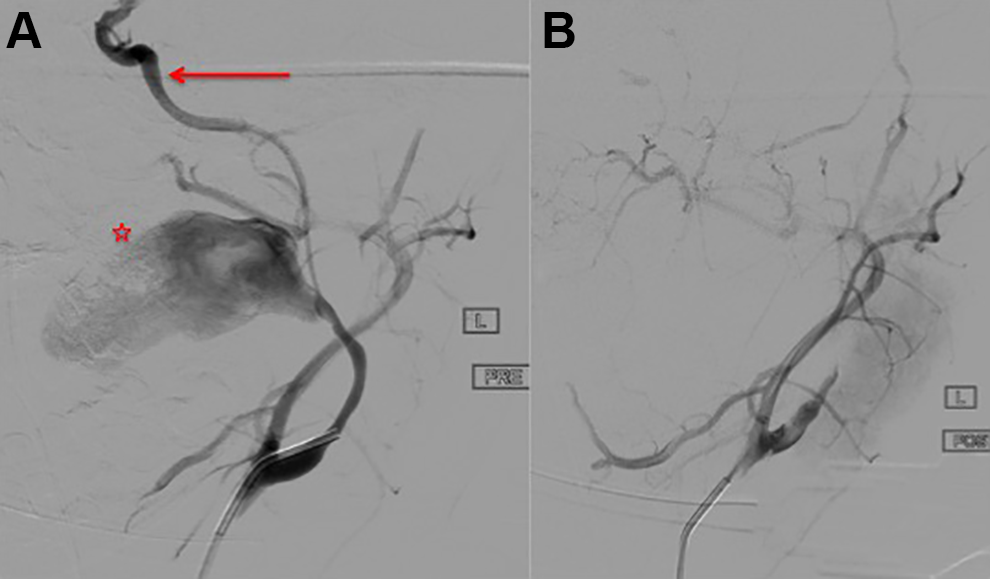
A, Digital subtraction angiogram (DSA) of left common carotid artery (CCA) in a left anterior oblique view revealed a patent left external carotid artery (ECA) filling the petrous left ICA via collateral flow. A small caliber ICA was patent distal to the pseudoaneurysm (star), becoming more normal caliber in the cavernous portion (arrow). B, The distal left ICA was embolized with a 5-mm Amplatzer 4 plug and the proximal with a 8-mm Amplatzer 4 plug resulting in successful occlusion of the left ICA. DSA confirmed no flow into the pseudoaneurysm. ICA indicates internal carotid artery.

Nonsubtracted image showing position of the 2 Amplatzer vascular plugs within the ICA. ICA indicates internal carotid artery.
Extracranial carotid artery aneurysms and pseudoaneurysms are rare, accounting for less than 1% of all arterial aneurysms. 1 The etiology is diverse and includes atherosclerosis, infection, connective tissue disorders, and trauma. 2 Although mycotic pseudoaneurysms in the context of neck sepsis are rare in the age of antibiotics, they remain a possible serious complication. Most present as a pulsatile mass but they can cause cranial nerve compression or stroke from emboli. 3 Although traditionally these were treated with open surgery first-line, endovascular intervention has increasingly been shown to be safe and effective with cohort studies and systematic reviews published in the literature. 4
A variety of surgical and endovascular options have been utilized in the treatment of carotid artery aneurysms including use of stent grafts with or without additional coiling of the aneurysm or pseudoaneurysm, which is the most published technique in the literature for treating aneurysms of the carotid arteries. However, endovascular stenting is also associated with potential complications, including early thrombosis and late stent stenosis, with quoted restenosis rates of 6% particularly if the stent is located at a kink or bend in the carotid artery. 4 Surgical management of extracranial carotid artery aneurysms carries a 7.7% risk of perioperative stroke, which can be fatal. 5
From the literature search, this is the only case of endovascular treatment of an extracranial ICA pseudoaneurysm with vascular plugs.
Endovascular options considered were either stent graft placement or embolization. Stent grafting was thought to be associated with significant risk of rupture during device insertion due to the tortuous nature of the left ICA anatomy. For backdoor and frontdoor embolization, vascular plugs were felt to provide a more accurate placement over a very short segment of the ICA when compared to coils, while keeping implanted devices away from the area of active infection of any device used. Given the retropharyngeal abscess surrounded the ICA, there was additional concern for a stent graft to become infected.
Mycotic pseudoaneurysms of the extracranial ICA are rare in the pediatric population, with limited evidence base behind treatment strategies however can result in potentially devastating and should be promptly diagnosed and treated to prevent rupture or stroke. Endovascular options can be safe and effective in treating such lesions with appropriate treatment planning. Case series and innovative techniques used to treat ICA pseudoaneurysms should be published to expand the evidence base to aid in future treatment planning.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.