
Abstract

A 58-year-old woman was admitted to our department with hoarseness for 1 month. Physical examination revealed a cervical mass at the right supraclavicular area with right vocal cord palsy. Computed tomography revealed a 4.2-cm heterogeneously enhancing mass that extended from the right lower lobe of the thyroid gland to the right supraclavicular fossa, which encircled the right innominate artery (Figure 1). Ultrasonography-guided fine needle aspiration cytoloty (FNAC) of the ill-defined hypoechoic mass at the inferior thyroid lobe was interpreted as papillary thyroid carcinoma with a poorly differentiated feature. Positron emission tomography revealed neoplastic activity in the right lower lobe of the thyroid gland, right cervical lymph nodes, and the varied-sized metastatic nodules in both lungs. Thus, the patient was diagnosed initially with papillary thyroid carcinoma of stage cT4bN1bM1.
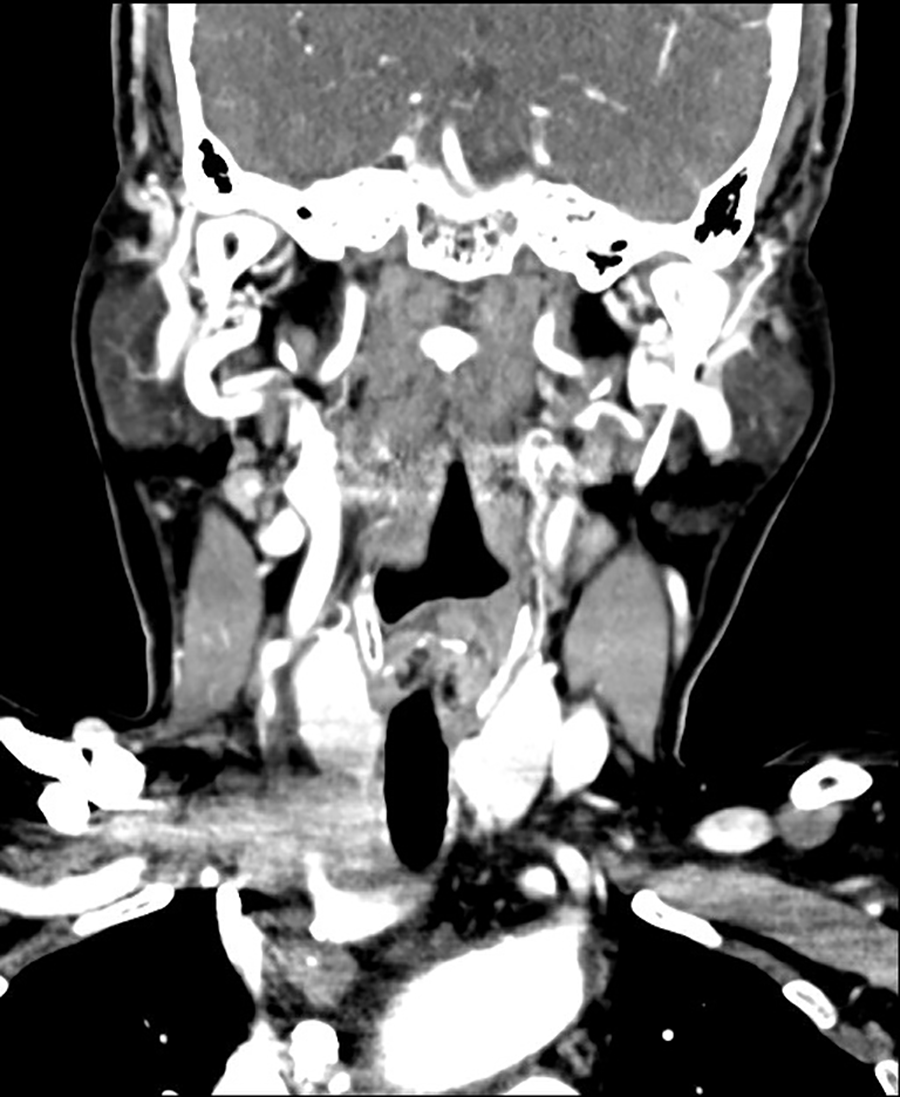
Enhanced computed tomography (CT) showing the 4.2-cm heterogeneously enhancing mass without calcification, which encircled the right innominate artery.
Operation was performed with therapeutic intent for postoperative radioiodine therapy. Intraoperative examination demonstrated invasion of the right recurrent laryngeal nerve, right vagus nerve, right internal jugular vein, and right innominate artery (Figure 2A). But the tumor had not infiltrated the adjacent trachea. Multiple metastatic nodes were found in the central and right lateral neck compartments. Total thyroidectomy and right selective neck dissection (II-VI) were performed. The right recurrent laryngeal nerve, vagus nerve, and innominate artery were killed. The artery was reconstructed by the cardiothoracic surgeon using a synthetic Y-graft between the right common carotid artery and the aorta, and between the right subclavian artery and the aorta (Figure 2B).
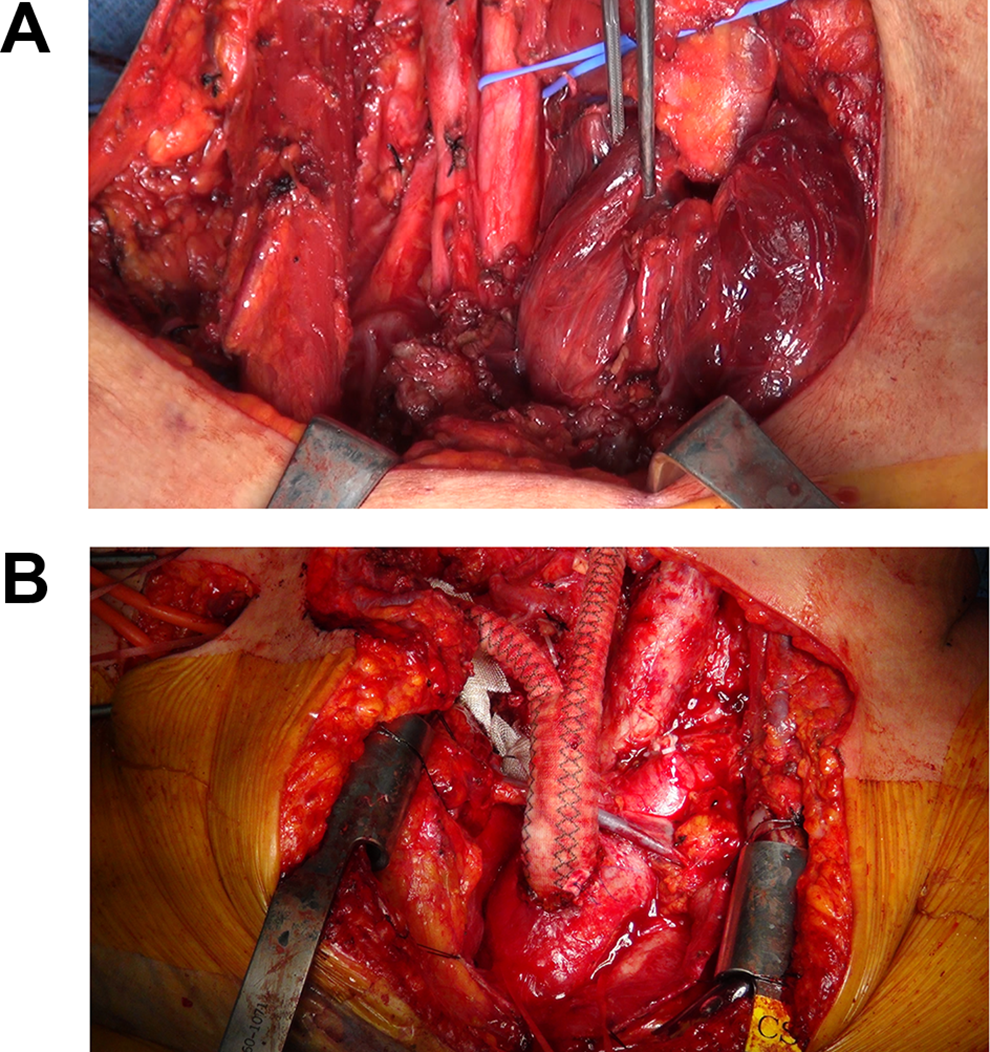
The tumor from the lower lobe of the right thyroid infiltrated the innominate artery, vagus nerve, and internal jugular vein. The tumor was removed with the innominate artery, and the artery was reconstructed with a Y-graft.
On microscopic examination, the tumor showed an expansive growth in the thyroid gland without capsular structures, extending into the surrounding soft tissue. Lower power view showed lobulated epithelial cell nests separated by desmoplastic fibrous stroma. This architecture is similar to that in thymic neoplasm. The tumor cells had squamoid or syncytial features with eosinophilic cytoplasm. The mitotic figures were 1 per 10 high power fields. The tumor islands were infiltrated by moderate lymphocytes and plasma cells. Immunohistochemistry revealed positive staining for CD5 and negative staining for thyroid nuclear factor 1. Based on all of these results, the final histopathological report confirmed the presence of a thyroid carcinoma showing thymus-like differentiation (CASTLE). So postoperative chemotherapy was performed after radical operation and she is alive with disease at 4-years follow-up with persisting right vocal cord palsy.
Thyroid CASTLE is a rare tumor of the thyroid gland, with a prevalence rate of approximately 0.08% to 0.15% among malignant thyroid neoplasms. 1 Preoperative diagnosis of thyroid CASTLE is difficult because its clinical manifestations are commonly observed in other aggressive and advanced thyroid carcinomas in the following aspects: hard mass with poor mobility and invasion to adjacent organs. 2,3 Furthermore, images of thyroid CASTLE are not specific and the diagnostic value of FNAC is limited. 4 But, it has typical morphological characteristics in hematoxylin and eosin staining of specimens. And similar to thymic carcinoma, thyroid CASTLE is strongly positive for CD5. Differences between FNAC findings and those of typical carcinoma could be indicative of thyroid CASTLE, as in our patient case.
Generally, CASTLE is a slowly progressing tumor with a low potential for malignancy and indolent biological behavior, for which treatment with external irradiation after surgery can be expected to be efficacious. 3,5 And it often invades adjacent soft tissues or organs and sometimes, the tumor extensively invades the surrounding organs, including the larynx, trachea, esophagus, or major vessels. But, curative surgery with radical resection of tumor can achieve favorable outcomes. 2,3,6 Therefore, complete resection of the tumor including infiltrated organs is imperative not only for reducing local recurrence rates and improving survival rate but also for accurate diagnosis. In our case, it is clear that total thyroidectomy and neck dissection with resection of innominate artery were essential to achieve good prognosis.
In case of distant metastasis, no standard treatment policy has been established yet. 3,6 But, chemotherapy is commonly used in patients with unresectable and/or metastatic CASTLE. Because the tumor cells in CASTLE originate from ectopic thymic tissue, many doctors attempted novel regimens for thymic malignancy. 7 -12 And the results were various, from no response to complete remission. Like those doctors, we adopted cisplatin and 5-fluorouracil and the result was good until 16 months after operation.
This is the first case report about aggressive CASTLE with innominate artery invasion and lung metastasis. Despite the more common indolent feature of disease, this case indicates that thyroid CASTLE may exhibit an aggressive phenotype. Thus, suspecting CASTLE based on atypical cytological features and imaging findings is highly important for early diagnosis and suitable treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.