
Abstract
The aim of this study was to assess whether the chronic preoperative administration of intranasal corticosteroids (INCs) in chronic rhinosinusitis with/without nasal polyposis (CRSwNP/CRSsNP, respectively) could significantly influence bleeding during functional endoscopic sinus surgery (FESS). We prospectively enrolled 109 patients (56 CRSwNP and 53 CRSsNP) candidate for FESS who underwent clinical evaluation and anamnestic data collection. They were allocated to 2 groups depending on whether or not they were chronic INC users, as declared at their first medical evaluation: chronic “INC users” represented the treated group, while “INC nonusers” formed the control group. Lund-Mackay and American Society of Anesthesiology (ASA) scores, blood loss expressed both in milliliters and using the Boezaart scale, operation time in minutes, pre- and postoperative 22-item Sino Nasal Outcome Scores (SNOT-22) were collected. Each sample underwent histopathological evaluation. The results showed that anamnestic information, Lund-Mackay, and SNOT-22 scores were similar between the 2 groups (P > .05). The average blood loss expressed in milliliters and operative time were slightly, but not significantly, higher in the INC user group, while the Boezaart scores proved significantly higher in the INC users (P = .038). No differences emerged between CRSwNP and CRSsNP within each group in terms of bleeding. The pathologist described common features in the majority (78%) of INC group samples: ectatic venules embedded in a fibrous stroma and hypertrophy of the arterial muscular layer. In our experience, despite the presence of NP, chronic preoperative administration of INCs was associated with increased intraoperative bleeding according the Boezaart scale although objective recordings of blood loss were not statistically different between the INC users and nonusers.
Keywords
Introduction
Chronic rhinosinusitis (CRS) is a heterogeneous disease classified into 2 main phenotypes based on the presence or absence of nasal polyposis (chronic rhinosinusitis with nasal polyposis [CRSwNP] and chronic rhinosinusitis without nasal polyposis [CRSsNP], respectively). Medical therapy represents the first stage of treatment and consists mainly of antibiotics, nasal irrigations, and corticosteroids. 1,2 In the case of medical therapy failure, surgery should be considered and a functional endoscopic sinus surgery (FESS) represents the gold standard treatment. 3 A clean surgical field is one of the most important factors affecting the surgical outcome. In fact, excessive bleeding can impair the endoscopic view during surgery, thereby increasing the incidence of skull base or orbital injuries. 4,5 Sinus surgeons usually use several techniques to lower/decrease bleeding and improve visibility during FESS, but the ideal technique is yet to be standardized. Although topical intranasal corticosteroids (INCs) are strongly recommended for the symptoms of CRS, 6 the role of INCs is not clear in the preoperative setting, once the decision has been made for FESS. 7 During our multiyear experience, the surgeon retrospectively investigated patients without risk factors who presented excessive bleeding during FESS and noted that the only common factor among them was the chronic preoperative use of INCs. To assess this relationship, we conducted a preliminary internal evaluation, in which we retrospectively collected anamnestic data about the preoperative administration of steroids and intraoperative bleeding scored according Boezaart scale in a cohort of patients treated with FESS for CRSwNP and CRSsNP. The Boezaart score is an ordinal scale routinely used by the surgeon to grade intraoperative blood loss based on the need for suctioning. We investigated the hemodynamic parameters noted during surgery in each patient form: baseline systolic, diastolic, mean arterial pressures, heart rate, and the depth of anesthesia using the E-entropy device. The partial results showed that when topical steroids were chronically administered preoperatively, the surgeon noted abnormal venous bleeding during surgery, despite the controlled hypotension induced by total intravenous infusion of propofol and remifentanil; by contrast, bleeding was less when no preoperative use of INCs was recorded. This retrospective observation (unpublished data), pointed to a need to better assess the preoperative use of topical steroids in relation to blood loss during FESS. We therefore conducted this prospective study with the primary aim of assessing whether the chronic administration of INCs could significantly influence bleeding during FESS; the secondary aim was to compare the histopathological features of the nasal mucosa in INC users and INC nonusers.
Patients and Methods
This prospective observational cohort study analyzed cases of CRS with or without NP refractory to medical therapy. Patient candidates for FESS were recruited from the Ear, Nose and Throat Department of Cattinara Hospital in Trieste, Italy. The study protocol was approved by the Ethics Committee on Clinical Investigation (232/2016). The study ran from April 2016 through April 2017. Patients were informed about the purpose of the study and gave their written consent. A single experienced surgeon carried out all the procedures.
Patient Selection
The study included 109 patients with a diagnosis of CRS: 56 patients had a diagnosis of CRSwNP (41 male, 15 female; mean age, 52 [14] years) and 53 patients CRSsNP (33 male, 20 female; mean age, 42 [14] years). Table 1 summarizes the study inclusion and exclusion criteria.
Inclusion and Exclusion Criteria.
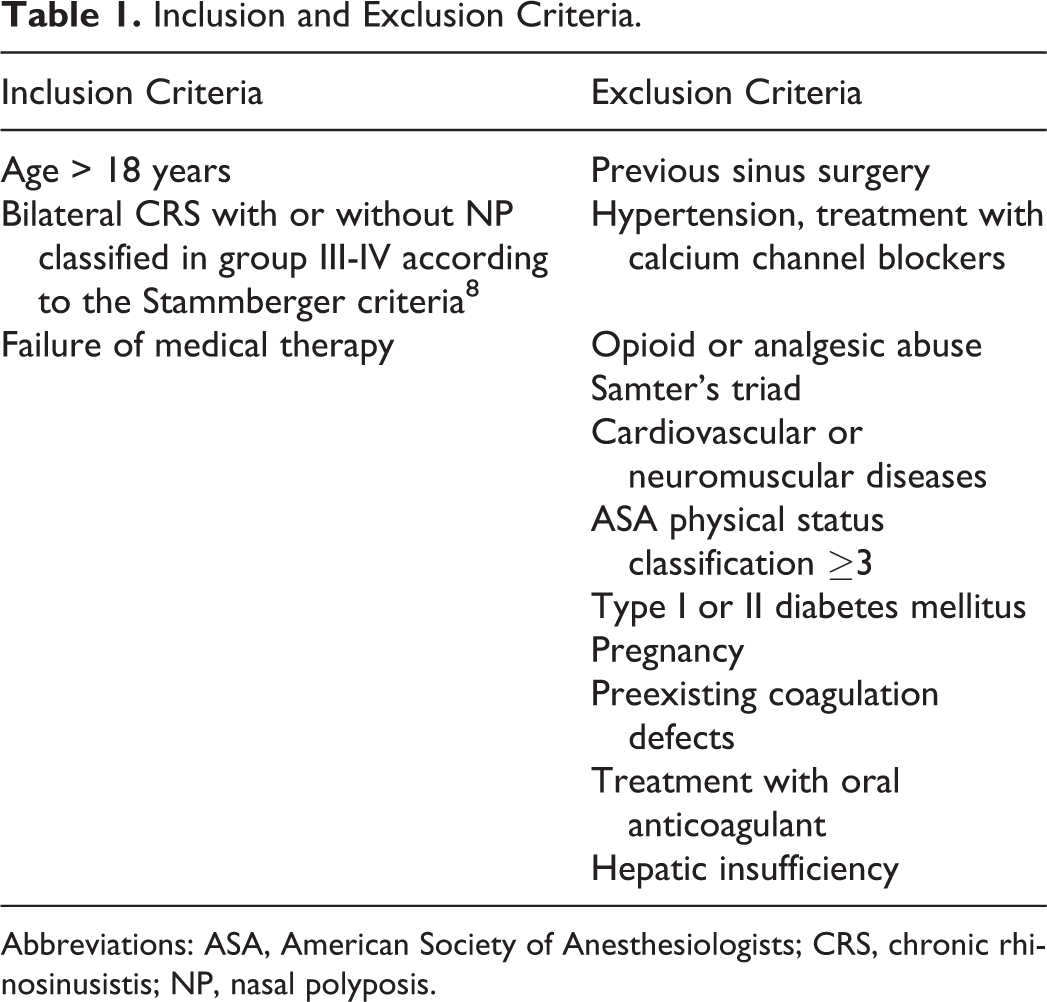
Abbreviations: ASA, American Society of Anesthesiologists; CRS, chronic rhinosinusistis; NP, nasal polyposis.
The diagnosis is mainly based on the criteria described by European Position Paper on Rhinosinusitis and Nasal Polyps 2012. 9 Patients who fulfilled the inclusion criteria underwent clinical evaluation and anamnestic data collection; particularly, the general condition of the patient was staged based on the American Society of Anesthesiology (ASA) scale.
A complete endoscopic evaluation of the upper aerodigestive tract was performed in all patients. To avoid selection bias, among CRSwNP we included groups II, III, and IV according to the Stammberger criteria. 10 A computed tomography (CT) scan of the sinuses was systematically performed before surgery. The extent of the sinus opacities was staged according to the Lund-Mackay scale. 11
Finally, a subjective assessment of symptoms at baseline was obtained using a validated questionnaire, namely, the 22-item Sino Nasal Outcome Score (SNOT-22). 12
Patients were allocated to 2 groups depending on whether or not they made chronic INC use, based on the patient’s declaration at the first medical evaluation: the chronic “INC users” were assigned to treated group, while the “INC nonusers” were enrolled as a control group. The treatment was considered chronic when the patient administered at least 1 puff once a day for at least 3 months. To ensure uniformity within the treated group, we enrolled only patients who were using second-generation INCs (eg, ciclesonide, fluticasone furoate, fluticasone propionate, mometasone furoate, betamethasone sodium phosphate). Once allocated to the groups, both patients and controls were asked to not change their INC status by stopping or beginning INC use after enrollment, so as to avoid methodological bias.
The surgeon was unaware of the participants’ allocation. Blinding of the personnel performing endoscopic sinus surgery was implemented by identifying a member of the research team (G.S.) as blinding authority. Specifically, he systematically provided the surgical team with a hard copy of the patients’ medical history intentionally concealing all the information concerning INCs.
Anesthesia and Surgical Technique
The anesthetic procedure was standardized, and baseline heart rate and systolic, diastolic, and mean arterial pressures were recorded. Induction was performed with an intravenous target control infusion of propofol and remifentanil using an Orchestra infusion workstation (Fresenius Kabi AG, Bad Homburg, Germany). Systolic, diastolic, and mean arterial pressures were monitored during surgery. If hypertension or tachycardia occurred, the infusions of remifentanil or urapidil were adjusted to stabilize the parameters.
The surgical procedure was standardized as follows: topical decongestion of the nasal mucosa with 0.25% phenylephrine HCL and then injection of 1:100.000 lidocaine–epinephrine solution in the middle turbinate and inferior wall of the ethmoidal bulla.
13
The extension of surgery was based on the CT scan findings. We decided to exclude cases in which septoplasty was performed, because this procedure could increase both the blood loss and the time of surgery.
14
–16
Finally, each nasal fossa was packed with Merocel (Medtronic Xomed Inc, Jacksonville, Florida). The operation time (in minutes) was routinely noted in the operating room form, and intraoperative blood loss was assessed by both objective and subjective measures: Objective of blood loss: The amount of blood in the suction collection system at the end of the surgical procedure, expressed in milliliters. Bleeding in the surgical field: The surgeon routinely uses the scale described by Boezaart et al.
17
to assess the grade of intraoperative blood loss in relation to the need for suctioning; at the end of surgery, the surgeon reported the average score in the operating room form, summarized as follows: 0 = no bleeding; 1 = slight bleeding with no suction of blood; 2 = slight bleeding and occasional suction; 3 = slight bleeding and frequent suctions, the surgical field is threatened; 4 = moderate bleeding that threatens the surgical field despite frequent suctions; 5 = severe bleeding with constant suctioning, surgical field severely threatened. Conventionally, a patient is considered as a “bleeder” when the score is equal to or greater than 3.
13,17
To compare the histological features of the 2 groups, the biopsy of the mucosa was kept separated from the polyps and fixed in formaldehyde for histological and immunohistochemical analysis (CD31 and CD34). To ensure a blind examination, a single pathologist blinded to the experimental setup analyzed all the samples.
Postoperative Management and Follow-Up
After surgery, we prescribed antibiotic therapy until removal of the nasal packing (4 days) and nasal irrigations with isotonic saline 3 to 4 times daily for 3 weeks starting 1 day after nasal packing removal.
Routinely, the clinical postoperative follow-up was performed at 4 weeks. At least 6 months after surgery, we recalled each patient and administered the SNOT-22 questionnaire to collect the postoperative scores.
Statistical Analysis
Data analysis was conducted at the Treviso Regional Hospital—Center for Head and Neck Cancer (University of Padua, Italy).
This study considers patients with and without polyps together in the initial evaluation of the considered parameters. However, subgroup analyses explore potential differences between them.
Statistical analysis was performed using dedicated software (Statistical Package for Social Sciences v.15, SPSS Inc, Chicago, Illinois). The normal distribution of scalar data was evaluated with a Kolmogorov-Smirnov test and the homogeneity of variances with a Levene test and Q-Q normality plots. Because of this analysis, nonparametric tests were chosen. Differences in relation to the Lund-Mackay, ASA and Boezaart scores were evaluated between the 2 groups with a Mann-Whitney U test. Age, operation time, and blood loss (in mL) were compared by means of an independent Student t test. The significance level was set at P < .05.
Results
We excluded 12 patients who dropped out of the study because they did not return as requested after 6 months to fill out the questionnaires. Thus, the sample included 97 patients (51 CRSwNP and 46 CRSsNP), 41 of chronic INC users (treated group) and 56 INC nonusers (control group). Anamnestic information was found to be homogeneously distributed between the groups (P = .13). The mean Lund-MacKay scores in the 2 groups were similar (P = .30). There were no differences in baseline SNOT-22 score between groups (P = .25; see Table 2). No major complications occurred during the surgery, and controlled hypotension was efficiently achieved with the adopted anesthetic protocol without any additional drug administration. Although the average blood loss expressed in milliliters was slightly different in the 2 groups, the result was not statistically significant (P = .07). By contrast, the Boezaart scores were significantly lower in the control group than in the INC group (P = .038). Subgroup analyses explored distinctions between CRSwNP and CRSsNP within each group, and no differences were found in terms of Boezaart scores. A slightly longer operative time was recorded in the INC group in comparison to the average duration of surgery observed in the control group, but the difference was not statistically significant (P = .09).
Results.
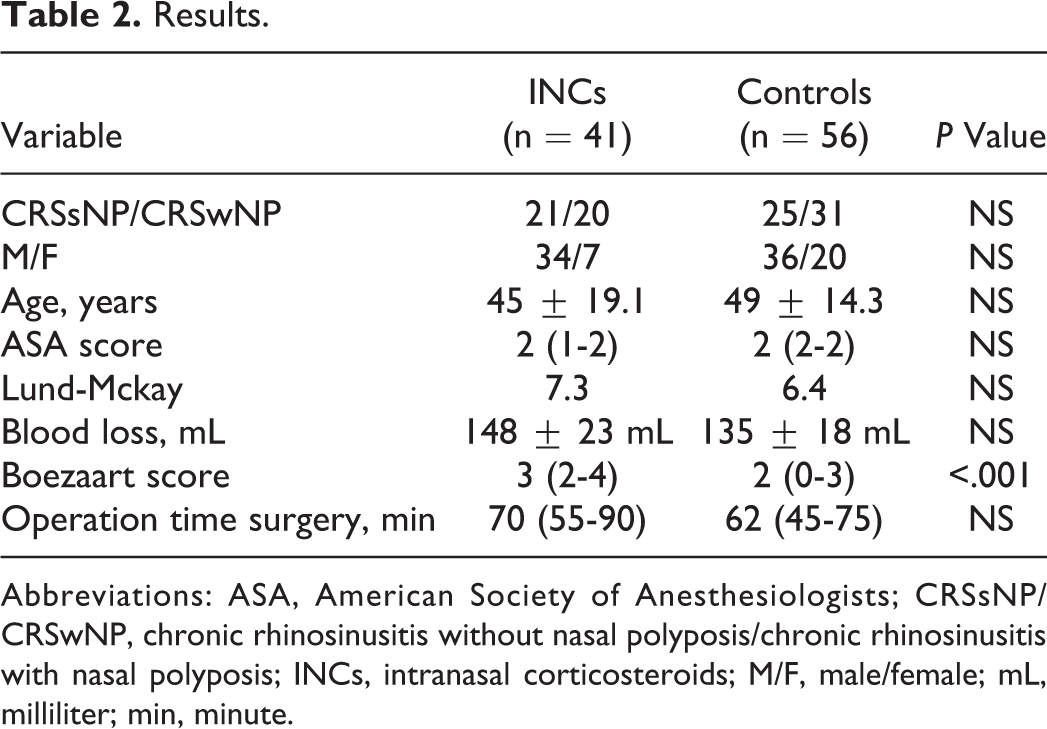
Abbreviations: ASA, American Society of Anesthesiologists; CRSsNP/CRSwNP, chronic rhinosinusitis without nasal polyposis/chronic rhinosinusitis with nasal polyposis; INCs, intranasal corticosteroids; M/F, male/female; mL, milliliter; min, minute.
The pathologist found common histopathological features among the samples of patients treated with steroids in 32 (78%) of 41 cases. The venules were dilated and ectatic, immersed in a fibrous stroma that enclosed thin arteries; moreover, and the muscular layer appeared hypertrophic causing partial occlusion of the arterial lumen. The INC user samples also presented a slightly higher incidence of eosinophils, but the difference was not statistically significant (Figure 1A and B). Conversely, the control group samples exhibited a normal capillary bed interspersed in minor salivary glands, with no muscular arteries or ectatic venules (Figure 1C).
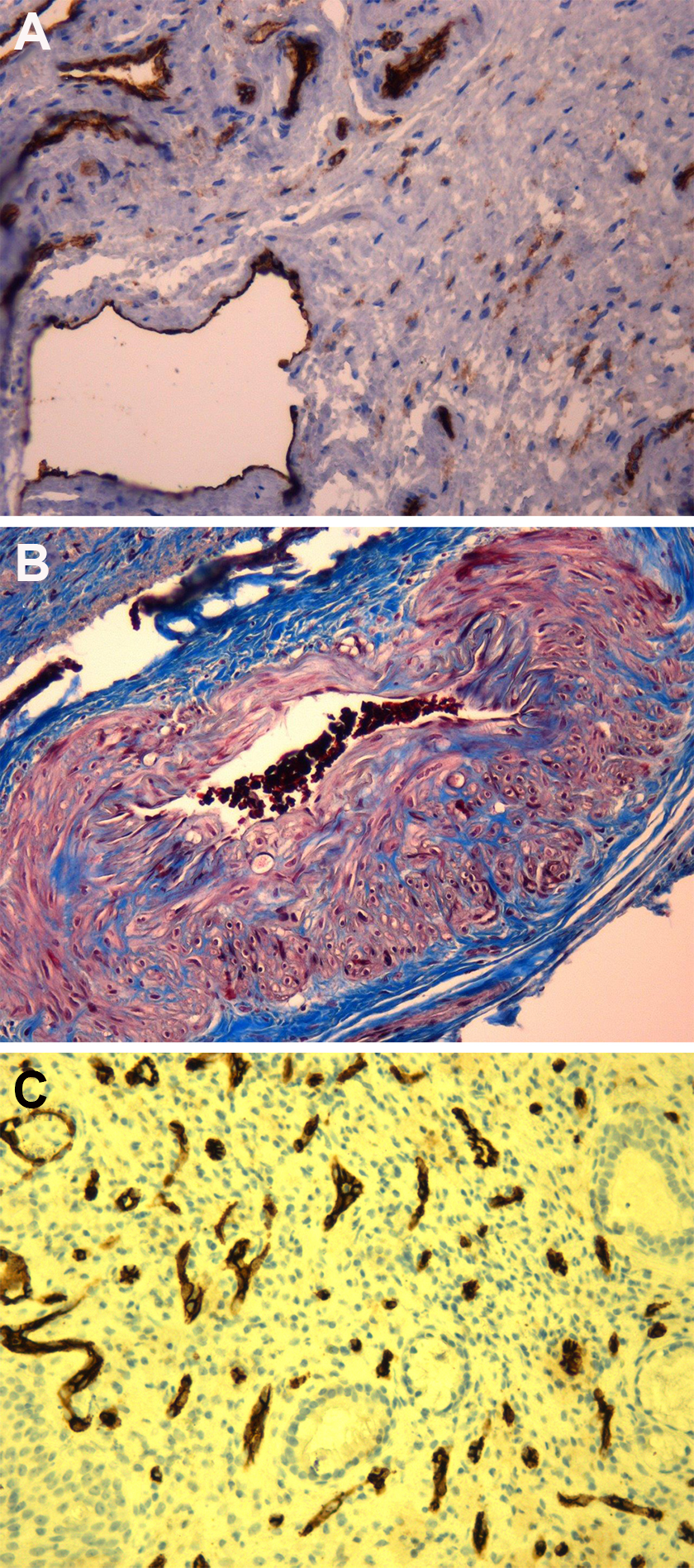
Representative specimens of each subgroup highlighting different vascular patterns. A, Intranasal corticosteroid (INC) group: 20× CD31-stained specimen. B, INC group: 40× Azan-Mallory-stained section. C, Control subgroup: 20× CD34-stained specimen.
With regard to the SNOT-22 questionnaire, neither the pre- nor postoperative scores showed a statistically significant difference between the 2 groups (P = .09 and P = .25, respectively).
Discussion
In the present study, there was no statistically significant difference between INC users and nonusers in terms of age, anamnestic characteristics, and pre- and postoperative symptoms scored with SNOT-22, meaning that symptoms at baseline were similar and FESS improved the condition of both groups, despite the preoperative therapy administered. The average Lund-Mackay scores were also similar between the 2 groups so that, differently from Mortuaire et al, 18 the bleeding grade could not be predicted by the radiological score in the present study. Although the difference between the 2 groups in terms of intraoperative bleeding expressed in milliliters was not statistically significant, the results showed that patients who chronically made use of INCs presented significantly higher Boezaart scores during surgery in comparison with patients who did not.
This inconsistency between objective and subjective measurements could be explained by the fact that the amount of blood loss during FESS is in any case small, so the surgeon can detect even a slight increase in bleeding in such a restricted surgical view.
Moreover, no differences in terms of Boezaart score were found between CRSwNP and CRSsNP in each group, meaning that this parameter was not influenced by the presence of NP. As reported in a recent meta-analysis, 19 in this study, controlled hypotension was efficiently achieved using total intravenous anesthesia without any additional drug administration during FESS. 13 The time of surgery was slightly (but not significantly) longer in the INC group, since intraoperative bleeding may interfere with the surgical procedure. This result could be explained by the more frequent suctioning required by the greater venous bleeding threatening the surgical view although not enough to significantly increase surgical time. It should also be underlined that in some “bleeder” cases, the excessive bleeding compromised the surgical view, and the surgeon had to suspend the FESS to repeat the topical decongestion and wait until a better surgical view had been restored, whereas in 3 cases the surgeon had to stop the procedure, thus shortening the duration of surgery and invalidating our estimates of average duration.
Although it has been demonstrated that steroids delivered topically have beneficial effects in patients with CRS due to their potent anti-inflammatory properties, the treatment response in studies is very heterogeneous. 20 Steroids are used preoperatively by many surgeons and can relieve symptoms. A Cochrane systematic review by Chong et al. 8 assessing the effects of INCs when compared to no treatment or placebo in CRS found that most of the evidence is of low quality. Symptoms that seem to be improved are nasal blockage, rhinorrhoea, and disease severity; only the risk of nosebleeds is increased with high-quality evidence, but this evaluation included all levels of disease severity, and the risk of local irritation was not clearly investigated.
A Cochrane meta-analysis demonstrated significant benefit especially in postoperative patients. 21 In preoperative patients, oral steroids have been shown to reduce blood loss intraoperatively, but little has been published on topical steroids. 7,22 Specifically, the one study published 5 did not distinguish between endotypes (wNP and sNP) of CRS, and the authors recommended additional clinical trials to confirm their results with regard to standardized indications for corticosteroid administration.
We agree that surgery is reserved for symptomatic cases that do not benefit from medical treatment; this is often the case of NP because polyps obstruct the normal flow of the INCs through the nasal fossa, making the drugs less effective. 23 Moreover, the effect of steroids is mediated by the activation of specific receptors, α and β isoforms, which have different functions: the first binds to steroids leading the anti-inflammatory effect, while the second interferes with the α receptors. 24 In patients with CRSwNP, the expression of β- and α-receptors is increased and downregulated, respectively, supporting the theory of a secondary resistance to steroid therapy for this disease. 25,26 This may account for the unbalanced results between the benefit and the lack of benefit of INCs in CRSwNP.
Moreover, epistaxis is another common adverse effect of INC use, with a reported incidence between 17% and 23%. 27 It is reasonable to suppose that increased bleeding during surgery and increased risk of epistaxis have in common the same mechanism of development. In fact, in our clinical records, INC users presented higher bleeding scores, despite the presence of NP.
Figure 2 shows intraoperative endoscopic views before the surgical procedure in different INC users, in comparison to endoscopic views from a control (Figures 3). The superficial vascular reticulum is quite evident, and it covers the septal mucosa, the middle turbinate, and the middle meatus.
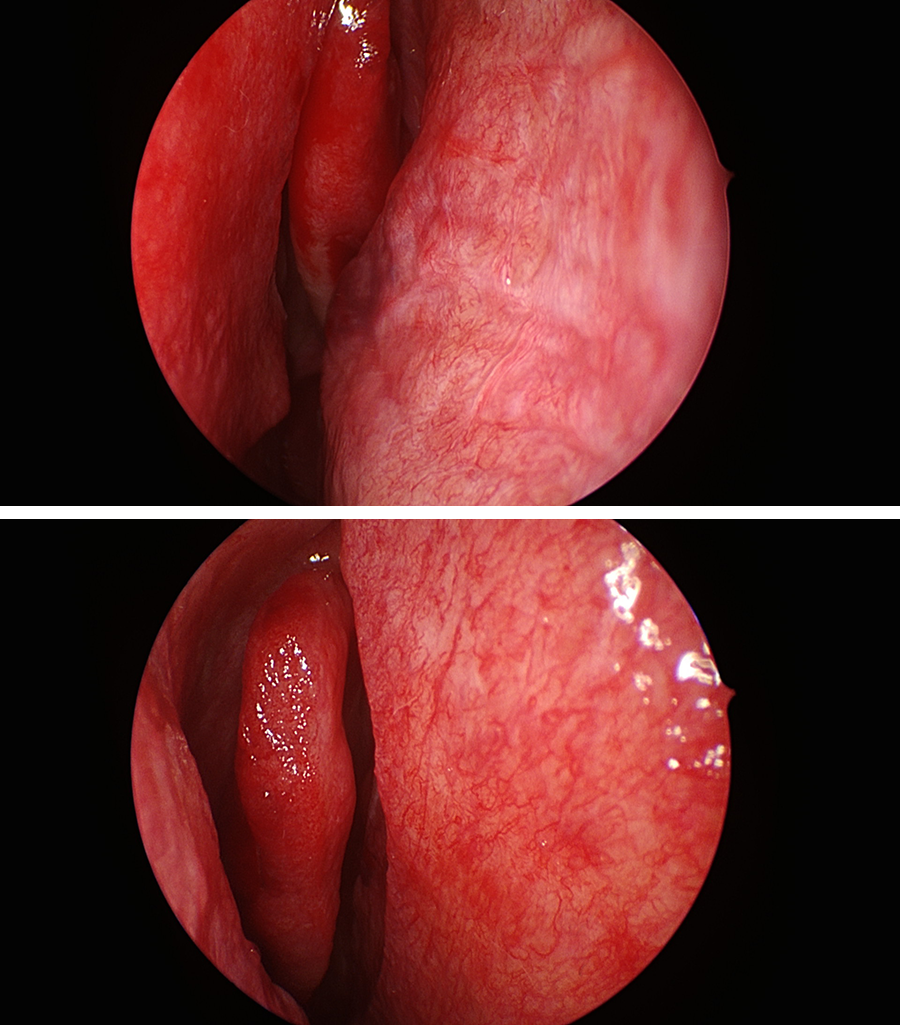
Intraoperative view of the nasal septum mucosa and middle turbinate before surgery; representative patients belonging to treated group.
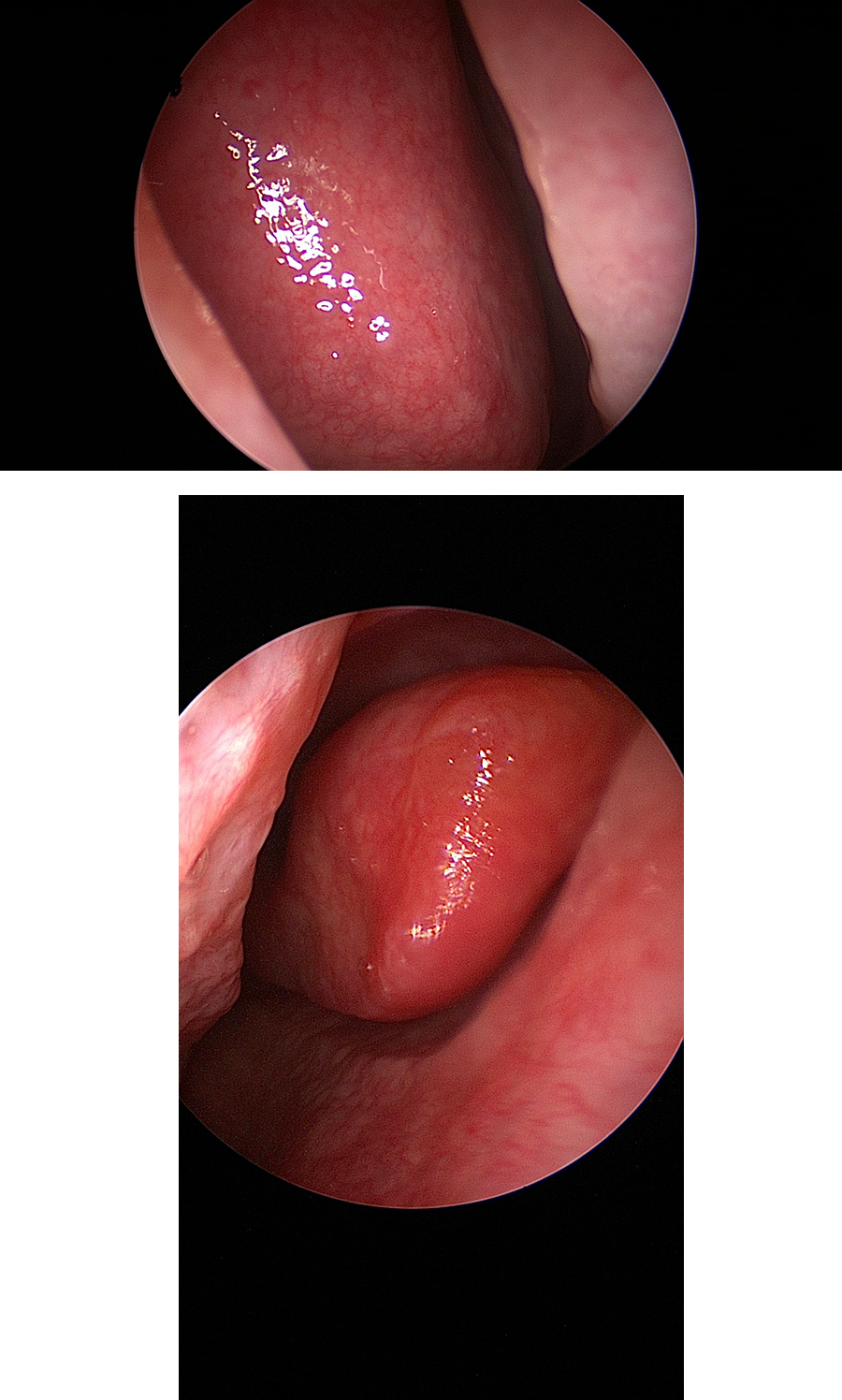
Intraoperative view of the nasal septum mucosa and middle meatus before surgery; representative patient belonging to control group.
The histopathological findings of the present study observed in patients who had taken steroids (Figure 1A and B) may be due to the INC administration, and this could justify the increased bleeding recorded during surgery. This speculation is further supported by the fact that in these patients the intraoperative bleeding seemed mostly venous, in agreement with the ectasia of the venous vessels clearly observed in the histologic specimens. A review of histological assessments of nasal mucosa after intranasal steroids reported that there was no evidence for mucosal atrophy, while increased glandular hyperplasia and squamous metaplasia may represent a reversal of the remodeling, rather than atrophy, of the nasal airway. 28,29
Steroids act through multiple molecular pathways and mechanisms that make a consensus difficult. Research on the action of different steroids in the field of rhinology may lead to a systematic use focused on more specific pre- or postoperative indications.
The strengths of this study are the prospective design, the use of standardized outcome measures (CT score, SNOT-22, and Boezaart score), and the blinded nature. Conversely, the main limitations are that the groups were self-selected, and the study was conducted in a single institution.
In our experience, the chronic preoperative administration of INCs was associated with increased intraoperative subjective bleeding according the Boezaart scale although objective recordings of blood loss were not statistically different between INC users and nonusers.
Footnotes
Acknowledgments
The authors thank Itala Mary Ann Brancaleone, MA, RSA Dip TEFLA, teacher of Medical English at the University of Trieste, for her support in editing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.