
Abstract

A 50-year-old woman presented with progressive dysphagia for 6 months. She also reported fatigue and dyspnea on exertion. Physical examination was notable for pallor conjunctiva, angular cheilosis, and atrophic glossitis. Esophagography demonstrated a plate-like filling defect at the anterior wall of the cervical esophagus without circumferential involvement of the lumen (Figure 1). Upper panendoscopy disclosed a cervical esophageal web (18 cm level from central incisors) without obstruction (Figure 2). Laboratory studies showed marked anemia with hemoglobin level of 5.3 g/dL, mean corpuscular volume of 60.2 fL, serum iron of 10 µg/dL, total iron binding capacity of 290 µg/dL, and serum ferritin of 3.22 ng/mL. The diagnosis of Plummer-Vinson syndrome (PVS) was established. Symptoms of the patient gradually resolved after treated with oral iron replacement for 3 months. Annual upper panendoscopy was suggested due to the significant association of PVS with upper gastrointestinal carcinomas. 1 Anemia and dysphagia could be effectively treated with iron supplementation alone; however, repeated endoscopic bougies, pneumatic balloons, or even surgery may be needed in some recalcitrant cases. 2,3

Lateral view of the barium esophagram demonstrating a thin membrane arising from the anterior wall of the cervical esophagus causing mild obstruction and mild proximal dilatation (arrow).
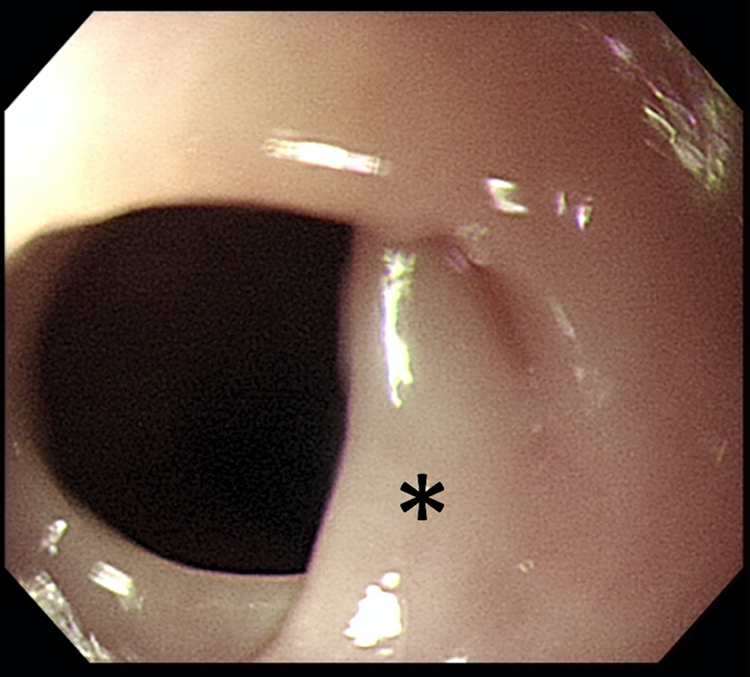
A cervical esophageal web is noted at 18 cm level from central incisors without obvious obstruction (asterisk).
Footnotes
Authors’ Note
The Plummer-Vinson syndrome, also called the Paterson-Brown-Kelly syndrome, consists of a triad of dysphagia, iron deficiency anemia, and esophageal webs.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.