
Abstract
The laryngopharyngeal reconstruction in patients with pyriform sinus carcinoma continues to be a challenge for surgeons. In this article, we describe our experience with laryngopharyngeal reconstruction in patients with pyriform sinus carcinoma using the modified infrahyoid myocutaneous flap (IHMCF). The modified incision design for the modified IHMCF and clinical outcomes are also detailed here. Between January 2012 and February 2018, 10 patients with hypopharyngeal squamous cell carcinoma who underwent laryngopharyngeal reconstruction using the modified IHMCF after hemicricolaryngopharyngectomy were included in this study. The drainage vessels of the modified IHMCF, oncological outcomes, and functional reservation of the larynx were recorded. All of the flaps survived well. No flap necrosis or other major complications occurred during follow-up. None of the patients remained on nasogastric feeding for more than 4 weeks postoperatively. The follow-up period ranged from 12 to 73 months (mean, 36 months). In our series, 6 patients were successfully decannulated and 5 had received radiation therapy. We roughly assessed the speech and swallowing functions, and the outcomes seemed acceptable in all of the patients after surgery. Laryngoscopic examination showed that the modified IHMCF survived well and the new glottis provided excellent function and good ventilation results. In our experience, the modified IHMCF is a safe and viable procedure that can serve as a valid alternative to free flaps and the pectoralis major myocutaneous flap to reconstruct laryngopharyngeal defects.
Keywords
Introduction
Squamous cell carcinoma (SCC) of the hypopharynx represents an aggressive cancer with a dismal prognosis due to the late presentation of symptoms and consequently, the treatment remains challenging to the otolaryngologist. The distribution of hypopharyngeal cancer within these subsites is as follows: pyriform sinus: 64.5%; hypopharynx not otherwise specified: 18.0%; posterior hypopharyngeal wall: 7.2%; and aryepiglottic fold: 5.2%. 1 Patients with advanced cancer of the hypopharynx may be managed with surgical resection and reconstruction, followed by postoperative (chemo)radiation, induction chemotherapy, or concurrent systemic therapy/radiation therapy. 2,3
Currently, many different surgical modalities for reconstruction after surgery to remove head and neck cancer are commonly used. Accepted reconstructive concepts include free flaps, pedicled flaps, and jejunum flap. 4 Despite the evolution of microvascular free flaps with the advancement of microsurgical techniques, pedicled flaps are widely used to reconstruct defects after head and neck surgery due to their ease of harvesting, viability of the pedicle, and extensive experience of the surgeons using them.
Wang et al first reported infrahyoid myocutaneous flaps (IHMCFs) for head and neck reconstructions in 1986, and IHMCFs were proven to be a good choice in certain cases. 5 The IHMCF is a pedicled myocutaneous flap fed by the superior thyroid artery and its branch. It has 2 drainage systems: the skin paddle that is drained by the superficial venous system and infrahyoid muscles that are drained by the superior thyroid vein; the ramus communicans is situated between the 2 drainage systems. 6 In the microvascular free flap era, the often overlooked infrahyoid flap still represents a reliable, quick, and easy reconstructive procedure. 7 In this article, we reported our experience of using the modified IHMCF for laryngopharyngeal reconstruction in selected patients undergoing hemicricolaryngopharyngectomy. We analyzed the restoration outcomes of swallowing, respiration, and voice, in addition to operative morbidity and oncological results.
Patients and Methods
From January 2012 to February 2018 (73 months), the medical records of 10 patients with pyriform sinus SCC who underwent hemicricolaryngopharyngectomy and reconstruction of mucosal defects with modified IHMCFs were retrospectively reviewed. All of the patients were males, and their mean age was 60 years (range, 43-72 years; median, 62 years). All of the patients had a pathological diagnosis of SCC and none had received preoperative radiotherapy or prior cervical surgical procedures.
The criteria for selecting our patients were as follows: extension into the entire unilateral pyriform sinus, invasion of the ipsilateral hemilarynx (which may result in one immovable vocal cord) and, according to the physical findings and imaging studies, swelling of the cervical lymph nodes presenting as a mobile, soft texture with smooth borders and a size less than 2 cm in the greatest dimension. Cases with tumors vertically crossing the postcricoid region, interarytenoid area, or epiglottis were excluded from the study, as were those with tumors extending to the posterior pharyngeal wall, thyroid cartilage, or deep extrinsic muscle of the tongue. Patients who required radical neck dissection or sacrifice of the internal jugular vein were considered unsuitable for IHMCF reconstruction. Disease was staged according to the 7th edition of the TNM staging system, established in 2010 by the American Joint Committee on Cancer. 8 Eight patients were classified as T3 and 2 as T4. The lymph nodes were classified as N0 in 3 patients and N1 in 7 patients. Clinical data for these patients are summarized in Table 1. All of the patients had undergone a single, modified intraoperative IHMCF for defect reconstruction. All of the flaps were unilateral, and the sides were determined by the primary tumor; therefore, the cervical incision for neck dissection and skin paddle were outlined on the same side of the neck.
Demographic Characteristics of the Patients (All Male) Who Underwent IHMCF Reconstruction.
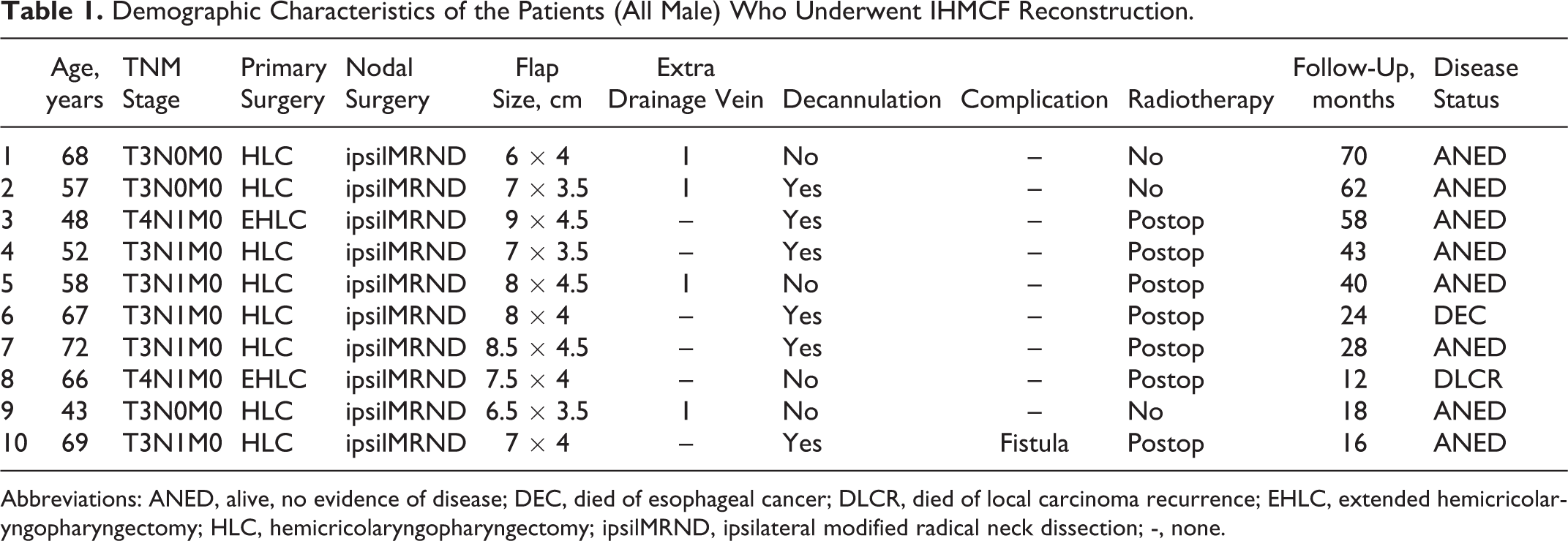
Abbreviations: ANED, alive, no evidence of disease; DEC, died of esophageal cancer; DLCR, died of local carcinoma recurrence; EHLC, extended hemicricolaryngopharyngectomy; HLC, hemicricolaryngopharyngectomy; ipsilMRND, ipsilateral modified radical neck dissection; -, none.
We had created a 3-dimensional reconstruction of the laryngopharyngeal defect by using of our own designed IHMCF, and it can reduce postoperative aspiration by rebuilding a new pyriform sinus, but no one had published this modified design. The modified IHMCF was divided into A, B, and C areas, which were reconstructed according to defects of the laryngotracheal cavity, aryepiglottic fold, and pyriform sinus and lateral pharyngeal wall, respectively. Using C area of the flap can help rebuild a new pyriform sinus, and the laryngopharyngeal defect was a 3-dimensional reconstructed structure with a modified IHMCF (Figure 1). The medial border of the flap lies at the midline, the superior border is 2 cm above the hyoid bone, and the inferior border is at the suprasternal notch; the lateral border is 3.5 to 4.5 cm from the midline. The skin paddle must be tailored to, and included in, the incision for neck dissection. First, the skin and platysma at the lateral and extensile superior border of the modified incision were incised, followed by the fascia along the anterior edge of the sternocleidomastoid muscle. Next, the superior belly of the omohyoid muscle was separated from the inferior segment and elevated toward the lateral border of the skin paddle. Modified radical neck dissection was performed in the usual fashion, with careful dissection of the pedicle and preservation of venous drainage from the flap, and the arterial and venous pedicle of the flap was skeletonized (Figure 2). The space between the enlarged lymph nodes and internal jugular vein can be clearly seen; if any signs that the nodes involved the internal jugular vein were found, the flap would be abandoned (Figure 3). Second, a medial and inferior border incision was made. The sternohyoid and sternothyroid muscles were then transected distally at the suprasternal notch. The motor innervations of the infrahyoid muscles were resected in our cases, provided by the ansa cervicalis, because denervation atrophy of the underlying musculature will increase the flap’s pliability and plasticity. 9 The skin paddle was sutured to the subjacent muscles, and the flap was then raised over the proper capsule of the thyroid gland. When the fine dissection reached the upper pole of the thyroid gland, the distal end of the superior thyroid vessels that entered the gland and cricothyroid artery were individually separated, ligated, cut, and kept with the flap. Thereafter, the sternothyroid and thyrohyoid muscles were released from the thyroid cartilage and then the sternohyoid and omohyoid muscles were excised from the hyoid bone. Finally, the flap was simply attached by the vascular pedicle, due to easy transfer for laryngopharyngeal defects (Figure 4).
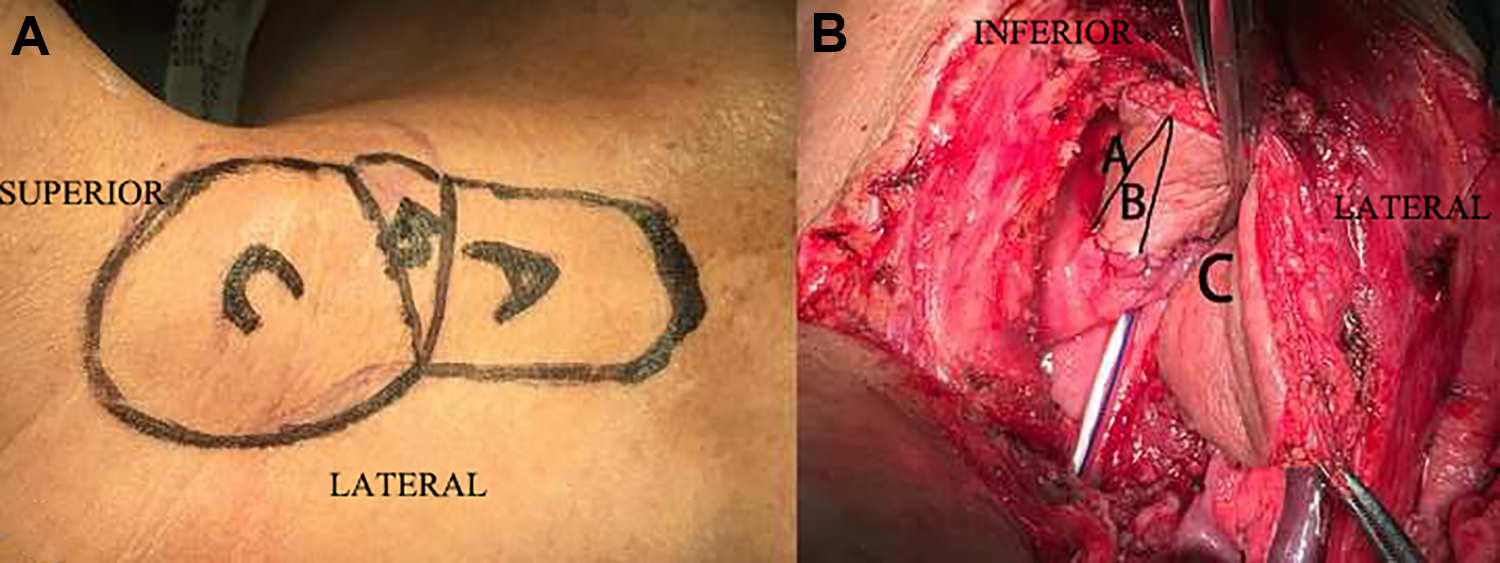
A, Preoperative photo of modified incision divided into A, B, C area. (B) Reconstructive details: area A reconstructed defects of the laryngotracheal cavity, area B was folded to straddle the aryepiglottic fold and part of the postcricoid region, and area C reconstructed defects of the pyriform sinus and lateral pharyngeal wall.
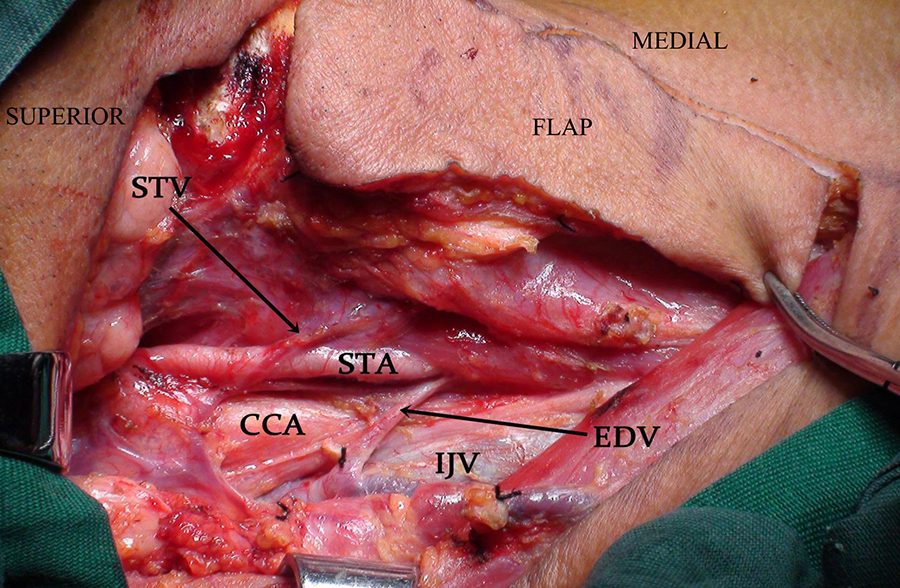
The venous draining of the flap was carefully preserved after left modified radical neck dissection as the photograph showing: STV: superior thyroid vein; EDV: extra drainage vein; IJV: internal jugular vein; STA: superior thyroid artery; CCA: common carotid artery.
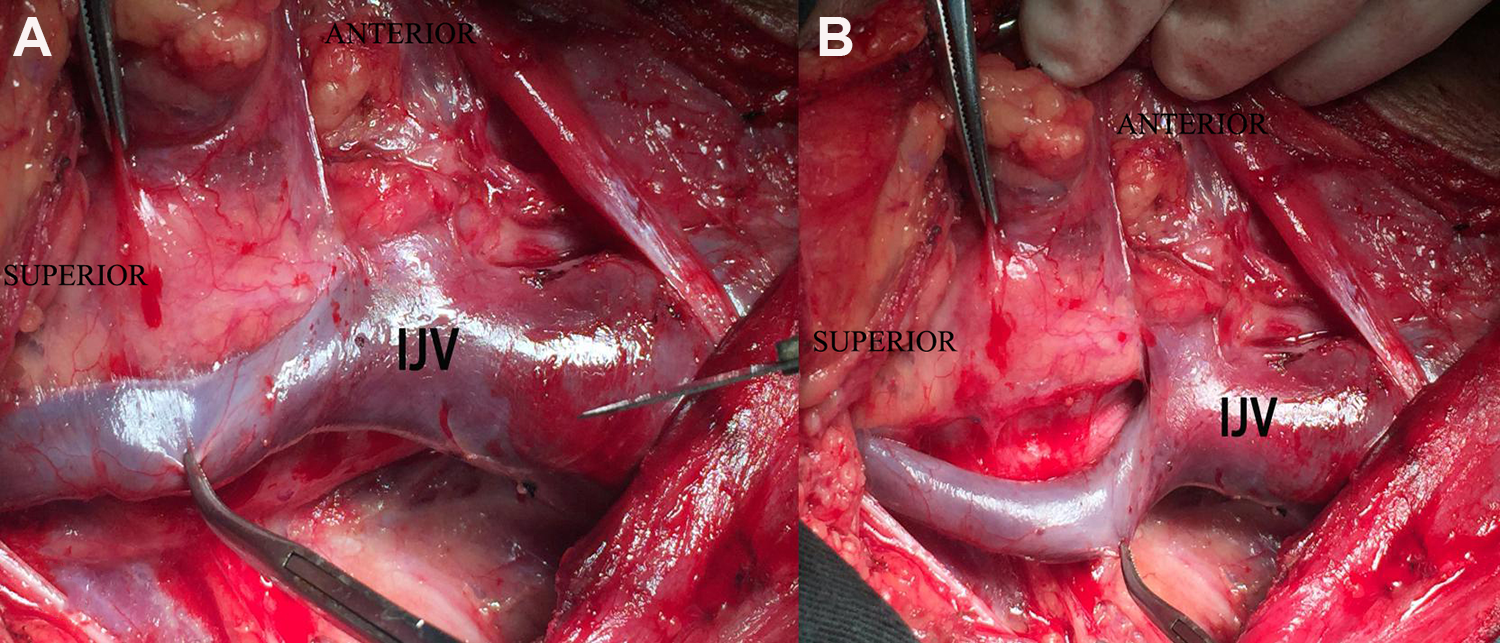
Intraoperative details. A, The internal jugular vein (IJV) had been dissected carefully. B, No signs of IJV had been invaded.
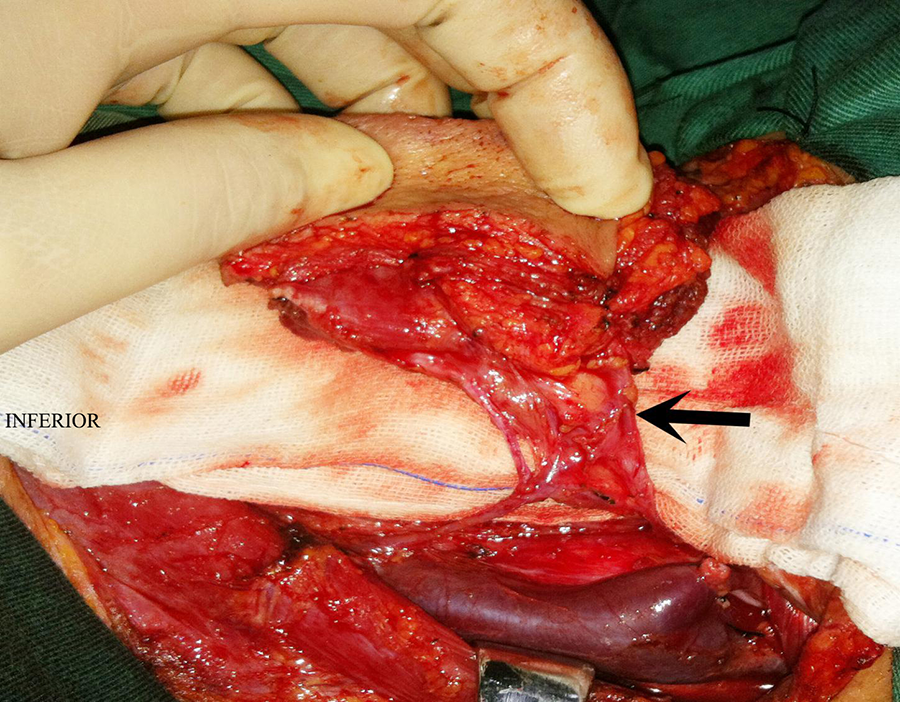
Intraoperative view of the arterial and venous pedicle (arrow) and then transferred to laryngopharyngeal defect for reconstruction.
After implementing tracheotomy, the vertical hemicricolaryngopharyngectomy procedure, in accordance with Krespi and Sisson, 10 was performed on our selected patients who had pyriform sinus carcinomas. In 8 patients, tumor excision of the hemi-laryngopharynx, half of the hyoid bone, the thyroid cartilage and cricoid ring, the epiglottis, the pyriform sinus apex, and the partial thyroid gland nearby the cricothyroid articulation was performed. In 2 patients, tumor resection involved extended resection of the tongue base. All the patients had made intraoperative frozen excision margins, and 3 patients had positive incisal margins in the lateral pharyngeal wall or base of the tongue, then the positive tumor excision margins were incised again until a free margin away from the tumor was secured. Clear excision margin was ensured by using intraoperative frozen section. Then, the laryngopharyngeal defect was reconstructed with a modified IHMCF.
With respect to the clinical data, we roughly assessed the status of the flap, postoperative complications, oral feeding, tracheotomy tube ablation, and speech. Oral intake was started about 2 weeks after surgery, and the nasal feeding tube was removed when the patient could swallow liquids without aspiration. The reconstructed laryngopharynx was anatomically evaluated by laryngoscope, and the tracheotomy tube was considered to be removed when no new glottic stricture was seen on laryngoscopic examination.
In our study, 7 patients received postoperative radiotherapy, and the radiotherapy dose was determined on an individual basis (range, 5500-6500 cGy).
Results
Between January 2012 and February 2018, 132 patients with hypopharyngeal cancer were treated at the First Affiliated Hospital of Nanchang University. Of the 132 patients, 34 patients were treated with hemicricolaryngopharyngectomy (25.8%). A total of 11 patients were deemed suitable for modified IHMCF reconstruction who underwent hemicricolaryngopharyngectomy (32.3%), one of them was found have the nodes associated with the internal jugular vein and this procedure was abandoned during the surgery.
In our study, the mean dimensions of the skin paddle of the flap were 8.3 cm × 4.0 cm (mean surface area, 33.2 cm2). All of the flaps survived well. No total or partial flap necrosis was noted in any case, and there were no complications at the donor site. Wider excision was carried out intraoperatively on 3 patients in whom intraoperative frozen section showed positive margin. In 4 of the patients’ flaps, the infrahyoid muscles were not only drained by the superior thyroid vein but also by the extra drainage vein during the surgery. The anatomic results of the reconstructed laryngopharynx were good, and the flaps showed good motility and pliability on flexible laryngoscopy. Cervical closure was performed without tension. Pharyngocutaneous fistula occurred in 1 patient (no. 10) whose fistula had closed spontaneously under conservative management. Postoperative radiation was performed in 7 patients. One patient (no. 8) died of tongue base recurrence at 12 months postoperatively. One patient (no. 6) had metachronous esophageal cancer at 12 months postoperatively and died after palliative chemoradiotherapy. To date, the remaining patients have all survived without tumor recurrence.
Oral intake was introduced at 2 weeks postoperatively, and removal of the nasogastric tube was performed on an average of 16 days after surgery. In one patient, the tube feeding time was prolonged because of a fistula that was treated by dressing changes. Finally, all of the patients were completely independent from nasogastric tube feeding and showed favorable swallowing results, and all could vocalize postoperatively. Speech function was roughly assessed, and the speaking capacity was good in all cases; that is, the patients could produce phonemes better compared with their presurgery abilities. The speech and swallowing outcomes seemed acceptable in all of patients postoperatively.
Six patients were decannulated despite partial resection of the cricoid, and 5 of them received radiation therapy postoperatively. The average time until tracheotomy weaning was 7.5 months (range, 1-10 months). All the patients had implemented tracheotomy, 4 patients had postoperative laryngeal stenosis, and 2 of them were completely dependent of endotracheal tube breathing. If the tube was blocked, it can cause severe tachypnea, and the other 2 patients’ tubes were blocked during rest on account of mild dyspnea. Because there is no staging system for laryngeal stenosis, we classified the severity of our cases on the basis of symptoms. On this aspect of laryngeal stenosis, flexible laryngoscopy showed that in these patients the glottis breadth is not enough, flap bloated, scar formation, it can causing some patients that they cannot be completely detached. Laryngeal stenosis is a challenging condition facing the laryngeal surgeon. In our study, treatments to correct the postoperative laryngeal stenosis contain conservative management (oxygen supplementation), montgomery T-tube insertion.
Flexible laryngoscopy showed that the flaps survived well, and functioning of the laryngopharynx, following reconstruction with a modified IHMCF after hemicricolaryngopharyngectomy, was excellent (Figure 5). There was no sign of stenosis in the newly reconstructed laryngopharynx. The modified IHMCF was harvested after neck dissection and the donor site was primary closed with good appearance (Figure 6).
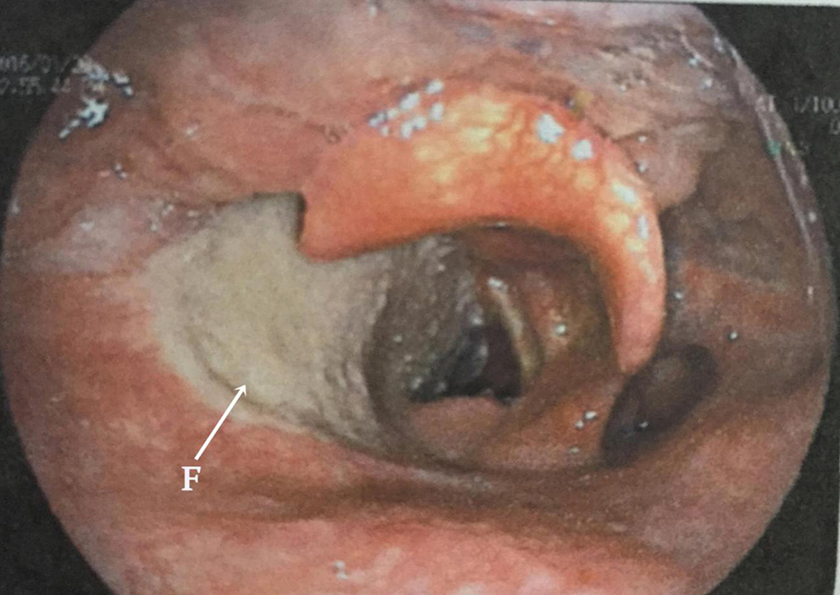
Flexible laryngoscope view 1 month postoperatively showing the modified infrahyoid myocutaneous flap (F) survived well; there is no stenosis sign of the new glottis.

The donor site was closed primarily. A, Frontal view. B, Lateral view.
Discussion
Total and conservative surgeries continue to be the treatments of choice for hypopharyngeal cancer, and the surgical defect frequently requires some forms of reconstruction. Recently, conservative laryngopharyngectomy was widely used for hypopharyngeal cancer, with preservation of laryngeal functions. 11,12 In this study, our patients had all undergone vertical hemicricolaryngopharyngectomy. Special attention should be given to preserving the integrity of alimentary and functional outcomes after surgery. Several flaps are available to reconstruct laryngopharyngeal defects resulting from ablative surgery of hypopharyngeal cancer, including pedicled (eg, infrahyoid myocutaneous or pectoralis major or platysma) or free (eg, anterolateral thigh or radial forearm) flaps, among other modalities; different reconstructive strategies have their own advantages and disadvantages. The choice of an appropriate reconstructive flap should be driven by the defect size and volume, donor site factors, reliability of the flap, patient characteristics, and patient and surgeon preferences. Reconstructive strategies need to be tailored to each individual patient.
Currently, the free flap is a common method employed for the reconstruction of partial hypopharyngeal defects, with favorable results achieved postoperatively. 13 The most common defect site for free tissue flap transfer is the oral cavity, followed by the hypopharynx/larynx, which is commonly reconstructed by the radial forearm free flap. 14 The microvascular free flap shows good versatility and reliability in reconstruction; however, it carries significant risks, including donor site morbidity, free flap failure, a significant learning period, and longer operative times and hospital stays. 14 Furthermore, not all patients are considered suitable for microvascular procedures, particularly elderly patients with serious general comorbidities. 9
The pectoralis major myocutaneous flap (PMMF) is still considered a good method for head and neck reconstruction. 13,15 Advantages of the PMMF include its ease of dissection, reliable blood supply, and ample volume of tissue to repair large defects, as well as the ability of the muscle pedicle to protect the neck vessels after neck dissection. However, the PMMF also has some disadvantages: excessive soft tissue thickness, an inferior final aesthetic result, and breast asymmetry in females. 4,13,16 The PMMF is too bulky and rigid, leading to possible speech impediment and poor voice rehabilitation; conversely, the IHMCF is thinner and more pliable. Since Wang et al reported using IHMCFs for head and neck reconstructions in 1986, the IHMCF became increasingly known and accepted thereafter. Although the IHMCF is not as fashionable as free flaps and the PMMF, its use in laryngopharyngeal reconstruction has unique advantages and deserves consideration in certain patients.
Although in 1986 Wang et al 5 first reported the flap for head and neck reconstructions, using this flap in reconstruction of the laryngopharyngeal defect is less popular. We had created a 3-dimensional reconstruction of the laryngopharyngeal defect by using of our own designed IHMCF, and it can reduce postoperative aspiration by rebuilding a new pyriform sinus, and no one had published this modified design before. Use of the IHMCF in head and neck reconstruction is generally successful; it has been used to reconstruct medium-sized defects in the oral cavity (69.8%), oropharynx (21.1%), hypopharynx (4.9%), and larynx (2.2%). 4,15,17 Additionally, the infrahyoid myofascial flap is effective to prevent postoperative pharyngocutaneous fistula formation after total (pharyngo)laryngectomy. 18 Several advantages of this flap are summarized as follows: it is thinner and more pliable than the PMMF; contrary to the free flap, there is no need for microsurgical expertise and instruments (and it is less time consuming); neck dissection can be finished simultaneously by one surgical team, and the donor area can undergo primary closure without additional incision; the anatomical region is familiar to head and neck surgeons, such that harvesting of the IHMCF can be performed quickly and easily; there is no need to change the patient’s position during the surgery; due to the proximity of the donor site to the defect, the flap can be easily transferred without damage of the pedicle; elderly and debilitated patients are considered more suitable for this flap reconstruction; aesthetic and functional outcomes are favorable; and, when complications develop, they are easy to manage. 6,7,9,15,17,19 In addition, the modified IHMCF can create a 3-dimensional reconstruction of the laryngopharyngeal defect.
The disadvantages of the IHMCF include dimensional limitations that make the flap inadequate for large-sized and complex defects; its vascular pedicle is in close proximity to lymph nodes that may be affected by occult lymph node metastasis (such that the vascular pedicle flap needs to be skeletonized meticulously), and necrosis can occur due to venous drainage problems, where venous drainage can be variable and insufficient (thus, for harvesting the flap, we need to preserve the drainage veins as much as possible to avoid the need to reconstruct less reliable areas). 6,7,15,17 To increase this flap’s venous drainage and improve the cosmetic results, various technical modifications were proposed by Dolivet et al 20 and Peng et al 15 ; they introduced a modified method of neck incision and preservation of the anterior jugular vein, respectively. In this study, we designed a modified incision according to the laryngopharyngeal defect after tumor ablation, because we had observed aspiration problems without technical modifications in 2 former patients. Consequently, the skin paddle was divided into 3 areas: area B was folded to straddle the aryepiglottic fold and part of the postcricoid region, area A reconstructed defects of the laryngotracheal cavity, and area C reconstructed defects of the pyriform sinus and lateral pharyngeal wall. All of our patients were completely independent from nasogastric tube feeding and showed favorable swallowing results after an average of 16 days postoperatively; however, in 1 patient, the tube feeding time was prolonged because of a fistula that was treated by dressing changes. We suspect that this modified incision can reduce postoperative aspiration complications and may increase the chance of decannulation; however, further study is needed to confirm this.
In our series, the IHMCFs of 4 patients were drained by an extra drainage vein, in addition to the superior thyroid vein, during the surgery. The extra drainage vein had a diameter of 1.2 mm (min: 1.0 mm, max: 1.5 mm), and it was drained by the internal jugular vein (Figure 2). In our opinion, it is essential to preserve the extra drainage vein to prevent the problem of insufficient venous drainage.
In our cases, all of the flaps survived well, and only one patient developed a pharyngocutaneous fistula, which had closed spontaneously with conservative management. Although the postoperative speech and swallowing abilities of our patients were only roughly assessed, the outcomes seemed acceptable in all cases. Six patients were successfully decannulated, among whom 5 received radiation therapy postoperatively. We speculate that postoperative radiation therapy could increase the chance of decannulation and may be related to muscular atrophy of the IHMCF, providing good ventilation in the new glottis.
Flexible laryngoscopy showed that the modified IHMCFs survived well, and there was no sign of stenosis in the new glottis (Figure 5). The IHMCF reconstruction proved to be a reliable and convenient procedure for treating laryngopharyngeal defects in our series, but further studies including more cases and long-term follow-up periods are needed to verify the preservation of laryngeal functions, as well as the oncologic safety of modified IHMCF reconstruction for laryngopharyngeal defects.
Conclusion
For laryngopharynx reconstruction after hemicricolaryngopharyngectomy, the modified IHMCF is a viable, convenient, and time-efficient reconstructive method. The IHMCF does not require 2 surgical teams or changes in the patient’s position during the surgery. In this study, the patients were carefully chosen in accordance with the exclusion criteria, and favorable functional and control outcomes were seen along with high patient satisfaction.
Footnotes
Authors’ Note
This study was reviewed and approved by the Review Board for Human Studies of the First Affiliated Hospital of Nanchang University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.