
Abstract

A 65-year-old diabetic man was referred to our hospital with left facial numbness, headache, and malaise approximately 2 weeks’ duration. Initially, his blood glucose level and HbA1c level were measured at 592 mg/dL and 12.6%, respectively. With strict control of blood sugar, antibiotic therapy was started because of suspected bacterial sinusitis on initial brain magnetic resonance imaging (MRI). His symptoms seemed to improve, but the facial pain and headache were suddenly aggravated at 2 weeks of admission. He was consulted to our department. Endoscopic examination revealed the black eschar in the inferior turbinate (Figure 1). Rechecked MRI showed total lack of enhancement (black turbinate sign) of the inferior turbinate of left side on T1-weighted image (Figure 2). Under general anesthesia, the patient underwent endoscopic surgery with wide excision of the necrotic tissue. Histopathologic examination demonstrated angioinvasive hyphae with characteristics of mucormycosis (Figure 3). After surgery, he finished a 6-week course of amphotericin and he remained symptom-free 18 months later.
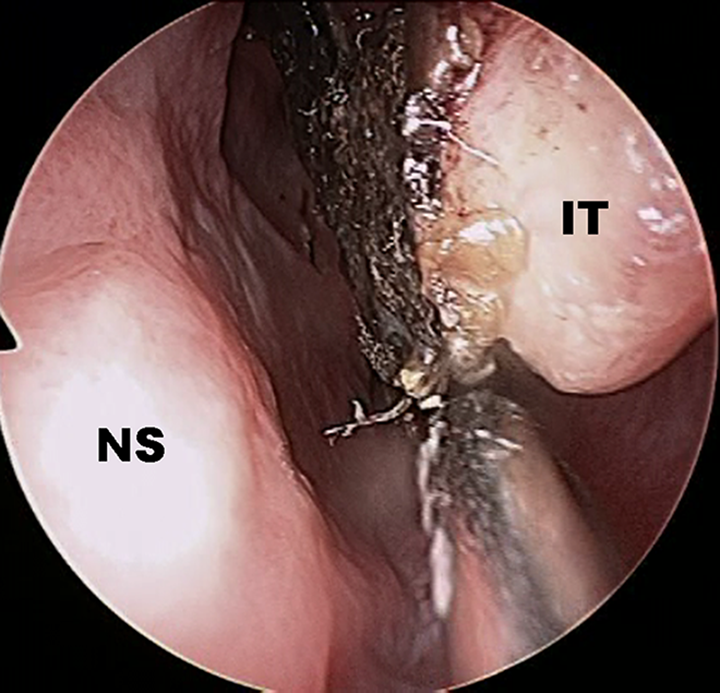
On endoscopic findings of left nasal cavity, there was black eschar in inferior turbinate. IT indicates inferior turbinate; NS, nasal septum.

An axial T1-weighted magnetic resonance imaging (MRI) demonstrates nonenhancing left inferior turbinate, “black turbinate sign” (arrows). Asterisk: right-side inferior turbinate.
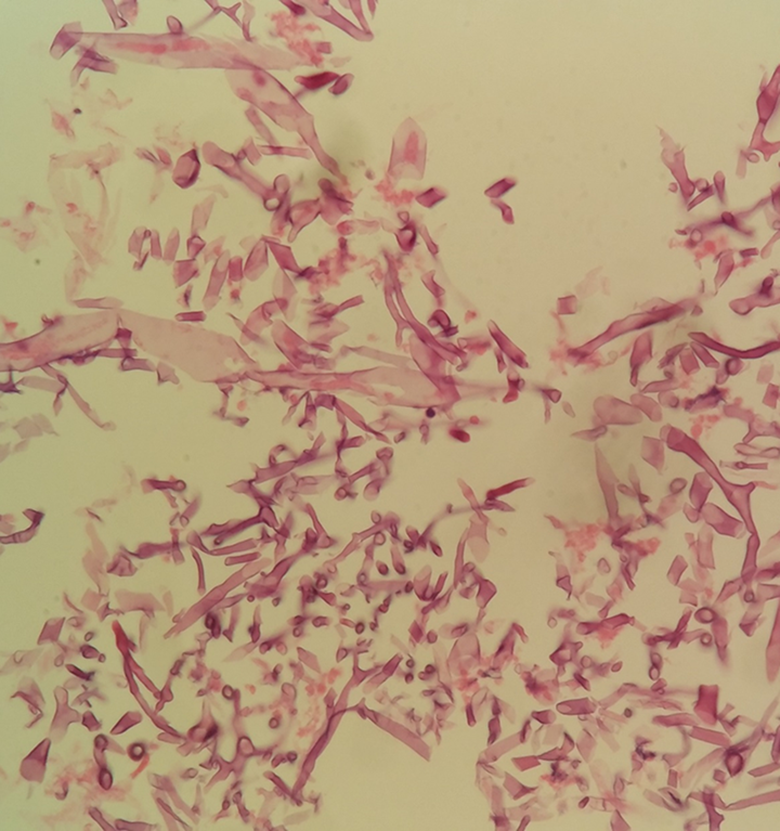
Pathologic specimen shows broad-based, ribbon-like, and nonseptate hyphae with wide-angle branch (H&E, ×400).
Mucormycosis is an acute opportunistic, angioinvasive, and devastating fungal infection which is associated with high mortality rates. 1 There has been a significant increase in incidence over the last 2 decades. 2 Early and accurate diagnosis of invasive mucormycosis remains a challenge for physicians. However, patients with invasive mucormycosis initially present with nonspecific symptoms and signs, leading to delays in diagnosis and imaging modalities and cultures are not usually useful for diagnosis. 2 –4 Mucor organisms have the propensity of angioinvasive hyphae that results in infarction of the involved tissue (especially turbinate), leading to the “dry gangrene” appearance due to the extensive angioinvasion with resultant vessel thrombosis. 3 As a result, diseased tissue is prone to necrosis, devitalization, and finally the development of black eschars on endoscopic findings. 5 This black eschar appears on MRI as contiguous foci of nonenhancing tissue, so-called “black turbinate sign,” which presents in early stages in nasal mucormycosis and can aid in earlier detection. 3,6 So, recognition of this unusual finding may lead to the early diagnosis and subsequently prompt treatment of this rare but deadly disease. 3 On the basis of the important points described above, physicians should keep in mind that invasive nasal mucormycosis can be suspected when the inferior turbinate appears black upon endoscopic examination of the nasal cavity or when black turbinate sign is found on MRI.
Footnotes
Authors’ Note
S.C.L. and K.S.K. contributed equally to this manuscript as corresponding author. The patient’s permission was obtained.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Chung-Ang University Research Scholarship Grants in 2017.