
Abstract
The aim of this study is to compare the delivery site of topical drugs using the short nozzle and the long nozzle. Fourteen fresh frozen cadaver heads were obtained. All cadaver specimens underwent bilateral endoscopic wide maxillary antrostomy, frontal sinusotomy, and complete sphenoethmoidectomy. The right nasal cavity of each cadaver was sprayed with radiolabeled saline using the short nozzle (short nozzle group), while the left nasal cavity was sprayed using the long nozzle (long nozzle group). The distribution of radioactive saline within the sinus cavities was determined using single-photon emission computed tomography/computed tomography. The distribution of the radiolabeled saline in reference with the maxillary line, vestibule, maxillary, ethmoid, sphenoid, and frontal sinus was compared between the 2 groups using Fisher exact test. The number of specimens that demonstrated radioactivity above the maxillary line is higher in the long nozzle group (14 cadavers, 100%) compared to short nozzle group (9 cadavers, 64.3%; p = .02). There are fewer specimens that demonstrated deposition of radioactive saline in the vestibule in the long nozzle group (6 cadavers, 42.86%) compared to short nozzle group (13 cadavers, 92.86%; P = .006). Compared to short nozzle group, there are more specimens demonstrating radioactivity in the maxillary, ethmoid, sphenoid, and frontal sinus in the long nozzle group, but the differences were not statistically significant (p = 0.241, 0.347, 0.126, 0.5). Compared to short nozzle, long nozzle more frequently delivers intranasal drugs beyond the maxillary line and less frequently in the vestibule. These findings support the hypothesis that the use of long and narrow nozzle, instead of the conventional short nozzle, can improve sinonasal drug delivery in post-endoscopic sinus surgery nose.
Introduction
Intranasal corticosteroids (INCS) play a significant role in the medical management of chronic rhinosinusitis (CRS). Several evidence-based guidelines 1,2 concur in recommending its use to improve objective and subjective outcomes in CRS with nasal polyposis. There is evidence supporting the benefit of INCS in CRS without nasal polyposis but this has been an inconsistent finding. 1,2
One of the main advantages of INCS is the potential to achieve high concentration to the ciliated sinonasal mucosa. However, the complex sinonasal anatomy, aggravated by the pathology, serves as a barrier to effective sinonasal drug delivery. 3 The delivery of the INCS from the bottle to the sinonasal mucosa is not ensured by the direct insertion of a device to the nostril. Thus, the effectiveness of INCS is not maximized.
Effective sinonasal drug delivery requires adequate access and appropriate delivery method. To provide adequate access, sinus surgery is required. 4 Very minimal drug is delivered to nonoperated sinuses. 5 After sinus surgery, sinonasal drug delivery is improved. 5 Sinus surgery not only removes the disease burden but also provides access for the INCS to the reach the sinuses, thus increasing the effectiveness of INCS. 1,6,7
Different devices have been used to deliver INCS postoperatively. Intranasal sprays are commonly used because of the ease of application and availability of many INCS in this formulation. 4 Intranasal sprays also offer high reproducibility of delivered drug dose. 4 However, most commercially available intranasal spray devices have short nozzles. Commercially available short nozzles usually deliver drugs in the vestibule and have limited distribution to the sinus mucosa. 3,7,8 It is our hypothesis that a longer and narrower nozzle can deliver INCS to the sinus mucosa up to the olfactory cleft. The aim of this study is to compare the delivery site of INCS using the short nozzle and the long nozzle.
Patients and Methods
Cadaver Specimens
The hospital ethics committee approved this study. Fourteen fresh frozen cadaver heads were obtained. The cadaver specimens were left to thaw for 48 hours at room temperature before sinus dissection and spraying with radiolabeled saline.
Cadaver Dissection
All cadaver specimens underwent bilateral endoscopic wide maxillary antrostomy, frontal sinusotomy, and complete sphenoethmoidectomy. The cadaver dissection was performed by multiple practicing otolaryngologists who were instructed on the technique, supervised, and assisted by the first and third authors during hands-on training course on endoscopic sinus surgery. After dissection, all cadaver heads were inspected to ensure completeness of endoscopic sinus surgery. Cadavers with septal deviation were excluded from the study.
Administration of Radiolabeled Saline
The contents of a commercially available steroid nasal spray bottle was emptied and replaced with 10 mL of normal saline mixed with 15 mCi of Technetium-99m. A commercially available short nozzle (Figure 1) and a custom-made long nozzle (Figure 2) were connected to the nasal spray bottle.

Short nozzle spray.
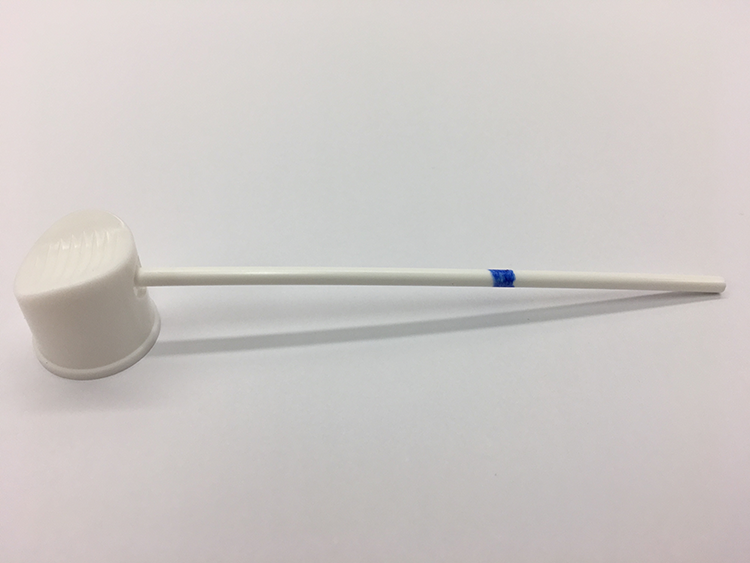
Long nozzle spray.
Each cadaver head was secured in a position with the faceup oriented parallel to the ground. Priming of nasal sprays was done by releasing 2 to 3 sprays until fine mist appeared. To minimize bias, only one author administered the radiolabeled saline on both sides in all the cadaver heads.
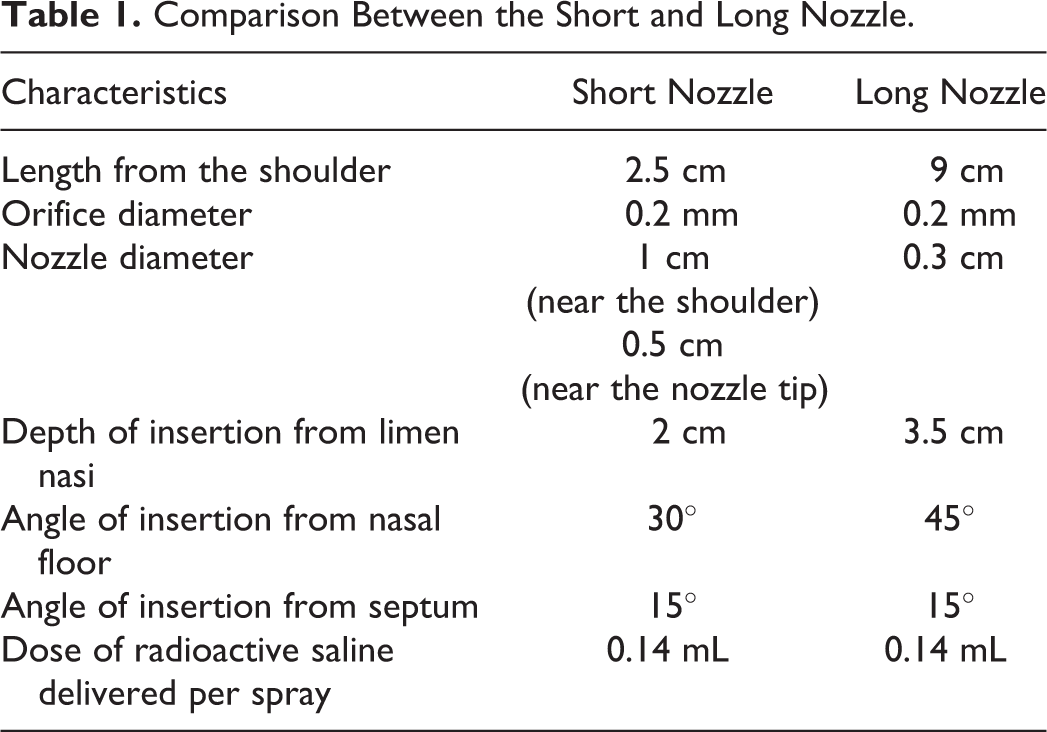
The right nasal cavity of each cadaver was sprayed using the short nozzle (short nozzle group), while the left nasal cavity was sprayed using the long nozzle (long nozzle group). Table 1 summarizes the characteristics of the short and long nozzle. Both nozzles have similar nozzle orifice diameter. On the right side, the short nozzle was inserted 2 cm into nasal vestibule until its shoulder. The short bottle was angled at 45° from the nasal floor and 15° from the nasal septum. Two spray puffs were administered delivering 0.14 mL of radioactive saline per spray. On the left side, the long nozzle was inserted 3.5 cm from the limen nasi, at 45° angle from the nasal floor and 15° from the nasal septum. The spray bottle was held upside down and 2 spray puffs were administered delivering 0.14 mL of radioactive saline per spray.
Comparison Between the Short and Long Nozzle.
Assessment of Radiolabeled Saline Using Single-Photon Emission Computed Tomography/Computed Tomography
Five minutes after the administration of radiolabeled saline, single-photon emission computed tomography/computed tomography (SPECT/CT; Symbia Intevo; Siemens, Washington, D.C.) was performed and assessed by a blinded nuclear radiologist to determine delivery of radioactive saline within the sinonasal regions.
Outcome Measure
The primary outcome is the distribution of the radiolabeled saline in reference with the maxillary line. Maxillary line is defined as the axial line passing through M point at the level of superior margin of maxillary sinus ostium. Secondary outcomes are the distribution to the following sinonasal regions: vestibule, maxillary sinus, ethmoid sinus, sphenoid sinus, and frontal sinus.
Single-photon emission computed tomography/computed tomography/CT images are assessed qualitatively by an independent nuclear radiologist. Results are categorized as positive or negative. For the primary outcome, positive result means the presence of >10% radioactivity detected above the maxillary line, while negative result means ≤10% radioactivity detected above the maxillary line. For the secondary outcome, positive result means presence >10% radioactivity detected in the sinonasal region being studied, while negative result means ≤10% radioactivity detected in that sinonasal region. Figure 3 shows the percent radioactivity scheme and the representative SPECT/CT images with their corresponding assessment.
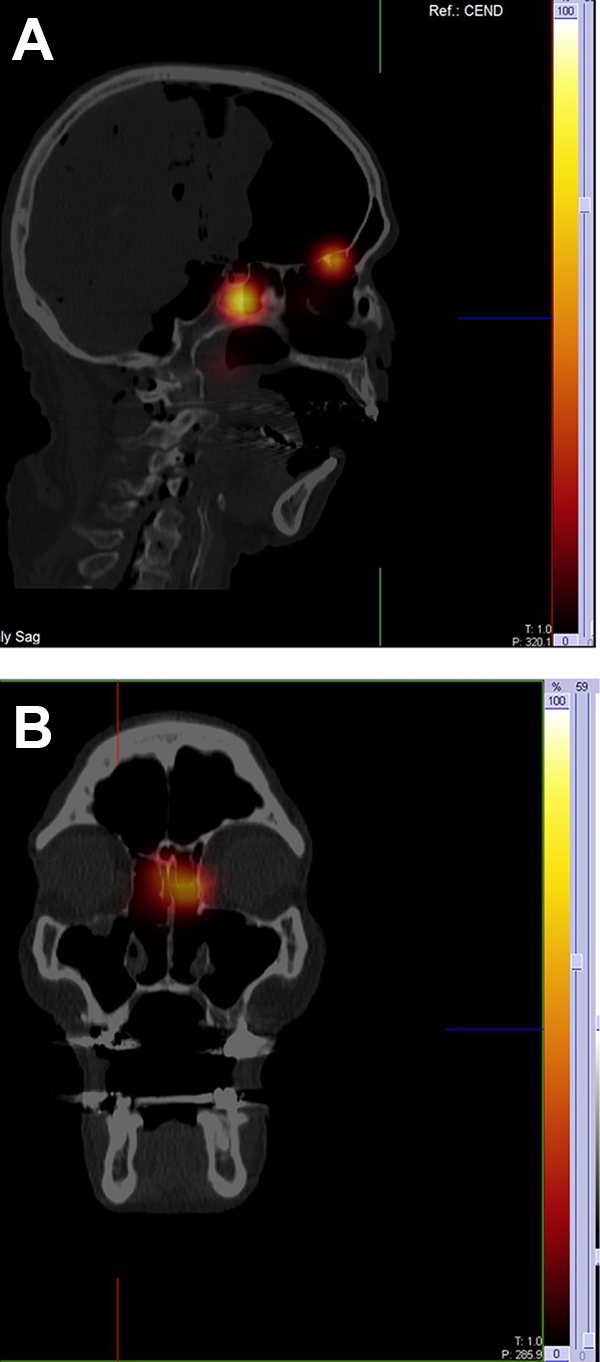
Percent radioactivity scheme and representative single-photon emission computed tomography/computed tomography (SPECT/CT) images of various cadaveric heads following administration of radiolabeled saline and their corresponding results. Positive result means presence >10% radioactivity detected in the sinonasal region being studied, while negative result means ≤10% radioactivity detected in that sinonasal region. A, Sagittal cut showing positive result in the sphenoid and ethmoid sinus, and negative result in the frontal sinus. B, Coronal cut showing positive result in the left ethmoid and negative result in the right ethmoid and bilateral maxillary sinus.
Statistical Analysis
Data were treated as nominal and analyzed using Fisher exact test. A p value <.05 was considered statistically significant.
Results
All 14 cadaver heads were well preserved through freezing with a near normal quality of the soft tissue. All had negative serological testing for infectious diseases. No other medical history was available. All cadaver specimens were adults by visual inspection.
The nasal cavity demonstrated evidence of radioactivity on all SPECT/CT performed after nasal spray. Figure 4 shows representative SPECT/CT images following administration of radiolabeled saline and their corresponding assessment.
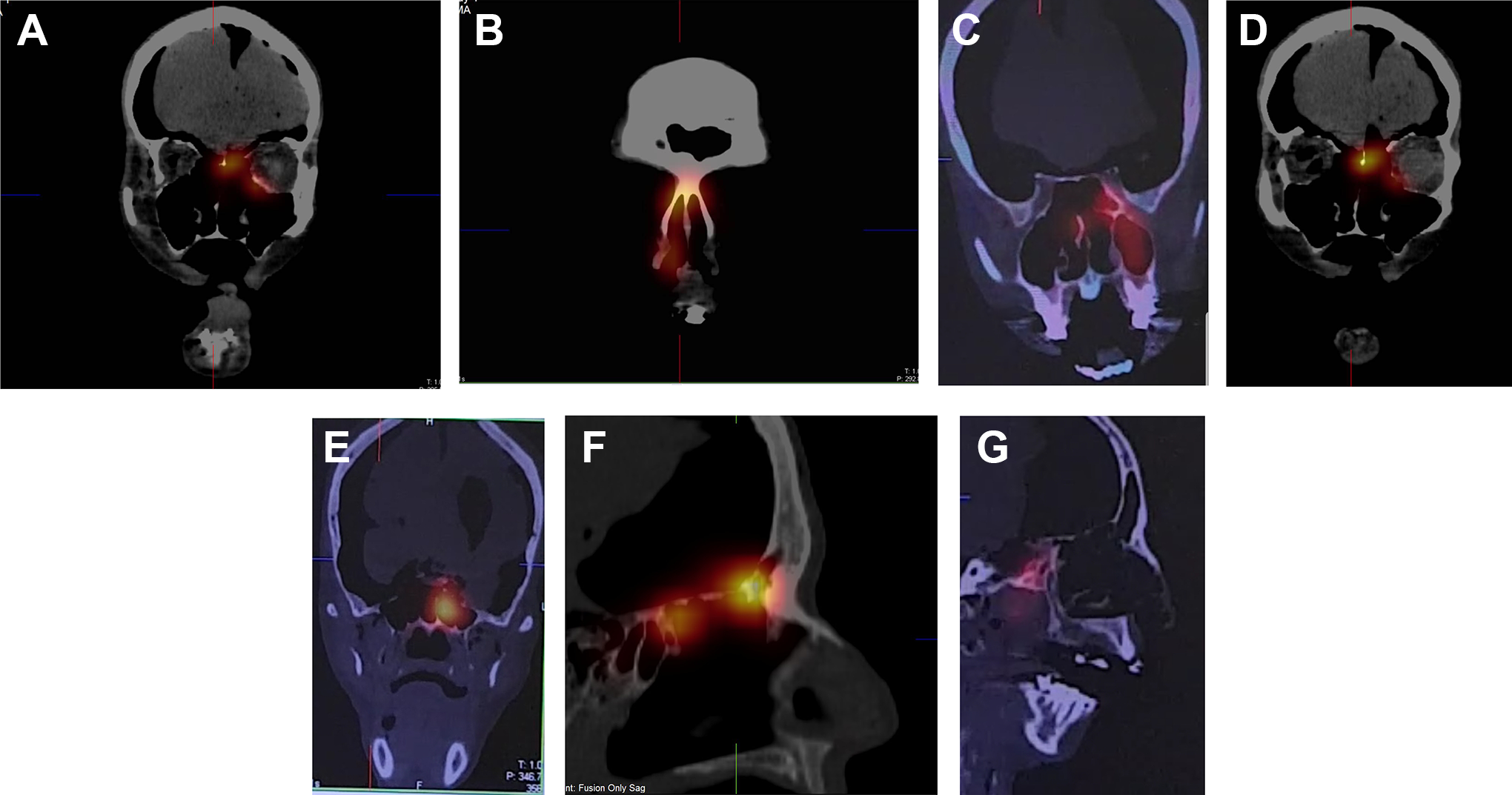
Representative single-photon emission computed tomography/computed tomography (SPECT/CT) images of various cadaveric heads following administration of radiolabeled saline and their corresponding results. Coronal cut at the maxillary sinus ostium (A), the left shows positive result, and the right shows negative result. Coronal cut at the nasal vestibule (B), the left shows negative result, and the right shows positive result. Coronal cut at the maxillary sinus (C), the left shows positive result, and the right shows negative result. Coronal cut at the area of the ethmoid sinus (D), the left shows positive result, and the right shows negative result. Coronal cut at the sphenoid sinus (E), the left shows positive result, and the right shows negative result. Sagittal cut at the frontal sinus showing positive result (F) and negative result (G).
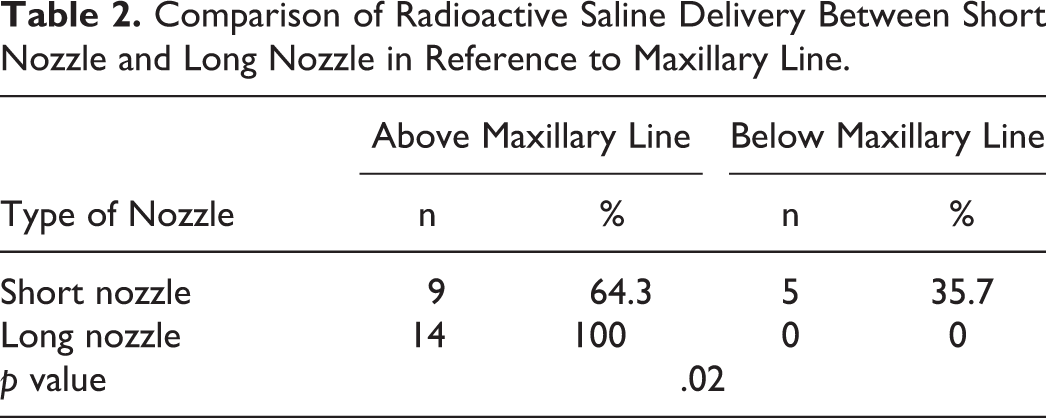
In the short nozzle group, 5 (35.7%) cadavers demonstrated radioactivity limited below the maxillary line, while 9 (64.3%) cadavers demonstrated radioactivity above the maxillary line, reaching the cribriform plate. In the long nozzle group, all 14 (100%) cadavers demonstrated radioactivity above the maxillary line, reaching the cribriform plate. The number of cadavers demonstrating radioactivity above the maxillary line is significantly higher in the long nozzle group compared to the short nozzle group (p = .02; Table 2).
Comparison of Radioactive Saline Delivery Between Short Nozzle and Long Nozzle in Reference to Maxillary Line.
Thirteen (92.86%) cadavers demonstrated radioactivity in the vestibule in the short nozzle group. This is significantly higher compared to 6 (42.86%) cadavers demonstrating radioactivity in the vestibule in the long nozzle group (p = .006; Table 3).
Comparison of Radioactive Saline Delivery Between Short Nozzle and Long Nozzle in Different Sinonasal Regions.

Compared to short nozzle group, more cadavers demonstrated radioactivity in the 4 individual sinuses in the long nozzle group, but this is not statistically significant (Table 3). The ethmoid and sphenoid sinuses are the most frequently delivered sites (10 cadavers, 71.43%) in the long nozzle group, while the ethmoid and frontal sinus are the most frequently delivered sites (8 cadavers, 57.14%) in the short nozzle group. In both groups, maxillary sinus least demonstrated radioactivity. No cadaver in the short nozzle group, and only 2 (14.29%) in the long nozzle group demonstrated radioactivity in the maxillary sinus.
Discussion
The clinical effect of intranasal corticosteroid is limited by its inadequate distribution to the sinus mucosa. 3,9 In order to improve sinonasal drug delivery, adequate access must be achieved and appropriate delivery method must be utilized. It is well established that sinus surgery removes anatomical barriers providing more access to the sinus mucosa and olfactory cleft. 1,2,6 -8,10 This translates clinically to greater polyp size reduction in patients who underwent sinus surgery with postoperative INCS compared to patients who received INCS but did not undergo sinus surgery. 1,2,11
Postoperatively, intranasal sprays are commonly used because of ease of administration. 3 Many INCS are available in spray formulation. 3 Despite these advantages, sprays have been shown to have less sinus delivery compared to sinus delivery methods such as direct sinus cannulation or postoperative sinonasal irrigation. 11,5 The proportion of INCS delivered to the sinuses has been measured to be less than 1% delivered to the nasal cavity. 8 Even after surgery, nasal sprays have inconsistent sinus distribution. 8 However, these studies use the commercially available spray with short nozzle. 5,12
Short nozzles can only be inserted intranasally until the spray shoulder depositing a large portion of INCS into the region anterior to the nasal valve area called the vestibule. 3,13 In a computational fluid dynamics study simulating nasal spray parameters of commercially available nasal sprays, >90% of the drug particles were deposited in the nasal vestibule. 14 The nasal vestibule is lined by nonciliated squamous epithelium, has no mucociliary action, low vascularization, and poor permeability. 13,15 Thus, the anteriorly deposited drugs will drip out of the nose and will not be absorbed. 16 In this study, the radiolabeled saline was delivered to the vestibule in 13 (92.86%) cadavers in the short nozzle group (Figure 4B). Five of these cadavers demonstrated radioactivity below the maxillary line. Another study 17 reported <20% of topical drugs delivered beyond the vestibule and no drug delivered to the sinuses, when using intranasal spray with short nozzle.
In order to minimize anterior INCS deposition to the vestibule, a longer and narrower nozzle was designed to replace the short nozzle. In this study, the radiolabeled saline was delivered to the vestibule in 6 (42.86%) cadavers in the long nozzle group. In addition, the radiolabeled saline reached above the maxillary line, reaching up to the cribriform plate (Figure 4A) in all cadavers in the long nozzle group.
Several studies 14,17 suggested that the key to optimize nasal drug delivery is to bypass the nasal valve area, which is an important anatomical barrier in sinonasal drug delivery. The nasal valve area has a limited dimension and mismatched geometry. 3 It is the narrowest segment of the nasal passage measuring 0.54 ± 0.13 cm2 each side in acoustic rhinometry studies. 18 In addition, the triangular nasal valve opening does not match the circular plume created by the spray. Once a spray is actuated, a hollow spray cone is formed with drug particles mainly at the periphery. 7 Particles at the lower and wider part of the triangle will penetrate the valve, while the majority of drug particles will impinge anterior to the nasal valve area and drip out. 7
The nasal valve area is located 2 to 3 cm from the nasal opening. 18 A short nozzle, even if inserted deeply up to 2 cm, will not be able to bypass this area. Because the long nozzle is inserted 3.5 cm from the tip, it bypasses the nasal valve area, ensuring that intranasal medication will reach the sinonasal mucosa.
Nozzle orifice diameter is another factor affecting nasal drug distribution. A smaller orifice diameter produces a narrower spray cone angle which allows greater percentage of droplets to penetrate the nasal valve. 14 Larger orifice diameter creates wider spray cone angle and larger spray pattern which deposits majority of the particles anterior to the nasal valve region. 14,19,20 In order to control for the confounding effect of the nozzle orifice diameter, the 2 nozzles in this study have similar orifice diameter.
Anatomic variations such as septal deviation can also affect drug deposition. Drug delivery is significantly diminished on the side of obstruction. 21 Another study 22 showed that the correction of septal deviation improves nasal drug delivery. In order to minimize the confounding effect of septal deviation, cadavers that were included in the study have no septal deviation.
For INCS to be effective in CRS, it should be delivered to the sinonasal mucosa, which is lined mainly by respiratory epithelium, has very high vascularization and good permeability. 9 In this study, the delivery to the sinuses increased when long nozzle was used compared to short nozzle, although the difference is not significant.
Scintigraphic methods have been used to assess sinonasal drug delivery. 23 -27 Among the radiopharmaceuticals available, Tc99m is commonly used because of its short half-life of 6 hours, high-efficiency detection and low radiation exposure. 28 Intranasally administered Tc99m labeled solutions were commonly assessed using 2-dimensional (2D) γ scintigraphy. 25,26 However, planar scintigraphy provides 2D images without clear anatomic features especially the maxillary sinuses. 24,25 In this study, SPECT/CT was used to assess radiolabeled saline deposition. Single-photon emission computed tomography/CT has been recommended as the scintigraphic imaging of sinonasal drug distribution. 27 It provides a 3D image combining the radioactivity measured using SPECT and the detailed anatomic images using CT scan. This method is highly advantageous in evaluating the sinonasal region because the sinonasal anatomic subsites are very close to each other. Single-photon emission computed tomography/CT has been shown to accurately assess drug deposition. 27 Leclerc et al 27 compared the intrasinus deposition assessed using SPECT/CT to a reference lavage method. Results showed the SPECT/CT is in agreement with the reference method unlike 2D planar scintigraphy which often overestimates drug deposition in the nose. 27
For a nasal spray to effectively deliver INCS from the bottle to the sinonasal mucosa and olfactory cleft, an appropriately designed nozzle is needed. It should bypass the nasal valve area, which limits the delivery of intranasal drugs to the surgically opened sinus cavities. The use of a long nozzle can help bypass this area, reaching the regions above the maxillary line more consistently than the use of short nozzle.
The particle size and plume geometry, consequently nasal drug delivery, is affected by device properties and formulation properties. 5,29,30 In this study, only one type of short and long nozzle nasal spray is used. We recommend further studies using other short and long nozzle nasal spray with different device properties.
Nasal drug delivery is not only affected by device properties but also by formulation properties (viscosity and rheological behavior). Results in this study could be underestimated because water was used as the liquid component of the nasal spray device. Compared to drug formulations, water has lower viscosity at 1.28 centipoise. 29 Increased viscosity of the liquid formulation resulted to larger droplet size, narrower plume angle, lower spray pattern and less vestibule, and nasal valve deposition. 25,29 Further studies using liquid with viscosity similar to nasal formulations are recommended.
Clinical generalizations from this study are limited by the inability of cadaveric models to reproduce other physiological and patient-related factors. Mucociliary clearance, comfort of use, and patient handling also affect drug delivery of the INCS. 3,9,13 Further studies on live patients are recommended to assess patient comfort, safety, and reproducibility of the insertion depth and angles in clinical setting.
One modification in this study is that the cadaver heads were placed in a supine position instead of the usual head upright position. The head supine position was used for both short and long nasal sprays. There are limited data about the absorptive capacity of cadaver nasal mucosa to radiolabeled saline. Some radiolabeled saline may drip to the nasal vestibule after being deposited to the sinonasal mucosa. This would confound the results. In order to remove this possibility, the cadaver heads were placed in a supine position. One limitation of this head position is it could overestimate the deposition to the sphenoid sinus. Future studies using head upright position is recommended.
This study demonstrated that in post-endoscopic sinus surgery specimens, long nozzle could deliver radioactive saline above the maxillary line more frequently and less frequently in the vestibule, compared to short nozzle. These findings support the hypothesis that the use of long and narrow nozzle, instead of the conventional short nozzle, can improve sinonasal drug delivery in post-endoscopic sinus surgery nose. This suggests potential for product improvement.
Footnotes
Authors’ Note
The views expressed in the submitted article are of the authors and not an official position of any institution. Precious Eunice R. Grullo is now affiliated with Tarabichi-Stammberger Ear and Sinus Institute, Dubai, United Arab Emirates, Department of Otorhinolaryngology, College of Medicine, University of the Philippines - Philippine General Hospital, Manila, Philippines and Department of Otorhinolaryngology, Rizal Medical Center, Pasig, Philippines.
Acknowledgments
The authors thank the Nuclear Medicine staff for their assistance throughout the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.