
Abstract
Introduction:
Sialolithiasis is the most common pathology in the submaxillary gland. The introduction of minimally invasive techniques isolated or associated with sialoendoscopy is replacing glandular resection as a treatment. The conservation of the gland is justified by the recovery of function and a low recurrence rate. The rate of complications is lower in conservative techniques than in submandibular gland resection.
Patients and Methods:
Thirty-three patients with fixed stones in the hilum of the submaxillary gland were treated by transoral sialolitectomy between July 2015 and July 2018, demographic data of the patients such as the number of stones, size, time of hospital stay, complications, pre- and postoperative lingual nerve function, and lithiasis recurrence were collected.
Results:
The average volume of the stones was 1.02 cm. Complete removal of the stone was possible in 32 patients. All the patients were operated in the outpatient clinic. Seven (21%) patients reported some degree of alteration of the lingual nerve function, of which the only one presented a persistence of more than 4 weeks due to an inadvertent injury that required a microsurgical anastomosis.
Conclusions:
Transoral sialolitectomy is a reproducible technique with good results and lower complication rates than submandibular gland resection. Our results in the first 33 cases encourage us to maintain the combined techniques as standard in the treatment of submaxillary sialolithiasis. Current experience guides the definitive substitution of submandibular gland resection by conservative techniques in obstructive pathology.
Introduction
Lithiasis formation in the Wharton duct represents the most frequent cause of pathology in the submaxillary gland. Different authors estimate the global incidence of obstructive sialadenitis among 1.2 to 5.9 cases per 100 000 inhabitants. 1,2 During the last decades, and even today, the most extended therapeutic option for this pathology has been the submandibular gland resection (SGR). The presumption that the functionality of the glandular parenchyma is irremediably altered after the obstructive process and the hypothesis related to developing of new stones are the main arguments for the glandular resection. Submandibular gland resection is also a well-standardized technique with a low rate of complications and a low impact on the quality of life of patients, and reviews from a different group of authors have been shown that the technique is not risk-free. 3
Lithiasis located in the middle or distal portion of the Wharton duct has never been a problem and its resection, under local anesthesia, with or without partial removal of the sublingual gland, has been the usual treatment. However, lithiasis located proximally in the hilum, which appears more frequently than distal forms, 4 implies deeper and more complex approaches.
The introduction of sialoendoscopy techniques at the beginning of this century has laid the foundations of a change in the way of dealing with obstructive salivary pathology. Its application in the resection of large stones using combined approaches has allowed giving value to minimally invasive techniques described some decades ago. 5
This is the reason why in the next paper we review our experience in the transoral approach in submandibular gland lithiasis located proximally in the hilum as a valid alternative to the traditional SGR. Moreover, we describe the technique used, key points, results, and complications observed.
Patients and Methods
After the approval of the ethics committee of our hospital, all patients were included prospectively in the obstructive salivary gland pathology database of the main author between July 2015 and July 2018. During the study period, 45 patients come to our department with submandibular gland lithiasis located proximally in the hilum, 12 of them were operated using the traditional approach through an SGR. Eleven of these 12 patients were included in a study performed previously by the authors in the arm of SGR to compare both techniques. 6 Moreover, 1 patient was operated using the classic technique due to his preference and not included in this previous study.
Thirty-three patients were included in the final analysis. Again, 11 of the 33 patients were included in a previous study conducted by our group in the arm of transoral approach. 6 In all cases, both the transoral procedure and the possibility of requiring an SGR if it failed were explained. All of them had at least one proximal calculus at the level of the hilum of the submaxillary gland, and none had previously been operated on for salivary gland lithiasis.
In the preoperative visit to the clinic, lingual nerve function was evaluated in all patients. The variables included in the study correspond to the average number of lithiasis, the average size of the lithiasis, average hospital stay, lingual nerve alteration, and complications for the technique.
Transoral sialolitectomy was performed under general anesthesia with nasotracheal intubation in all patients. In one case due to cardiac pathology, general anesthesia was contraindicated, and mandibular and lingual nerve block associated with sedation was chosen. To expose the floor of the mouth, a Ferguson mouthpiece was placed on the contralateral side, and the assistant positioned at the patient’s head pull the tongue, showing the glandular hilum. Before incision, we infiltrated the area with local anesthesia and vasoconstrictor. Then the lithiasis was located either by palpation or transillumination using the optic, placed in front of the lithiasis in the Wharton duct. An area of mucous and submucosal lax tissue was resected with a fine-tipped electrosurgical device generating a window of broad access on the hilum. After this, we will discover the posterior part of the sublingual gland that we can resect or not according to the difficulty of the approach. Immediately under the soft submucosal tissue, through a blunt dissection, we will discover the path of the lingual nerve that constantly appears as a thick nerve with a high tolerance to manipulation. Locating the lingual nerve allows us to advance dissecting toward the Wharton duct that, following the gland, deepens and turns in an inferolateral direction over the mylohyoid. The location by palpation or transillumination at this point is essential since Wharton differentiation is not as immediate as in the case of the lingual nerve. Depending on the location of the obstruction, we must move the nerve medially (in our case more frequent) or laterally to access the lithiasis. At this time, the assistant’s collaboration pulling the tongue medially and pushing the gland simultaneously to make the glandular hilum prominent on the floor of the mouth makes the dissection easier. Once the lithiasis is located, we make an incision that shows the yellowish and usually irregular surface of the stone.
We extended the incision as necessary to extract the lithiasis with a 90° ear hook. Subsequently, through the orifice, we wash the duct with saline to eliminate possible remains, and we introduced a sialendoscope to explore all the ductal tree looking for other stones. We did not close the duct usually, both in a few cases we gave some lax points of approach of the mucosa, and we did not place a stent (Figure 1).
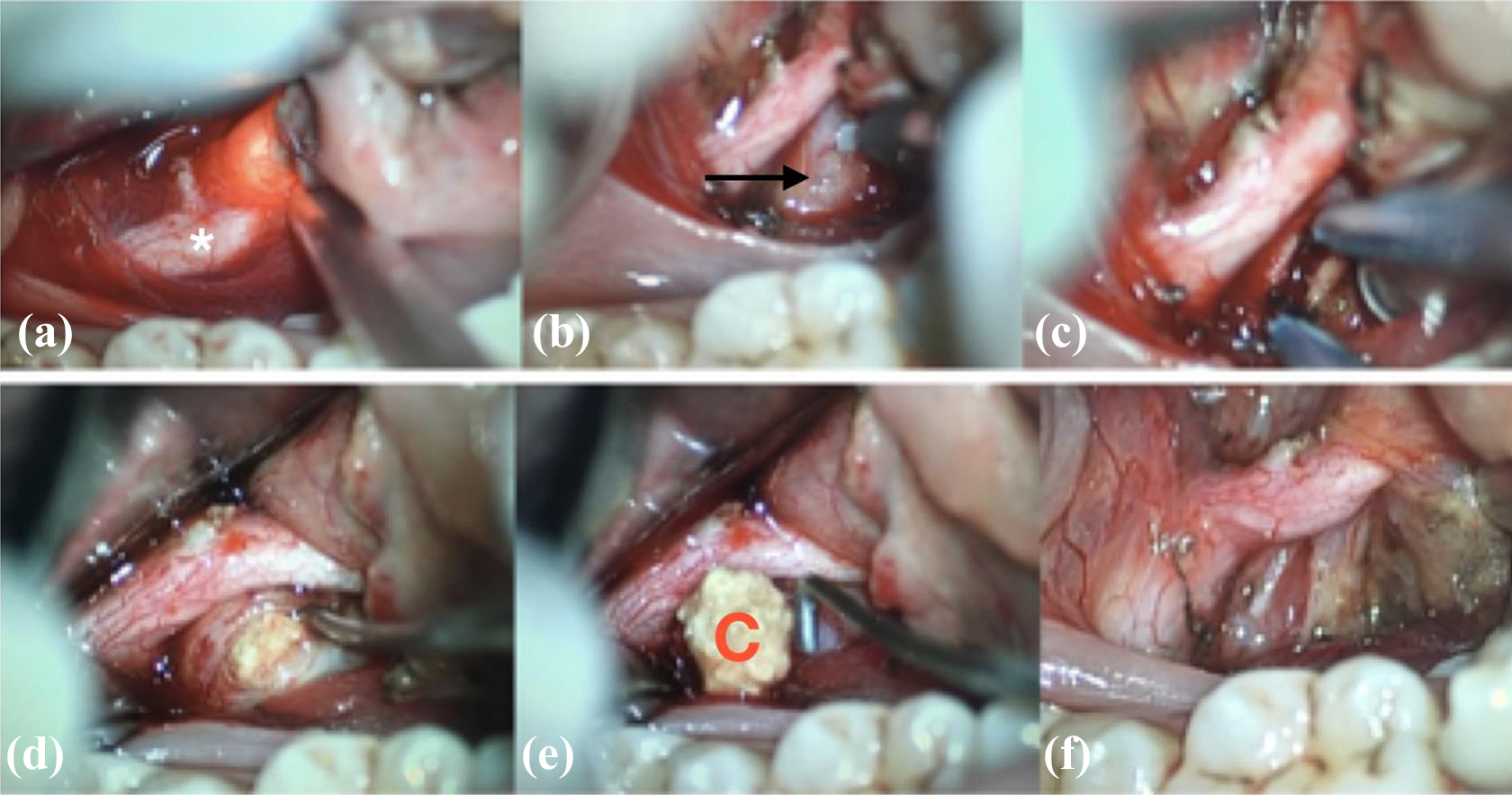
Floor of the mouth. Right side. Dissection steps: (a, b, and c): nerve identification. (d and e): lithiasis extraction. (f) Wharton duct opened. * = lingual nerve; black arrow = Wharton duct; C = calculi.
The statistical analysis was carried out using the JASP program, version 0.8.5.1 computer software (University of Amsterdam). The quantitative variables within the study are expressed as mean (standard deviation), the results are expressed as a total plus percentage.
Results
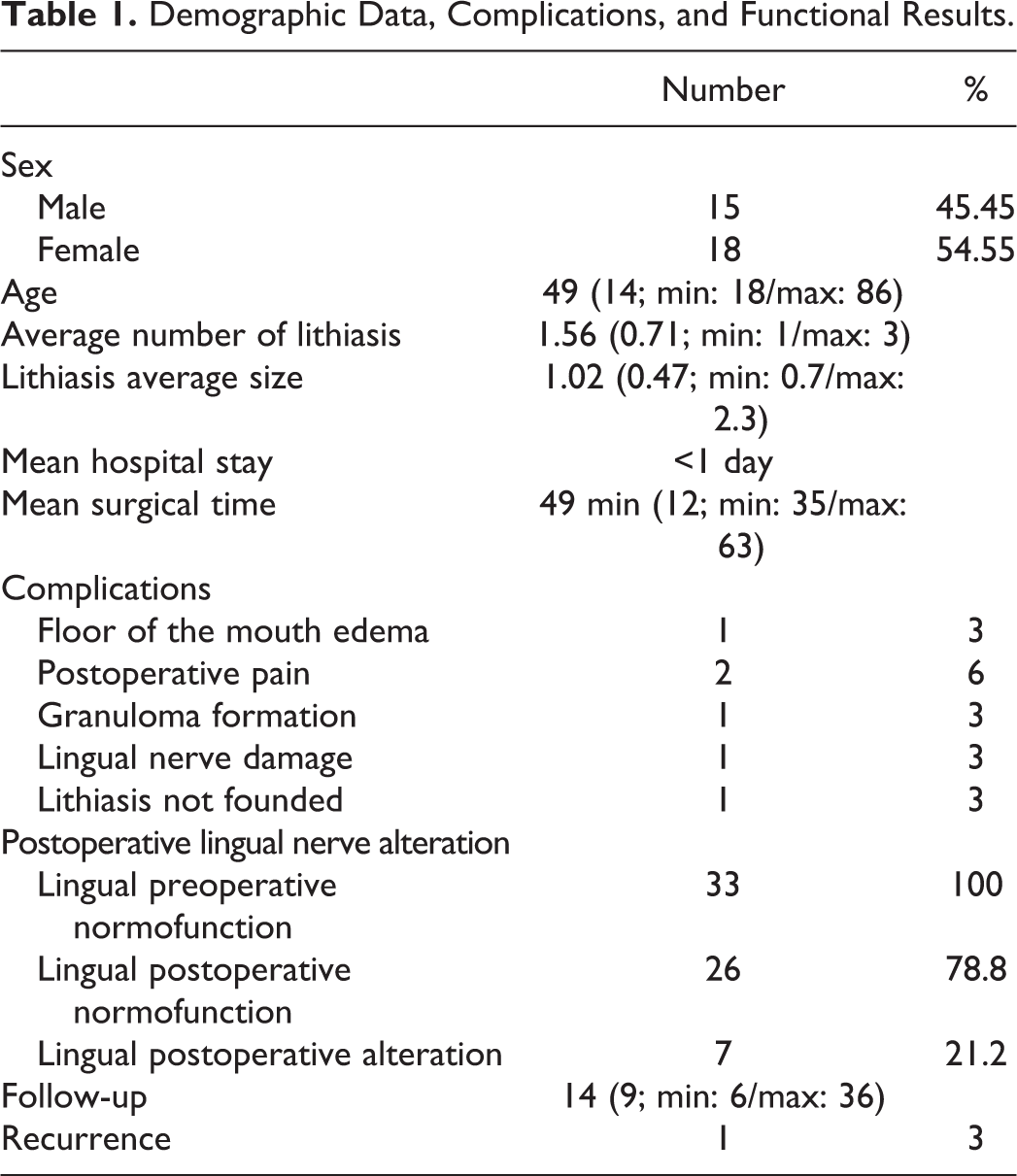
Thirty-three patients met the inclusion criteria. Sixteen (45.45%) were men and 18 (54.55%) were women, the average age was 49 years (14 years; min: 18/max: 86). The average number of stones in the sample was 1.56 (0.71; min: 1/max: 3), the average size of the stones was 1.02 cm (0.47 cm; min: 0.7/max: 2.3). All patients were discharged in the afternoon after surgery. In 7 (21.2%) patients, some degree of lingual nerve alteration was evidenced in the postoperative follow-up; in 1 of the cases, the loss of sensitivity was total due to an inadvertent section of the nerve during the dissection, requiring repair by microsurgical suture. In 1 case, it was not possible to locate the lithiasis during surgery, opting for an expectant attitude in the absence of symptoms. The rest of the data and complications are described in detail in Table 1.
Demographic Data, Complications, and Functional Results.
Discussion
The development of specific material and the accumulated experience make glandular resection techniques reserved, as a first therapeutic option, exclusively for the tumor pathology. Lithiasis, stenosis, and chronic inflammatory conditions can benefit from minimally invasive procedures associated with sialoendoscopy. This technique has demonstrated a diagnostic utility superior to radiology, locating pathology in the ductal tree, and allows us to treat directly through the optic work channels or combined transoral or transfacial approaches. 7,8 At the same time, the introduction of sialoendoscopy has meant a change in the surgeon’s vision on the treatment pathway and the interest in the application of minimally invasive techniques has been enhanced; recovering approaches described many years ago.
In 1953, Seldin et al 5 published his experience using transoral approaches to extract lithiasis in the submaxillary gland. Despite the good results shown in their work, in the last 60 years, glandular resection has been the norm and, in most countries, minimally invasive approaches whose efficacy has been proven recently by more authors have not been taken into account. 1,9,10
When we start the application of minimally invasive approaches, we compared our results with those obtained by SGR and detected similar rates in clinical resolution and complications with a significant reduction in hospitalization time. 6 On this occasion, we found that these good results have been maintained by increasing the number of cases operated.
The anatomical complexity in the hilum of the submaxillary gland is low; the lingual nerve is situated superiorly and medially to the gland in its posterior zone. In its anterior course runs lateral to the Wharton and crossing it medially at the height of the second molar (Figure 2). In many cases, we are faced with large stones that are easily palpable so the stone itself will mark the path of dissection, but the previous location of the lingual nerve is required to avoid the risk of injury. We can find small branches of the facial artery that we can control with bipolar coagulation, and the lingual artery and vein will usually be separated from the dissection area by the fibers of the hyoglossus muscle. The hypoglossal nerve will be less accessible when it appears in this approach in a deep position concerning the lingual nerve. However, maintaining a stable space between the displaced tongue and the jaw during the dissection can be difficult—being the assistant collaboration crucial in this procedure.
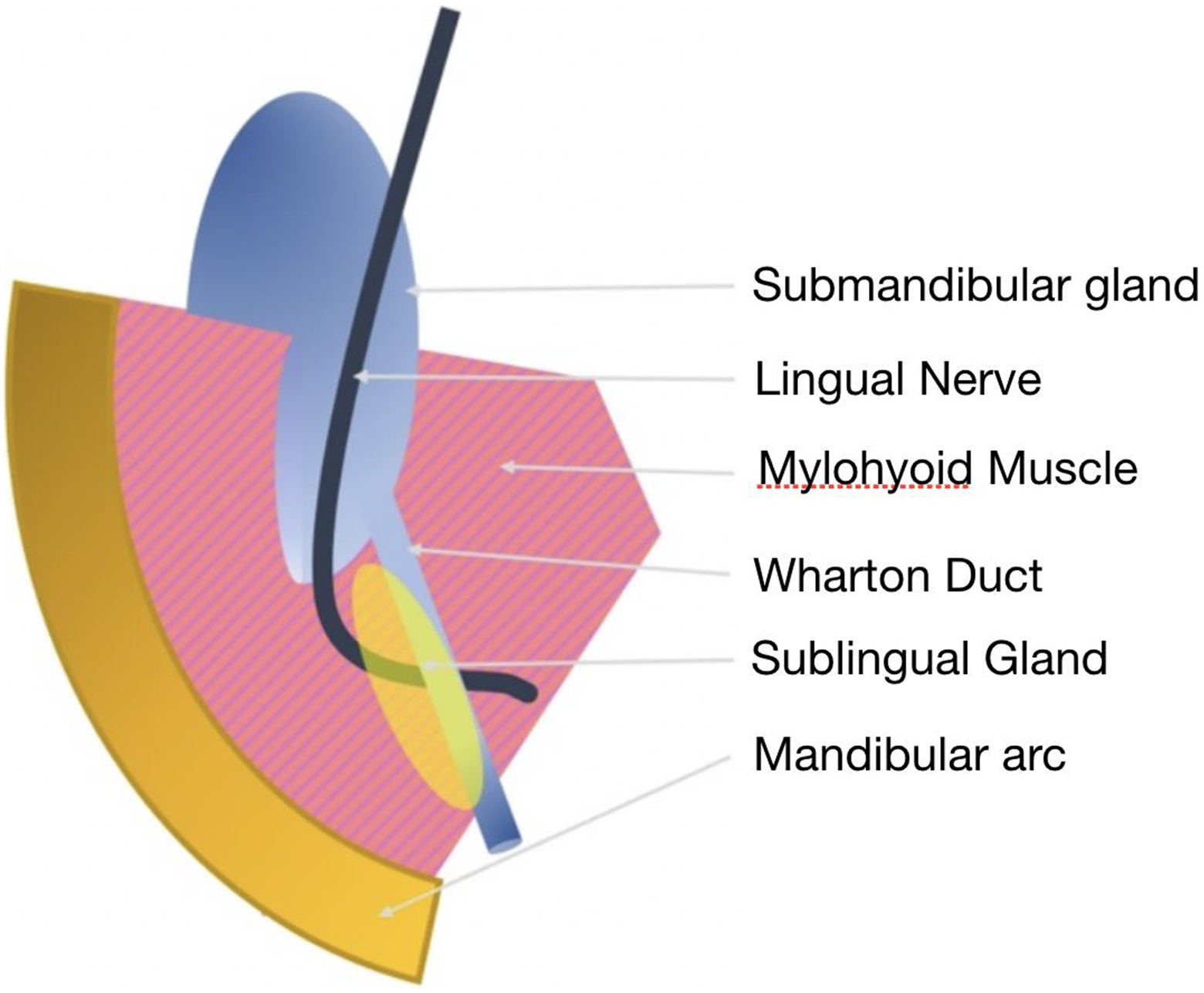
Schematic representation of the hilum gland.
The nerve manipulation, necessary in some cases, can be associated with an abnormal lingual sensitivity or hypoesthesia. Postsurgical pain, even in deep dissections, can be easily controlled with commonly used analgesics.
Transoral approach complications are less frequent and less severe than in SGR. Authors such as Combes review their complication rates and face those published in glandular resection, showing lower rates in transoral techniques. 9 Regarding intraoperative complications, these are related to the limited access rather than the anatomical complexities of the dissection. In our series, the most significant complication occurred as a result of poor control of the separation system that directly injured the lingual nerve. The development of specific retractor that allow us stable and atraumatic access to the hilum will be able to reduce the complication rate, which is already low. Some authors have already proposed devices that favor approach. 11
Our results and the data from other groups demonstrate the advantages of the transoral approach, providing an apparent advantage over glandular resection. For the patient, the postoperative period is more tolerable, and they can come back to regular activity in a shorter period, being the postoperative pain easy to control. We also conserve the submandibular gland whose functional and anatomical recovery after the period of obstruction has been demonstrated by multiple works. 12 –14 Some surgeons use recurrence rates as an argument to rule out these techniques. However, the recurrence rates detected in different studies rule out the systematic reappearance of the pathology. 1,5,10 Finally, we avoid the aesthetic alteration of the scars and the volume defect derived from the external approach.
Obviating the clear advantages for the patient, the transoral sialolitectomy also implies significant cost reductions comparing an outpatient surgery with a procedure with almost 2 to 3 days of hospital admission; this reduction is undeniable if we refer to a simple transoral approach without sialoendoscopy in the case of palpable and unique lithiasis. Moreover, this can be considered an effective option in those centers where the material necessary for a combined technique is not available. 15
Although several publications show a large series of patients treated by this technique under local anaesthesia, 1 we consider that general anesthesia can facilitate the procedure, especially in the first cases. Being the approach under local anesthesia, an excellent option for those patients with anesthetic contraindication as long as the anatomy is favorable.
In our current experience, there are no recurrence or tissue injury data that justify the sacrifice of the glandular parenchyma as a way to resolve the obstructive pathology in lithiasis sialadenitis. The transoral approach has been sufficiently proven and defined during the last decades to be universally accepted as the first option in the treatment of submaxillary sialolithiasis. Our experience in the first 33 cases treated with this technique has allowed us to restrict SGR, as the first choice, exclusively for cases of submaxillary tumor pathology. The accumulated knowledge about transoral approaches with and without sialoendoscopy indicates reductions in the time of admission, complications, and costs concerning the classic SGR.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.