
Abstract
Head and Neck Clinic
A 50-year-old man visited the emergency department of our hospital with a neck injury. The blade of a grass cutter suddenly dislodged on impact and penetrated his neck. Piercing pain and mild neck discomfort followed, but there was no massive bleeding or respiratory distress. Upon physical examination, a 7-mm-sized linear skin laceration was noted at the left upper lateral neck on the anterior border of the sternocleidomastoid (SCM) muscle. The foreign body was not visible but vaguely palpable under the skin.
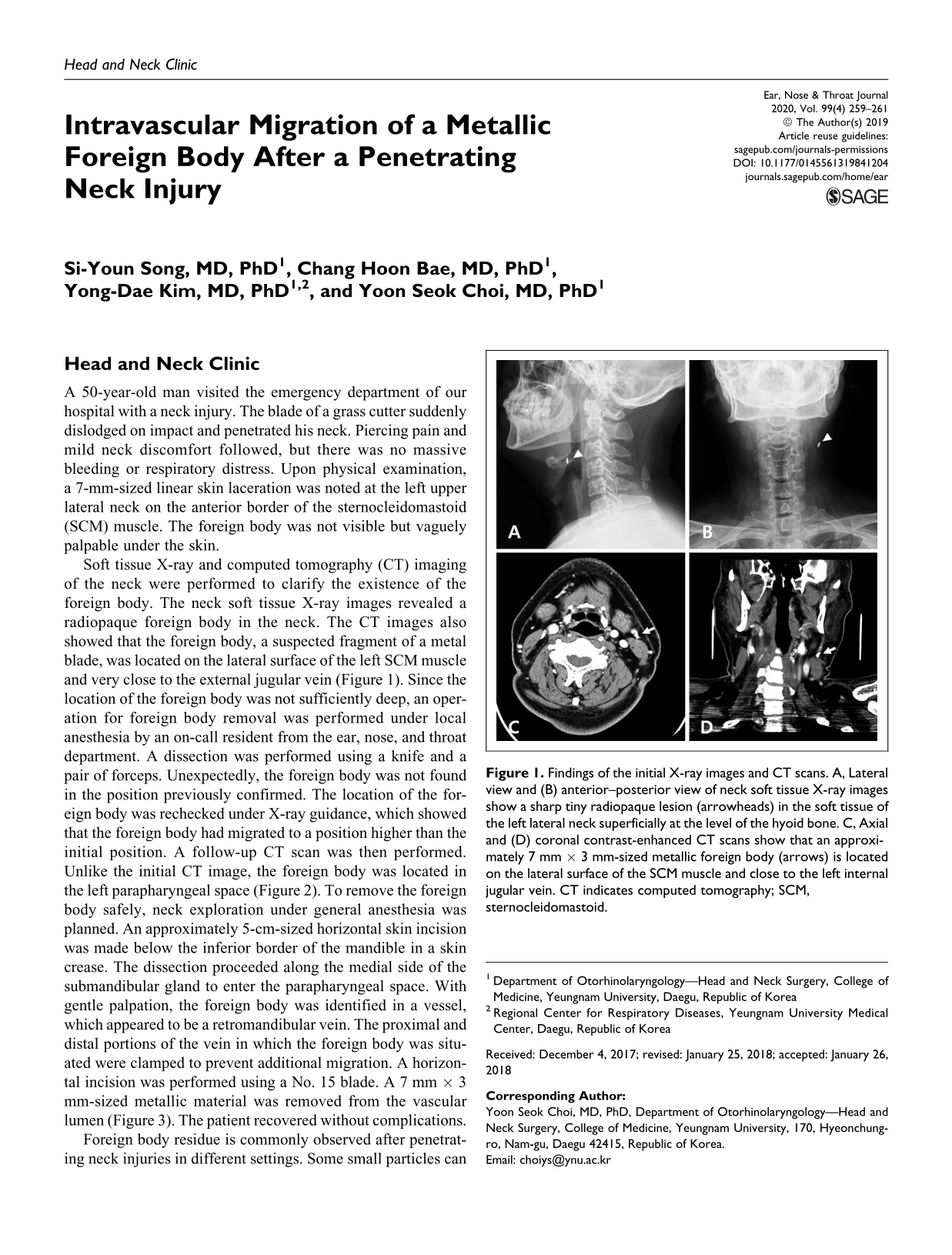
Soft tissue X-ray and computed tomography (CT) imaging of the neck were performed to clarify the existence of the foreign body. The neck soft tissue X-ray images revealed a radiopaque foreign body in the neck. The CT images also showed that the foreign body, a suspected fragment of a metal blade, was located on the lateral surface of the left SCM muscle and very close to the external jugular vein (Figure 1). Since the location of the foreign body was not sufficiently deep, an operation for foreign body removal was performed under local anesthesia by an on-call resident from the ear, nose, and throat department. A dissection was performed using a knife and a pair of forceps. Unexpectedly, the foreign body was not found in the position previously confirmed. The location of the foreign body was rechecked under X-ray guidance, which showed that the foreign body had migrated to a position higher than the initial position. A follow-up CT scan was then performed. Unlike the initial CT image, the foreign body was located in the left parapharyngeal space (Figure 2). To remove the foreign body safely, neck exploration under general anesthesia was planned. An approximately 5-cm-sized horizontal skin incision was made below the inferior border of the mandible in a skin crease. The dissection proceeded along the medial side of the submandibular gland to enter the parapharyngeal space. With gentle palpation, the foreign body was identified in a vessel, which appeared to be a retromandibular vein. The proximal and distal portions of the vein in which the foreign body was situated were clamped to prevent additional migration. A horizontal incision was performed using a No. 15 blade. A 7 mm × 3 mm-sized metallic material was removed from the vascular lumen (Figure 3). The patient recovered without complications.
Findings of the initial X-ray images and CT scans. A, Lateral view and (B) anterior–posterior view of neck soft tissue X-ray images show a sharp tiny radiopaque lesion (arrowheads) in the soft tissue of the left lateral neck superficially at the level of the hyoid bone. C, Axial and (D) coronal contrast-enhanced CT scans show that an approximately 7 mm × 3 mm-sized metallic foreign body (arrows) is located on the lateral surface of the SCM muscle and close to the left internal jugular vein. CT indicates computed tomography; SCM, sternocleidomastoid.
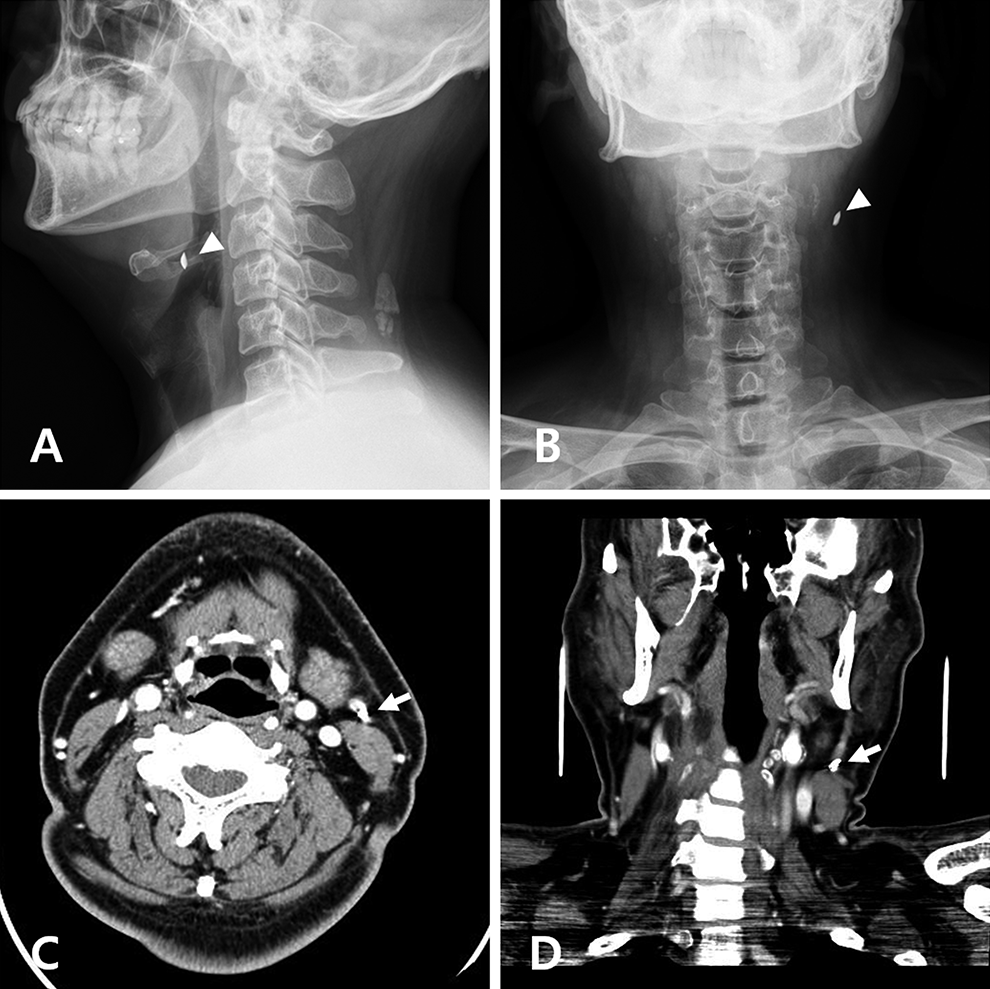
Findings of the follow-up X-ray images and CT scans after the first attempt for foreign body removal. A, Lateral view and (B) anterior–posterior view of the neck soft tissue X-ray images show that the metallic foreign body (arrowheads) had moved to a higher and deeper position than its initial position. C, Axial and (D) coronal contrast-enhanced CT scans revealed the metallic foreign body (arrows) in the left parapharyngeal space. CT indicates computed tomography.
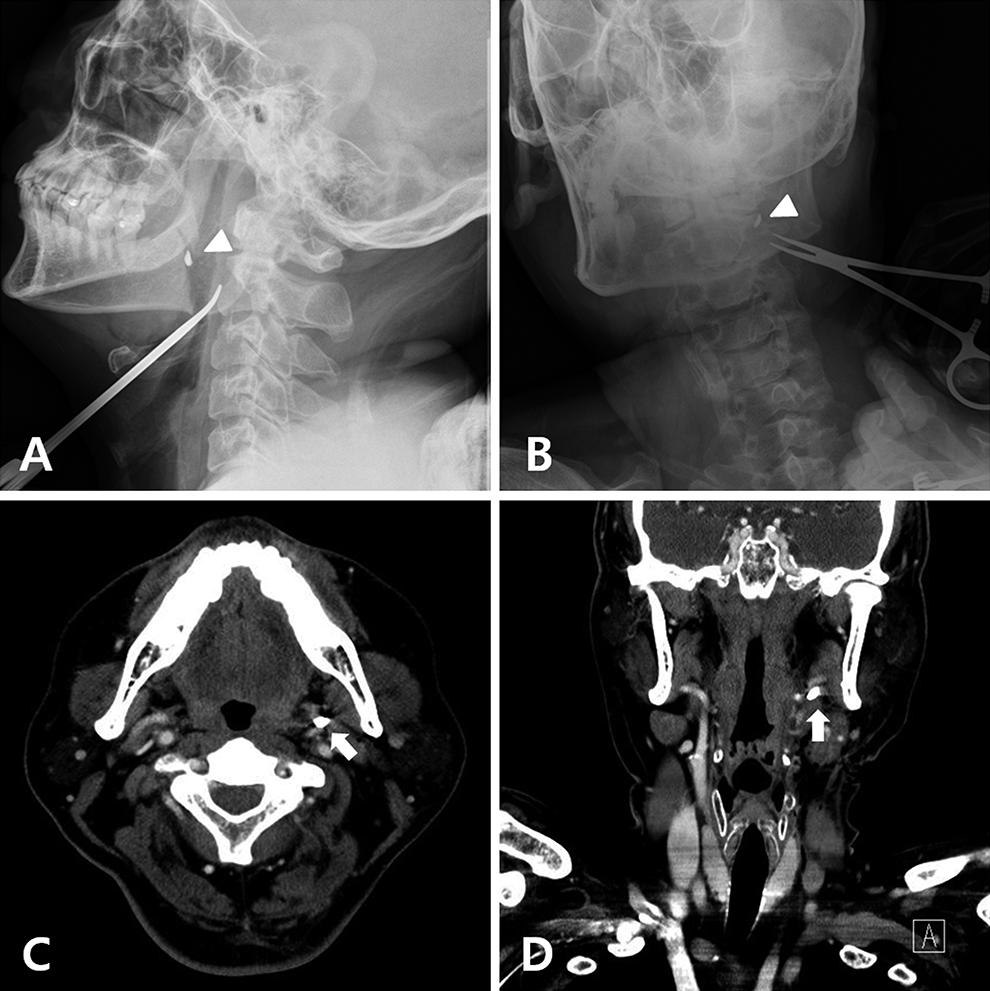
Intraoperative findings. A, Proximal and distal portion of the retromandibular vein (arrowheads) in which the foreign body was situated were tied to prevent additional migration and (B) the metallic foreign body (arrow) was observed in the lumen of the retromandibular vein.
Foreign body residue is commonly observed after penetrating neck injuries in different settings. Some small particles can be difficult to locate and remove. They can also penetrate the vascular wall or migrate through the vascular lumen, which cause false aneurysms that can result in delayed rupture. 1 In addition, an intravascular foreign body can migrate further and reach other organs, such as the brain or heart. 2,3 Without early diagnosis and treatment, residual foreign bodies remain a major cause of mortality.
Intravascular foreign bodies have been reported under the names of bullet emboli or missile emboli, which were widely known during World War II and the Vietnam war. 4,5 Rich et al reported 22 cases of 7500 casualties. 5 The incidence was approximately 0.3% and the majority were involved in the arterial system. Venous emboli are generally cited as being more uncommon. 6 In particular, peripheral venous migration limited to the neck is extremely rare; there are no reports in the literature.
The primary factors that determine the probability of intravascular foreign bodies are reported to be vessel proximity, kinetic energy, and size of the foreign body. 7 To enable a foreign body to penetrate the vessel wall, a shrapnel that is small in size with a low velocity is necessary. 8 Another important factor of migration is the size of the vessel and blood pressure. This is because in the case of an intravascular foreign body involved in a major vessel, the vessel diameter is large and the blood pressure is sufficiently high to form distant emboli. Therefore, it is less likely that a foreign body in a major vessel will be found near the original penetrating location. Moreover, in the case of superficial venous penetration, intravascular foreign body migration is unlikely because of the small diameter and low blood pressure.
In the present case, the metallic foreign body was observed to be adjacent to the external jugular vein on the CT image, but the initial exploration was performed without a thorough interpretation of the CT scan. Thereafter, the foreign body migrated to the peripheral vein against the bloodstream after the initial procedure. Consequently, an additional incision and dissection were needed and the foreign body was removed under general anesthesia. Although it is unclear whether the intravascular migration was iatrogenic or not, it appeared that the initial unsophisticated manipulation played a role to some degree. Through experience with this case, we now know that there is a risk of vascular wall penetration and intravascular migration of foreign bodies by unsophisticated procedures for removal near vessels and that detailed interpretation of CT findings is necessary prior to surgical removal of foreign bodies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the 2015 Yeungnam University Research Grant.