
Abstract
The maxillary bone’s frontal process, lacrimal bone, and ethmoidal labyrinth’s uncinate process can each harbor pneumatizations, referred to as agger nasi cells (ANCs), lacrimal cells (LCs), and uncinate bullae (UBs), respectively. Different studies have failed to differentiate ANCs from LCs. We aimed at studying these 3 anatomic sites to establish the anatomical patterns that could be encountered. We performed a retrospective study on cone-beam computed tomography scans of 36 patients (72 sides); the anatomic identification was supported by bidimensional multiplanar reconstructions (MPRs) in all 3 planes and 3-dimensional volume renderings. We established 6 patterns of pneumatization as follows: (1) type I: single LCs (47%), (2) type II: distinctive adjacent LCs and ANCs (8%), (3) type III: LCs expanded as UBs (6%), (4) type IV: ANCs adjacent to LCs expanded with UBs (1%), (5) type V: ANCs expanded as LCs (27%), and (6) type VI: ANCs expanded as LCs and further expanded as UBs (11%). In a type I pattern case, we found a cell-in-cell aspect on sagittal MPRs, which was further demonstrated as being an anterolateral recess of the middle nasal meatus projected in front of an LC. Such an “agger nasi recess” of the middle meatus was not previously described. For an accurate anatomical diagnosis, computed tomography studies should use complementary MPRs in all anatomical planes, as well as 3-dimensional models, to avoid confusing ANCs with LCs and better document the drainage pathways.
Introduction
Due to the advent of endoscopic surgery, an important role has emerged for diagnostic and preoperative computed tomography (CT) evaluation of the sinonasal anatomy; although anatomic variants are not disease states per se, they alter the normal drainage and access pathways. 1 The ethmoid sinus is considered the keystone of the sinus system, as it is related to the drainage pathways of all other paranasal sinuses; however, like all other sinuses, it can also be subject to great morphological variations. 2 Well-known anatomic variants could combine and generate less expected ones. 3
Agger nasi cells (ANCs) are usually regarded as anterior ethmoid cells. 4 However, although ANCs are considered present in all cases, 4 it has been adequately documented that this term is assigned to different anatomical structures, such as lacrimal cells (LCs), frontal sinus cells, and the recessus terminalis. 2 A true ANC is located in the agger nasi, a ridge anterior to the middle turbinate attachment on the nasal surface of the maxillary bone’s frontal process. 2 An LC corresponds laterally to the lacrimal bone and lies posterior to the agger nasi. 2,5 The recessus terminalis is determined by the superior insertion of the uncinate process on the medial orbital wall, and the separation of this recessus terminalis from ANCs is arbitrary. 6 Thus, we assume that ANCs are not a constant anatomical feature, and the aim of our research is to perform a retrospective cone-beam computed tomography (CBCT) study of the anatomic possibilities of pneumatization in the anterior part of the lateral nasal wall.
Material and Method
A retrospective CBCT study on the archived files of 36 patients (14 males and 22 females) was performed. All participants had been scanned using an iCat CBCT machine (Imaging Sciences International [Hatfield, PA, USA]) with the following settings: resolution 0.250, field of view 130, and image matrix size 640 × 640. The patients were positioned according to the manufacturer’s instructions. By using the iCatVision software, the CBCT data were exported as a single uncompressed DICOM file, which we further analyzed using the Planmeca Romexis Viewer 3.5.0.R software. We evaluated the bidimensional multiplanar reconstructions (MPRs) in the 3 anatomical planes, as well as the 3-dimensional volume renderizations of specified areas by use of the soft tissue filter. Relevant anatomical features were exported as image files. The patients have given written informed consent for all medical data (including radiographs, CBCT scans, and intraoral images) to be used for research and teaching purposes, provided the protection of the identity is maintained.
We considered ANCs those air cells located within the frontal process of the maxillary bone, in front and/or above the anterior end of the middle turbinate. We considered LCs those air cells that pneumatized the lacrimal bone but not the frontal process of the maxillary bone, being thus superior to the anterior end of the middle turbinate. We considered an uncinate bulla (UB) the air space extension within the uncinate process, as demonstrated on sagittal and coronal MPRs.
Single or adjacent air cells with distinctive drainage (ANCs and LCs) were documented, as well as possible combined variations resulting from expanded air cells: (1) LCs expanded as UB; (2) ANCs expanded as LCs; and (3) ANCs expanded as LCs, which were further expanded with UB.
Results
From the total of 72 sides that were evaluated using CBCT, several anatomical patterns of pneumatization of the lateral nasal wall above the anterior end of the middle turbinate emerged (Figure 1). We did not find ANCs without adjacent LCs.
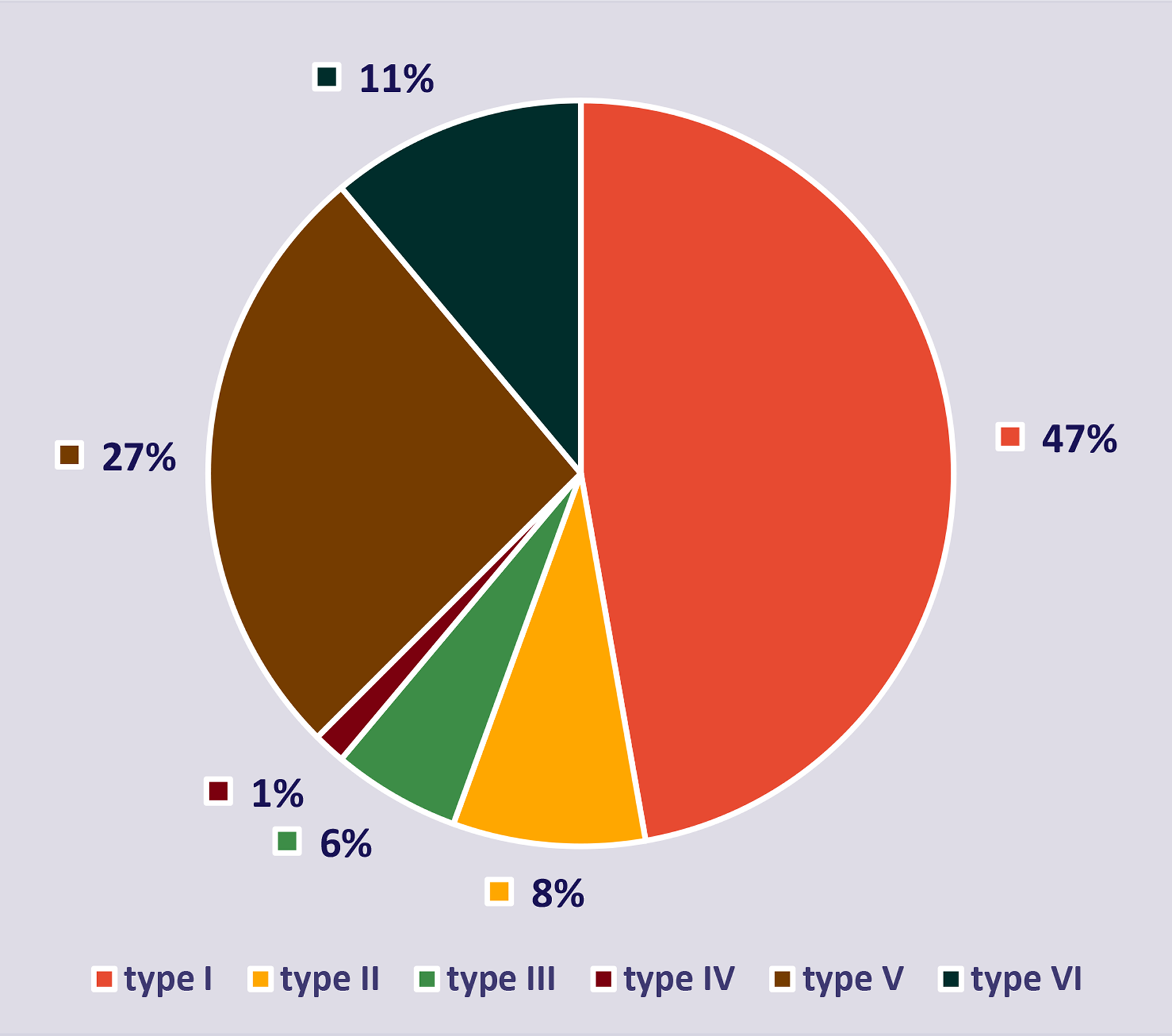
Prevalence of different anatomical patterns (I-VI) at the level of the agger nasi cell. N = 72 sides.
In 6 cases (type I), we found unilateral (6 sides) LCs not neighbored by ANCs; these did not expand beyond the limits of the lacrimal bone. On the opposite sides, we found the following: (1) type V pneumatization in 5 cases, with the ANCs expanded posteriorly as LCs; and (2) type III (LC expanded in the UP as UB) pneumatization in 1 case. In another 14 cases, type I was found bilaterally (28 sides). The LCs in type I were draining either into the frontal recess (FR; 2/34 sides) or ethmoidal infundibulum (EI; 32/34 sides).
For type II, with adjacent ANCs and LCs (6 cases; Figure 2), the ANCs were draining into the FR (3 cases), MNM (2 cases), and EI (1 case). In type III, LCs expanded with UBs (Figure 3) were found unilaterally in 4 cases (4 sides), all draining into the EI. For type IV (one case/side), an ANC was adjacent to an LC expanded with UB.
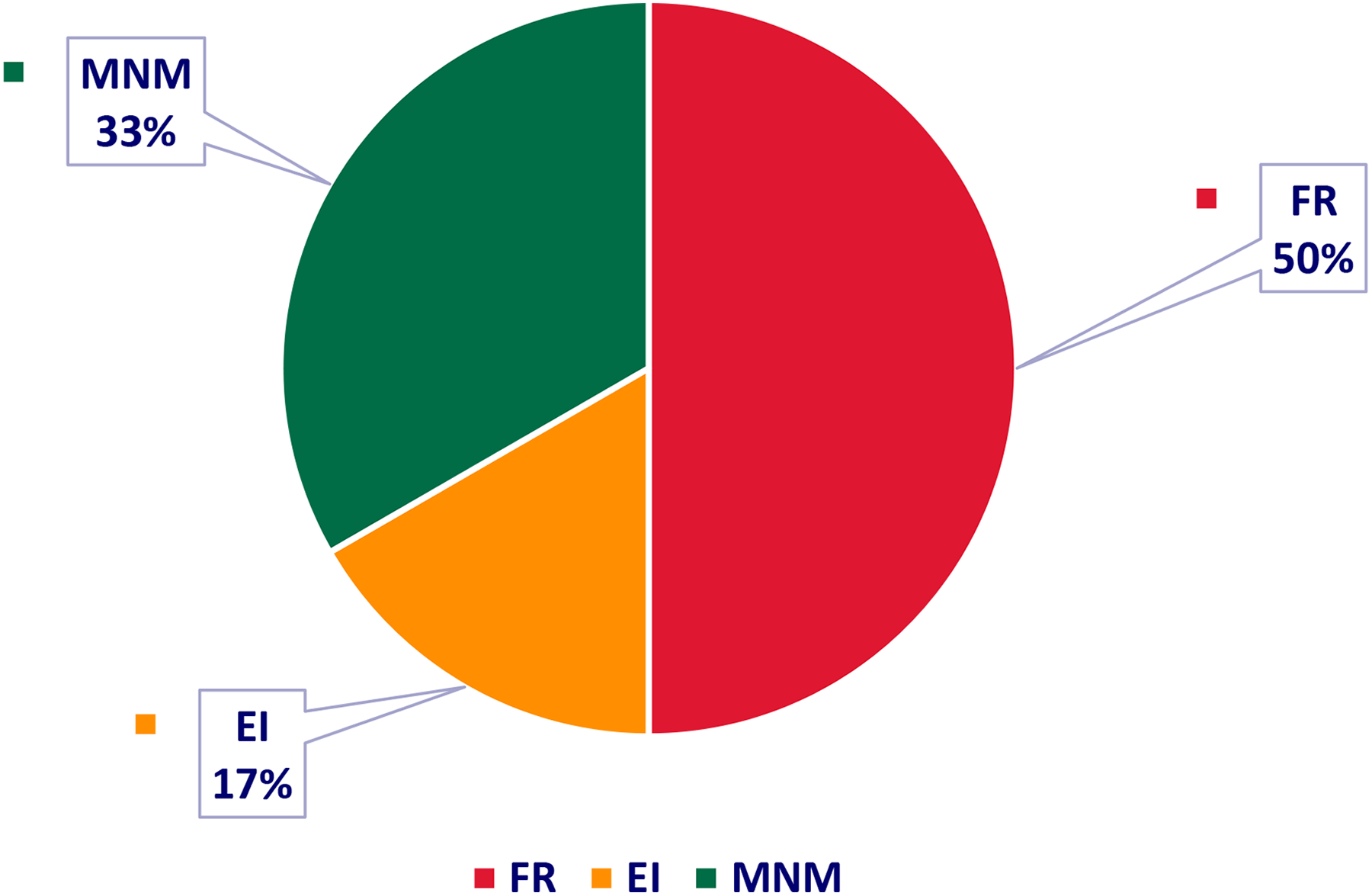
Drainage of ANCs associated with LCs (type II). ANC indicates agger nasi cell; EI, ethmoidal infundibulum; FR, frontal recess; LC, lacrimal cell; MNM, middle nasal meatus.
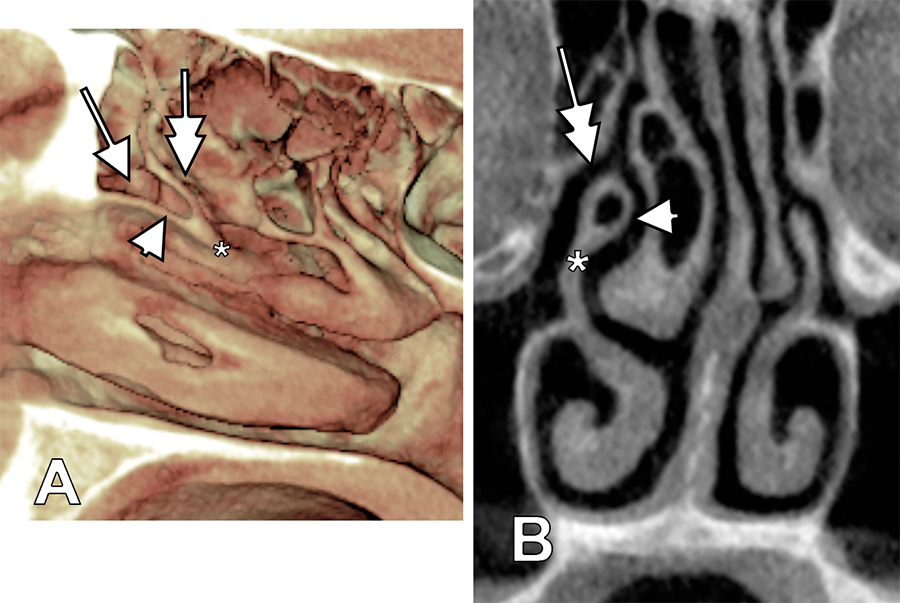
Three-dimensional volume renderization (A, medial view of right lateral nasal wall) and coronal MPR (B) depicting the coalescence of an LC (arrow) with an UB (arrowhead). These are indicated the UP (*) and the EI (double-headed arrow). EI indicates ethmoidal infundibulum; LC, lacrimal cell; MPR, multiplanar reconstruction; UB, uncinate bulla.
In type V, ANCs were found to be expanded posteriorly as LCs in 19 of 72 sides. In 7 cases, these were unilateral (7 sides), with the following patterns found on the opposite sides: (1) type I (5 cases), (2) type II (1 case), and (3) type VI (1 case). In 6 cases, type V was bilateral (12 sides).
Agger nasi cells expanded as LCs (or vice versa) were well differentiated on axial MPRs. We could identify ANCs located in the maxillary bone’s frontal process and LCs in the lacrimal bone (Figure 4).

Axial MPR depicting coalescence of ANC and LC on the right side (diverging arrows) and LC on the opposite side (arrowhead). ANC indicates agger nasi cell; LC, lacrimal cell; MPR, multiplanar reconstruction.
The last type (VI), in which ANCs were expanded posteriorly as LCs and then with UBs, was found in 7 cases. Six cases were unilateral (6 sides), while in one case, the pattern was bilateral (2 sides; Figure 5).
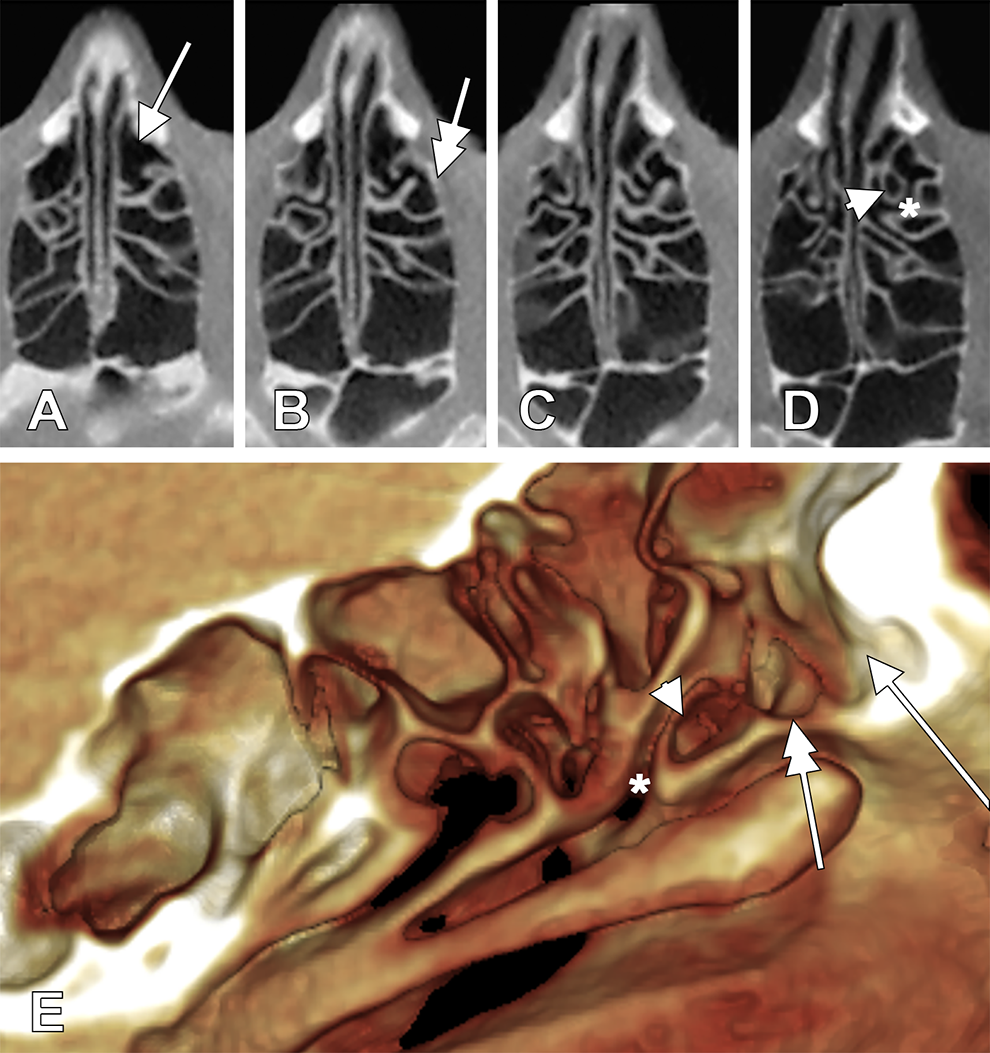
Triple coalescence of ANC (arrow), LC (double-headed arrow), and UB (arrowhead) is documented on serial axial MPRs (A-D, superior-to-inferior sequence) and on three-dimensional volume renderization (E, medial view of left lateral nasal wall). *EI. ANC indicates agger nasi cell; EI, ethmoidal infundibulum; LC, lacrimal cell; MPR, multiplanar reconstruction; UB, uncinate bulla.
In a case with bilateral asymmetry, on the right side (Figures 6 and 7), we found an ANC draining into the FR; this, in turn, was located above the LC on that side, thereby representing a type II pattern. On the opposite side, we found an LC without an ANC; thus, it was a type I pattern. Here, the left LC was found to have a cell-in-cell feature on sagittal MPRs (Figure 7A), as determined by a small rounded air space embedded immediately behind the anterior wall of the LC. However, as further identification proceeded, it became clear that the small air cell–like space was in fact a narrow anterolateral recess of the MNM (Figures 6 and 7), which was in contact with the frontal process of the maxillary bone in the agger nasi site; thus, it was projected beneath the fossa of the lacrimal sac. We termed this MNM recess an “agger nasi recess.”
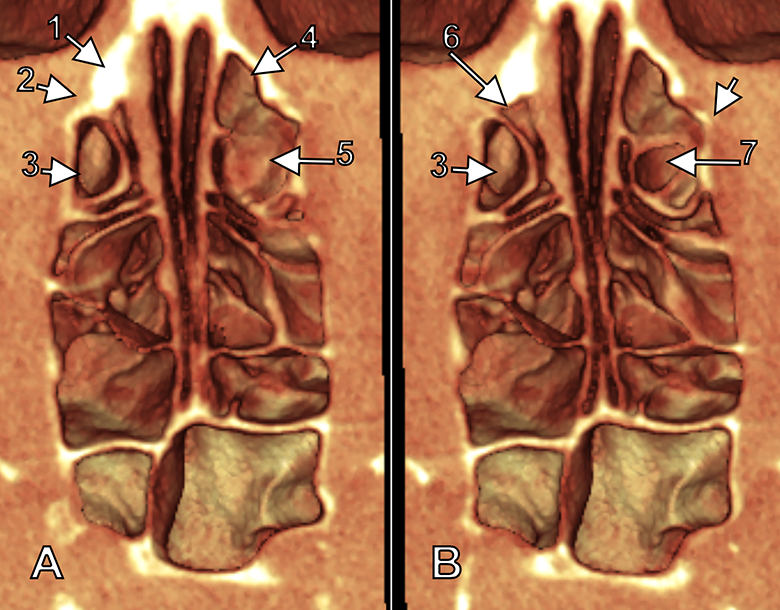
Three-dimensional volume renderization, superior views of successive axial cuts (A: superior, B: inferior) of nasal fossae: (1) frontal process of left maxillary bone, (2) left fossa for lacrimal sac, (3) left LC, (4) right ANC, (5) FR, (6) anterolateral recess (agger nasi recess) of left MNM, (7) right LC, and (8) right posterior lacrimal crest. ANC indicates agger nasi cell; LC, lacrimal cell.
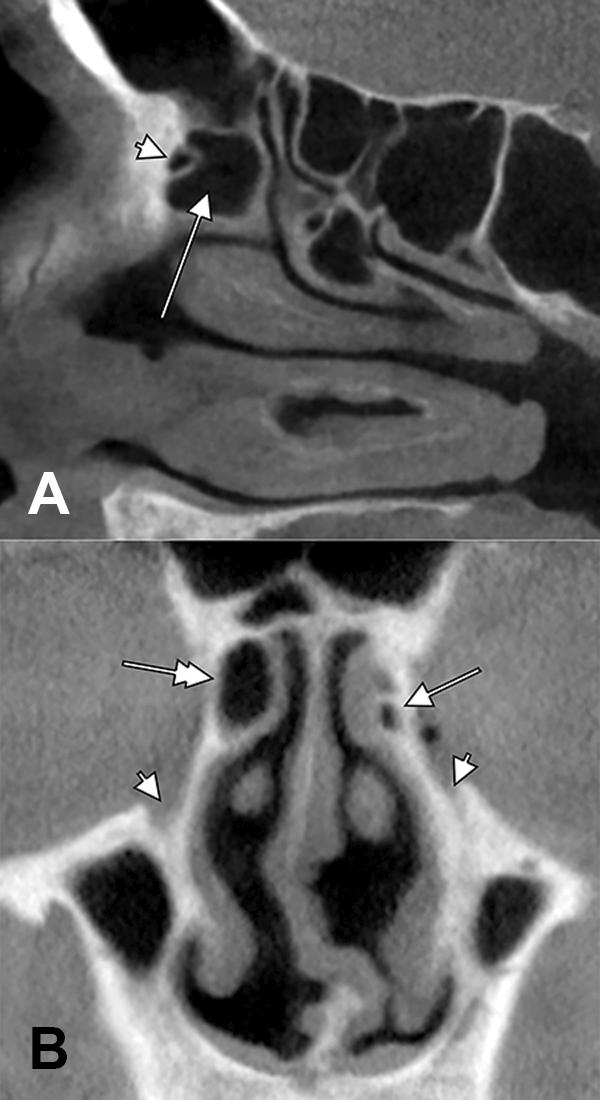
A, Sagittal MPR. The agger nasi recess of left MNM appears as a false air cell (arrowhead) within the LC (arrow). B, Coronal MPR. The topography of the right ANC (double-headed arrow) and of the agger nasi recess of the left MNM is comparable as related to the nasolacrimal canals (arrowheads). ANC indicates agger nasi cell; MPR, multiplanar reconstruction; LC, lacrimal cell.
Discussion
Morphogenesis of ANCs
During fetal development, in the lateral nasal wall, ridges or folds called ethmoturbinals form, and these have ascending anterior and descending posteroinferior portions. 7 The ascending portion of the first ethmoturbinal remains as the agger nasi. 7 Bone pneumatization at the agger nasi ridge is an ANC.
True/False ANCs and Overlooked LCs
A true ANC was rigorously differentiated from an LC as follows: the lateral wall of an ANC is the maxilla’s frontal process, whereas the lateral wall of an LC is composed of the lacrimal bone. 2 On coronal slices, the anterior border of the middle nasal turbinate is not observed adjacent to an ANC, but it is evident if an LC is cut. 2 We used these landmarks in our study, and we found that true ANCs were absent, but they could be imitated by LCs (types I and III), in 53% of cases. When anatomical diagnoses are performed on CT slices, it should not simply be assumed that “the most anterior air cell in the lateral nasal wall is the ANC” 7,8 ; rather, the middle turbinate and lacrimal and maxillary bones should be observed to determine whether the air space is an ANC or just an LC. An air cell above the anterior end of the middle turbinate on coronal CT is not an ANC, as some authors have indicated, 8 but an LC.
Agger nasi cells have been defined as those air cells lying anterior to the upper end of the nasolacrimal duct. 1 When this landmark is used, it should be kept in mind that LCs are posterior to the upper end of the nasolacrimal duct, which suggests that the anatomical evaluation should be conducted using a series of coronal slices, and not just a single one.
We documented several studies dealing with ANCs by searching for the term “lacrimal”; when this term was found, we checked further to determine whether it indicated LCs (Table 1). The results showed that, although ANCs were documented, LCs were not distinguished from ANCs. When LCs are considered a distinctive anatomic structure, as in our study, one can observe that the prevalence of ANCs decreases (Table 1). When the ANC was adequately located anterior to the anterior end of the middle turbinate, it was identified in 49% of cases, 15 which is comparable to our results. However, a study in which it was adequately observed that ANCs could invade the lacrimal bone found a very low prevalence of ANCs compared with other authors’ results, at only 1.9%. 17
Different Studies Failed to Discriminate Between Agger Nasi Cells (ANCs) and Lacrimal Cells (LCs), Which Could Explain Why in the Present Study the Prevalence of ANCs Is Lower.
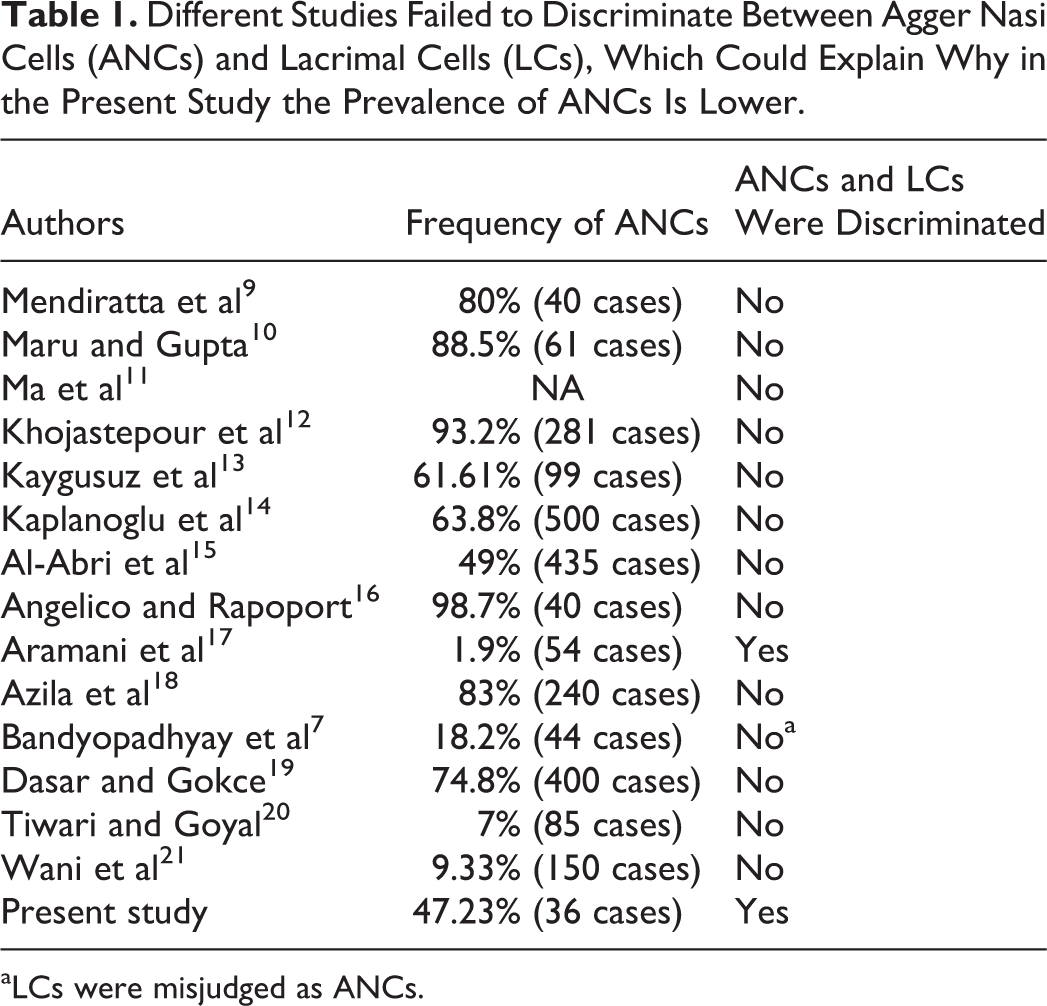
aLCs were misjudged as ANCs.
A frequency of 18.2% for ANCs was reported in one study, but these were identified as “the most anterior ethmoidal cell, situated below the frontal sinus, next to the frontal recess, representing the lacrimal bone pneumatization due to ethmoidal extension.” 7 This definition undoubtedly indicates LCs and not ANCs.
It was previously discussed that the FR above the ANC could obstruct the drainage pathway of the frontal sinus. 10 We demonstrated that this is also true for LCs, especially if an ANC is absent.
Endoscopic sinus surgery is increasingly used to reestablish sinus drainage and ventilation. Although conventional endoscopic frontal sinus surgery can alleviate most chronic frontal sinusitis, peculiar anatomic patterns challenge the endoscopic intranasal approach. 11 The Draf procedures and endoscopic modified Lothrop procedure are challenging techniques that are useful for the management of difficult frontal sinus diseases. 11 A modified endoscopic frontal sinus surgical approach was proposed that uses the agger nasi landmark to approach the frontal sinus floor by drilling the frontal process of the maxillary bone (termed the “frontomaxillary process”). 11 The prevalence of ANCs in the 85 patients included in the study was not presented 11 nor was a discussion provided of how the substitution of an ANC with an LC could impede the modified endoscopic procedure. Rather, it was reported that the “frontomaxillary process was directly drilled out upward between the orbital plate of the ethmoid bone and attachment of middle turbinate.” 11 This overlooks the lacrimal bone intercalated between the frontal process and ethmoidal labyrinth.
Endoscopy is used for both nasal and sinus surgery and dacryocystorhinostomy (DCR). 22 In endoscopic endonasal DCR surgery, the UPs and/or ANCs were frequently found to obstruct the access to the lacrimal fossa. 23 Our analysis demonstrates that an LC and/or UB could do the same. The DCR failure was attributed to intranasal problems impeding the creation of a reliable connection between the lacrimal sac and nasal fossa. 22 Agger nasi cells close to the lacrimal sac should be removed during DCR surgery. 22 During the procedure, it is possible to injure not only the frontal and ethmoidal sinuses 22 but also the LCs, as shown here; such injury could lead to postsurgical adhesions. Nevertheless, a surgical solution for a diseased ANC that ignores an adjacent LC could leave on site a possible subsequent cause of nasolacrimal duct obstruction.
The UB: A Rare Entity
The UP of the ethmoid bone belongs to the lateral wall of the MNM. Its pneumatization is known as an UB, which is a rare entity defined as an “an extension of air cells” in the UP. 24 As the UP limits the EI, if an UB is present, it narrows it and impairs the drainage and ventilation of the sinuses. The coexistence of UBs and maxillary sinusitis was found to be statistically significant. 25
Our evidence supports the claim that the only type of air cell that can expand into the UP is an LC; UB was found in the present study in 13 (18.05%) of 72 sides. In 750 patients (1500 sides) evaluated by CT, there were UBs found in 6.26% of cases; these were located unilaterally in 1.60% of the patients. 25 A different group found UBs in 5% of 512 cases (1024 sides). 24 Kennedy and Zinreich found UB in 1 (0.4%) of 230 patients, on coronal CTs. 26 Bolger et al also found UBs, which they described as an uncommon variation, in 2.5% of 202 patients, and they indicated that the pneumatization occurred in the most anterior–superior part of the UP because of “an excavation of the agger nasi cell” 27 ; however, this description is inexact. These latter authors documented only coronal CT scans of patients, which are less suitable for the adequate identification of the so-called ANC placement, especially when the structures are not explored in all 3 anatomical planes; these could have equally been air cells of the maxilla’s frontal process or the lacrimal bone. As we demonstrated, an ANC can expand as an UB only after joining an LC, with the lacrimal bone intercalated between the frontal process of the maxilla and the UP-projecting ethmoidal labyrinth. Cumberworth et al 28 found 1 unilateral and 2 bilateral UBs (1.2%) in 250 patients and quoted Bolger et al’s (1990) 27 claim that the UB is an extension of the ANC. Our comments above are supported by the study of Yenigun et al who found that the simultaneous occurrence of an UB and ANC has no statistical significance. 25 However, this latter study was also performed exclusively on coronal CTs, leading to the speculative assessment that the UB is either an extension of the medial wall of the maxillary sinus or something that originates from the medial face of the orbit and superior wall of the maxillary sinus.
The Agger Nasi Recess of the MNM
Previous reports have given evidence for the possibility for nasal meatuses sending lateral recesses toward the fossae neighboring the nasal fossa, such as pterygopalatine recesses of the middle and superior nasal meatuses. 29,30 We could not find any report indicating that the MNM could project a recess toward the fossa for the lacrimal sac; here, we report such an “agger nasi recess” of the MNM. Such a rare variation could facilitate, or modify, the DCR procedure by which the lacrimal sac is fistulized into the nasal fossa.
Concluding Remarks
Different patterns of pneumatization can occur above the anterior end of the middle turbinate, and these are not uniquely ANCs. For accurate diagnosis, it is mandatory for further CT studies evaluating pneumatizations of the lateral nasal wall to use complementary MPRs in all anatomical planes, as well as 3-dimensional models. Care should be taken to adequately locate ANCs to avoid distorting the studies’ prevalence results.
This study demonstrated that CBCT could be a more reliable tool for the evaluation of nasal pneumatizations, as previously assessed. 12,29,31 The need for CBCT prior to any surgical procedure should be determined on a case-by-case basis, as the common Vesalian anatomy is frequently overridden by anatomical variations. 32,33
Footnotes
Authors’ Note
All authors have equally contributed to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.