
Abstract
Introduction:
Virtual endoscopy (VE) is the computer-based reprocessing of diagnostic imaging to simulate endoscopy of an anatomic region of interest. VE of the Frontal Sinus Outflow Tract (FSOT) may assist surgical planning and education.
Method:
VE was performed on 16 normal sinus computed tomography (CT) scans for a total of 32 sides using the “path-to-target” tool on the TruDi surgical navigation system (ver. 2.3; Acclarent, Irving, CA, USA). To aid orientation during VE, planning points were placed on the middle turbinate, ethmoidal bulla, and skull base. The VE representation of anatomy and FSOT accuracy was manually confirmed by reviewing the corresponding orthogonal CT images and comparing them to the computed pathway.
Results:
Of the 32 sides, the software successfully calculated the FSOT in 22 sides (69%). Of those 22 sides, the calculated FSOT, depicted in the VE sequences accurately represented the FSOT. Among sides with an accurately calculated FSOT, the VE sequences depicted a “fly-through” from a starting point in the middle meatus around various frontal recess cells to the end point in the frontal sinus
Conclusion:
This pilot study demonstrates that software-generated VE of the FSOT is indeed feasible but requires confirmation by the surgeon for accuracy. Instances in which the software did not achieve its objective may drive further refinements of the protocol. VE of the FSOT should be explored as a tool for preoperative planning and surgical education.
Introduction
Virtual endoscopy (VE) is best described as a 3-dimensional viewing of hollow viscus structures based on high-resolution radiographic imaging studies created from computer-based algorithms. 1 This human-computer interface simulates realistic environments and enables surgeons to experience interactive 3D digital models. The early application of VE in paranasal sinus anatomy was demonstrated by Gilani et al. 2
VE replicates the natural environment with “freely flying” pathways through and around corners of 3-dimensional structures. In theory, VE offers unique advantages in navigating the complex pathway to the frontal recess. The utilization of VE as a planning tool could provide potential benefits in surgical planning, efficiency, and safety, especially in training environments. Previous applications of virtual endoscopy in the sinus anatomy involved manual translation of high-resolution computed tomography studies into virtual endoscopic view using various 3D reconstruction software applications. 3 Traditionally, this process was time-consuming, laborious, and impractical in a surgical environment driven by rapid turnovers and efficiency. The TruDi (ver2.3) navigation system (Acclarent, Irvine, CA) incorporates real-time semi-automated software rendering of a virtual fly-through path of the frontal sinus drainage outflow tract from high-resolution sinus computed tomography (CT) imaging data. This study illustrates the application of this software in the assessment of frontal recess anatomy.
Methods
All sinus CT scans with 0.5 mm contiguous axial slices from Jan 2022 to Oct 2022 from our rhinology patient directory portal were reviewed with chief main complaint being headache. We have excluded any CT scan images depicting pathology within the frontal recess, frontal sinus disease, unilateral or bilateral frontal sinus aplasia, fibro-osseous lesions in the frontoethmoidal region, previous maxillofacial trauma, congenital anomalies, or previous sinus surgery. Each scan was uploaded to TruDi version 2.3 (Acclarent Irving, CA, V2.3), and the path-to-target tool of the software was used to automatically calculate the path from the middle meatus entrance to the frontal sinus bilaterally and examined with VE. TruDi’s VE tool provides a prospective rendering of the anatomy along the calculated path. By advancing along the path, the user can visualize the anatomy through a virtually reconstructed 3D space as if one were moving a virtual telescopic camera along the path. To aid in orientation, the ethmoid bulla, middle turbinate, and skull base were marked with color-coded planning points using another TruDi planning tool. The VE representation of the frontal recess anatomy was manually confirmed by reviewing the corresponding orthogonal CT images and comparing it to the computed pathway.
The committee for the Protection of Human Subjects of The University of Texas Health Science at Houston approved this retrospective review.
Results
A total of 16 scans (32 sides) were reviewed on patients ranging from 25 to 80 years old with the median age of 50.5 years. For each case the virtual endoscopic video analysis and corresponding orthogonal CT scan were reviewed together.
The TruDi software was able to identify the FSOT in 22 sides (68.75%). The system was not able to generate a FSOT virtual path in the remaining 10 sides (31.25%). When each completed VE sequence was further analyzed, all 22 sides were deemed to represent the true FSOT (Figure 1). Amongst the 22 sides, 3 sides displayed artifacts where a pathway appeared to cross soft tissue or bone in the VE view. However, the pathway on the orthogonal CT images was correct (Figure 2). This occurs as a result of an offset between the virtual camera and the calculated pathway so that the virtual camera can visualize the pathway. In these instances, the calculated FSOT remained accurate on secondary review that included tracing the pathway on the orthogonal CT images. Among those 10 sides where no actual pathway was found, 6 out of 10 (60%) seemed to be anatomically complex cellular configurations in the frontal recess.
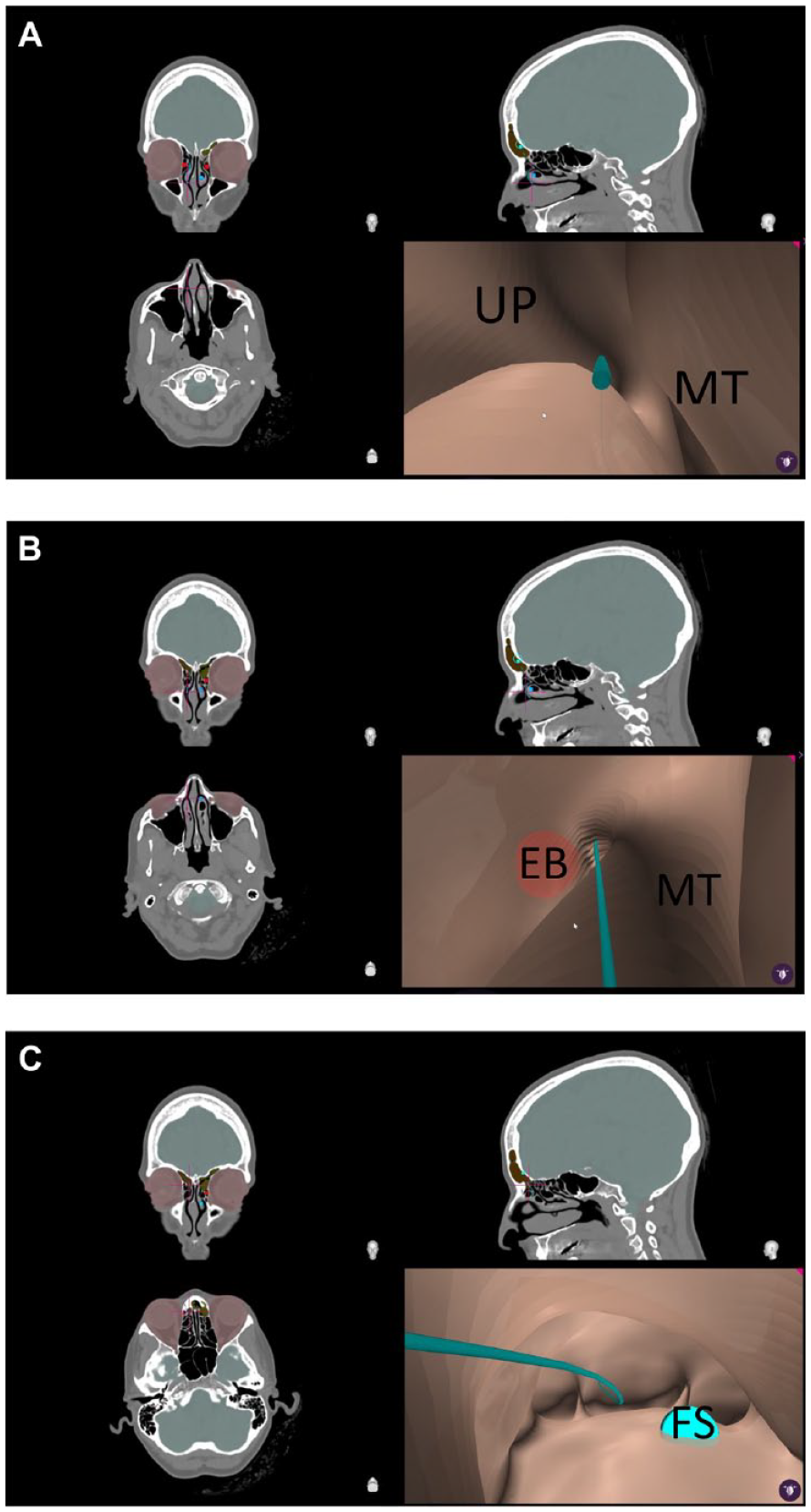
In this example showing the normal free-flying open FSOP pathway (blue line) in VE view from starting point at the middle meatus (A), through the frontal recess region (B), and into the frontal sinus (C).
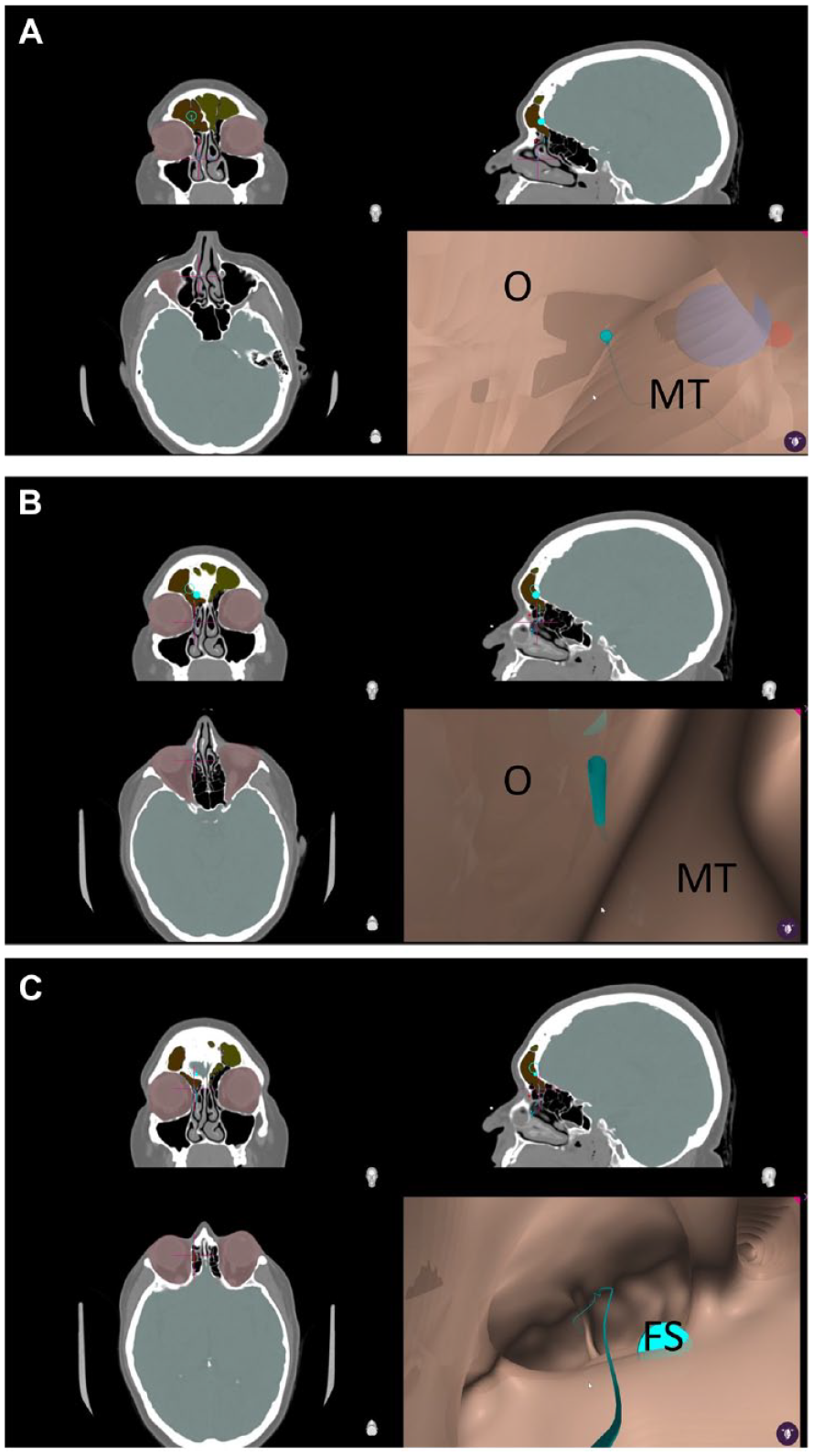
In this figure the initial virtual flying pathway shown in figure (A) subsequently appears to cross soft tissue or bone in the VE view. (B) Final virtual pathway below confirms the pathway in the open FSOP. (C) However, the pathway shown on the orthogonal CT images was correct and did not violate bony or soft tissue limits (A, B, C).
Discussion
The aim of our study was to assess the fidelity of VE video sequences of the frontal recess in patients without sinus disease. In theory, VE could be a tool for resident and fellow education. The current study highlights the output of an automated system for VE rendering.
The introduction of VE constructed from CT images has been previously described for use in hollow visceral structures such as virtual colonoscopy and bronchoscopy for diagnostic purposes.4,5 Such use was expanded to include sinus surgery in the late 1990’s, but the tedious and time-consuming nature of converting a sinus CT scan into virtual endoscopy halted further progress.2,6 The utilization of virtual endoscopy in the context of skull base surgeries involving sellar tumors has been described in this report. The Osirix application was used to convert DICOM files into VE views, thereby enabling pre-operative assessment of the relationship of the tumor, carotid artery, and pituitary gland.7,8 However, despite the pre-operative educational value, the intra-operative applicability was constrained in part because the system was non-interactive.7,8 More recently, TruDi version 2.3 (Acclarent, Irving, CA, USA), a navigation system platform used for sinus surgery, added an built-in functionality to automatically create a virtual endoscopy fly-through pathway from a DICOM file with an average processing time less than 1 minute.
In the current report, the TruDi software was able to successfully generate an FSOT with accuracy in 68% of sides. An automated system of identifying and generating paths is more efficient, but one should remember that the calculations can lead to inadvertent collision with surfaces, which create artefacts in the VE output. The TruDi software, however, was not able to generate any FSOT pathway in 32% of the sides. The technical parameters for calculating the Virtual Sinus Outflow Tract (VSOT) are not available for review; however, it is possible to speculate on possible causes. Certain anatomic details may be beyond the resolution of CT scan, and therefore, the gaps between image slices can serve as additional sources of error. Small areas of mucosal contact or tight bony confines may also render identification of the FSOT problematic.
VE is a potential non-invasive pre-operative surgical tool for both trainees and novice endoscopic sinus surgeons. The calculated VSOT pathway can be displayed on both the orthogonal CT images and a 3-dimensional rendering when the TruDi system is used for surgical navigation. VE during surgical navigation, which is beyond the scope of this paper, is worthy of exploration. Obviously, before clinical work, the fidelity of the VE sequences must be confirmed, as this project illustrates. Similarly, to other VE sequences, the VE images seem flat and lack details for the orientation of the viewer. To compensate for this limitation, the application of planning points using another software tool provided in TruDi software package, provide guideposts for orientation. It is crucial to note that virtual endoscopy is heavily reliant on the quality of CT images fed into navigation system, which could consequently result in views not accurately reflect the exact intricate anatomical pathway resulting in misinterpretation. The augmentation of the VE view by incorporating additional details such as frontal recess configuration (agger nasi cells and supra-agger cells) into frontal recess region and enhancing the texture along with color would prove advantageous in rendering a representation that closely resembles the real endoscopic view. Although not explored in this project, the integration of VE sequences with traditional surgical navigation for sinus surgery is worth exploration. It is imperative to acknowledge that despite the aforementioned shortcomings of virtual endoscopy, it remains a tool that necessitates a requisite learning curve for proficient utilization by surgeons.
Conclusion
Surgical dissection of the frontal recess can be a formidable challenge for the practicing rhinologist. We developed a pilot study demonstrating the use of in-built semi-automated feature on a navigation platform rendering virtual endoscopic views of the frontal recess as a potential pre-op planning tool. Our study indeed showed reasonable reliability of the system depicting frontal recess pathway; however, reconfirmation with triplanar sinus CT scan by the surgeon is required for accuracy. There is a great potential for future improvement with further refinement of the VE algorithms and planning tools, including the addition of color-coded points for orientation and additional annotations for relevant anatomy.
Footnotes
Acknowledgements
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The committee for the Protection of Human Subjects of The University of Texas Health Science at Houston approved this retrospective review.