
Abstract
Obesity in pediatric population is an important global problem. The prevalence of obesity in children is dramatically rising. According to World Health Organization, about 41 million children under the age of 5 years are obese or overweight worldwide. Overweight and obesity are well-known risk factors for a number of health disorders. Diseases commonly observed in this group of patients are metabolic disorders, type 2 diabetes mellitus, cardiovascular diseases, fatty liver disease, musculoskeletal problems, and many others. The main aim of this study was to present the current knowledge of the association between childhood obesity and common otorhinolaryngological disorders. It is suggested that obese children are more prone to suffer from otorhinolaryngological illnesses than the lean ones. Obesity may predispose to otorhinolaryngological diseases in various ways. It strongly interferes with the immune system (increases serum levels of interleukin 6, tumor necrosis factor, C-reactive protein, and leptin and reduces adiponectin concentration) affecting organs of the upper respiratory tract. Additionally, obesity induces mechanical disorders in the upper airways. According to our review, obesity predisposes to otitis media with effusion, acute otitis media, recurrent otitis media, obstructive sleep apnea, sensorineural hearing loss, adenotonsillar hypertrophy, and post-/perioperative complications after adenotonsillectomy. Obesity in children significantly correlates with both obstructive sleep apnea (OSA) and asthma and constitutes a significant component of “OSA, obesity, asthma” triad.
Introduction
Obesity in pediatric population is an important global problem. The prevalence of obesity in children is dramatically rising. According to the World Health Organization (WHO) about 41 million children under the age of 5 years are obese or overweight (OW) worldwide. It was estimated that in the United States that approximately 32% of children are OW or obese, and among them approximately 17% fulfill the criteria for obesity. In southern Europe, the prevalence reaches 40%. 1
Overweight/obesity is a status of excessive adipose tissue accumulated in the human body. The international measurement of body mass status is called body mass index (BMI). The BMI classifies individuals as underweight, normal weight, OW, or obese. The BMI measure can be used in both adults and children; however, the scoring differs in these 2 groups. In children, “OW” is defined as a BMI at or above 85th percentile and below the 95th percentile adjusted for sex and age, whereas “obesity” is defined as a BMI at or above 95th percentile for the children with the same sex and age.
Overweight and obesity are well-known risk factors for a number of health disorders. Children with excessive weight have medical and psychological problems. The quality of life of these patients is poorer than observed in their lean peers. 2 It was established that obesity in childhood has a significant impact on morbidity and mortality in adulthood. Diseases commonly observed in obese patients are metabolic disorders, type 2 diabetes mellitus (T2DM), cardiovascular diseases, fatty liver disease, musculoskeletal and dental problems, asthma, and many others. 3
Obesity is a metabolic disease leading to low-grade chronic systemic inflammation. 4 The systemic inflammation in obese patients is a result of elevated number and volume of adipose cells that produce inflammatory factors. Obesity-induced inflammation is characterized by abnormally increased level of proinflammatory proteins, especially interleukin 6 (IL-6), tumor necrosis factor (TNF-α), IL-1β, and C-reactive protein (CRP). In addition, excessive adipose tissue affects the immune system by modifying the profile of adipocytokines—the biologically active substances secreted by adipocytes. Obesity leads to elevated serum concentration of leptin, a proinflammatory factor, and to reduced amount of adiponectin, an anti-inflammatory factor. The high levels of leptin in obese patients stimulate adipocytes to release proinflammatory cytokines such as IL-6 and TNF-α and induce changes in the balance between Th1 (T-helper 1)-dependent and Th2 (T-helper 2)-dependent immunologic response. 4 Leptin inhibits Th2-mediated activity and promotes Th1-mediated response. It was suggested that increased level of leptin in the airway tract may explain the correlation between obesity and asthma. 5 The strong correlation between obesity-induced inflammation and systemic diseases such as T2DM or cardiovascular diseases was widely discussed by various authors. 6 –8
The main aim of this study was to review and analyze all available and appropriate scientific researches discussing potential correlations between childhood obesity and otorhinolaryngological illnesses and to present the current knowledge on this topic in a precise review.
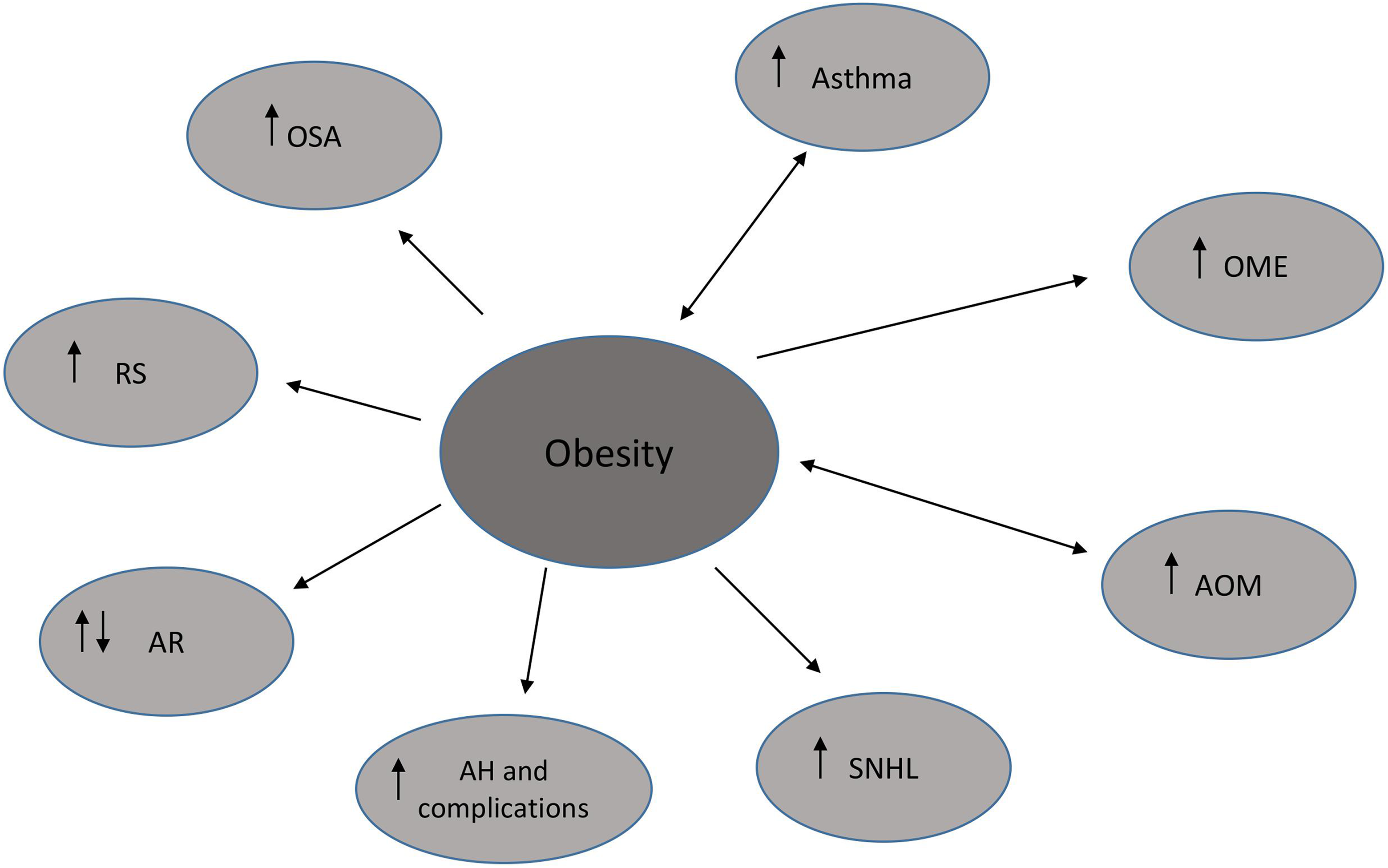
We discussed separately a number of otorhinolaryngological diseases, inter alia, otitis media, hearing loss, obstructive sleep apnea (OSA), adenotonsillar hypertrophy, rhinosinusitis, and their associations with obesity (Figure 1). The analysis of the “OSA, obesity, and asthma” triad in pediatric population was also presented.
Obesity and ENT diseases.
Besides the fact that there are studies presenting positive correlation between childhood obesity and ENT (ear, nose, throat) disorders, the exact association between these entities has not been established yet. 9
Due to the fact that otorhinolaryngological diseases are frequently observed in children, discussing their correlation with obesity is of great importance.
Methods
The Medline and Web of Science databases were searched without time limit using the terms “obesity” in conjunction with “children”, “otitis media with effusion”, “otitis media”, “palatine tonsil”, “adenoid”, “hearing loss”, “rhinosinusistis”, “obstructive sleep apnea” and “asthma”. Boolean operators (NOT, AND, OR) were also used in succession to narrow and broaden the search. Autoalerts in Medline were also run, and reference lists of original articles and review articles were searched for further eligible articles. The search was limited to the English, Polish, and German literature. Articles that did not address the topics, case reports, low-quality studies, and studies based on nonsignificant cohorts were excluded, and the full text of the remaining high-quality articles was reviewed.
Result
Obesity and ENT Diseases
According to recent studies, obese children are more prone to have otorhinolaryngological illnesses than their counterparts with normal weight. It was suggested that obesity may predispose to, for example, otitis media, hearing loss, obstructive sleep apnea, asthma, and adenotonsillectomy complications. Additionally, gastroesophageal reflux (GERD), commonly observed in patients with excessive body mass, may predispose to otorhinolaryngological diseases. Obesity increases periodicity of the lower esophageal sphincter relaxation incidence, reduces sphincter’s contraction, and elevates intragastric pressure. That leads to GERD and subsequently to inflammatory reactions in the upper respiratory tract and ears. 10
Obstructive Sleep Apnea
Obstructive sleep apnea is a common disorder in obese children. Obstructive sleep apnea belongs to large group of sleep-disordered breathing (SDB) and is the most severe form of SDB. Obstructive sleep apnea is characterized by hypercapnia, hypoxia, snoring, recurrent hypopneas/apneas, and arousals during sleeping. The diagnosis is mainly based on polysomnography. 11 Current data present that OSA predisposes to cardiovascular diseases, metabolic syndromes, and neurocognitive disorders. 11,12 It was estimated that approximately 60% of obese pediatric population have OSA, whereas the prevalence of OSA in nonobese children constitutes approximately 1% to 5%. 11,12 According to current knowledge, obesity might predispose to OSA by narrowing the upper airway. The narrowed airway is as a result of fat deposits located in this area. 13 It was suggested that in obese children with OSA, fat-induced obstruction of the upper airway potentially reduces the secretion of growth hormone, subsequently leading to disturbances in growth process. 13 It was also presumed that obesity-induced obstruction of the upper airway potentiates inflammatory responses. Upper airway occlusion and obesity itself might be amplifying processes in immunity activation. 14 According to a randomized, large cohort study, high levels of TNF, a proinflammatory protein released by adipose tissue, decrease contractions of diaphragm and thoracic muscles in obese children deteriorating OSA. 15 The retrospective study on Australian pediatric population revealed that excessive adipose tissue also leads to reduced chest wall compliance, cranial dislocation of diaphragm, and decreased intrathoracic volume. 16
Because of the fact that the most common cause of OSA in children is adenotonsillar hypertrophy, the main way of treatment is adenotonsillectomy/adenotonisllotomy. 13 In the majority of cases, symptoms of OSA disappear after the surgery. Nevertheless, the observational study conducted by O’Brien et al revealed that obesity predisposed to persistent OSA after adenotonsillectomy, irrespective of initial disease severity. The authors established that obesity was the major risk factor for residual OSA after the surgery. The estimated risk of persistent OSA after the surgery was almost 4 times higher in obese individuals than in lean counterparts. 13 This finding suggests that obese pediatric population is less prone to benefit from oropharyngeal surgery (adenotonsillectomy) as a way of OSA treatment.
Moreover, it was established that obesity significantly elevates the risk of OSA development and its severity. The precise review analysis of Tauman et al described that obesity significantly increased the risk of both incidence and severity of OSA. 14 The assessed risk of OSA rose about 12% for every 1 kg/m2 in BMI above mean BMI, adjusted for gender and age. Similar tendencies of elevated risk of OSA in OW and obese were reported in large cohort, cross-sectional studies worldwide. 17 –19 Tauman et al further reported that approximately 50% of examined children with suspected OSA were obese. 14 Such observation was also found in another large-scale study. 20 A randomized large cohort study conducted on elementary schoolchildren presented that waist circumference and BMI were crucial and strong predictors of SDB. No such correlation was found for neck circumference. The results implied that obesity has a strong impact on OSA via systemic rather than local disorders. 15 Kalra et al evaluated extremely OW adolescents (aged between 13-18 years) classified for bariatric surgery. The frequency of OSA in this population reached 55%, and it rose proportional to BMI increase. The authors observed important reduction in OSA severity after the surgery. The studied sample was relatively large for such procedure in such young population. 21 Another large-scale research studied the age-matched association between obesity and OSA, finding that older obese children (8-12 years) were more prone to have OSA than younger (<8 years) ones. 22 Other investigations on representative cohorts consistently revealed that excessive body mass in children significantly increased the risk of OSA. 16,23,24
Canapari et al quantified adipose tissue distribution in children with OSA using magnetic resonance imaging. Authors suggested that visceral obesity constitutes a link between obesity and OSA. They found that visceral fat, independent of BMI, is a crucial prognostic factor of OSA. This observation may elucidate why OSA develops not in all obese children. Nevertheless, this finding requires further analysis on a larger cohort. 25
On the other hand, there are studies that do not support the statement that obesity in children predisposes to OSA. No correlation between excessive weight and OSA incidence was described in a study involving relatively small sample and in a study with specifically selected patients. 26,27
“OSA, Asthma, and Obesity” Triad
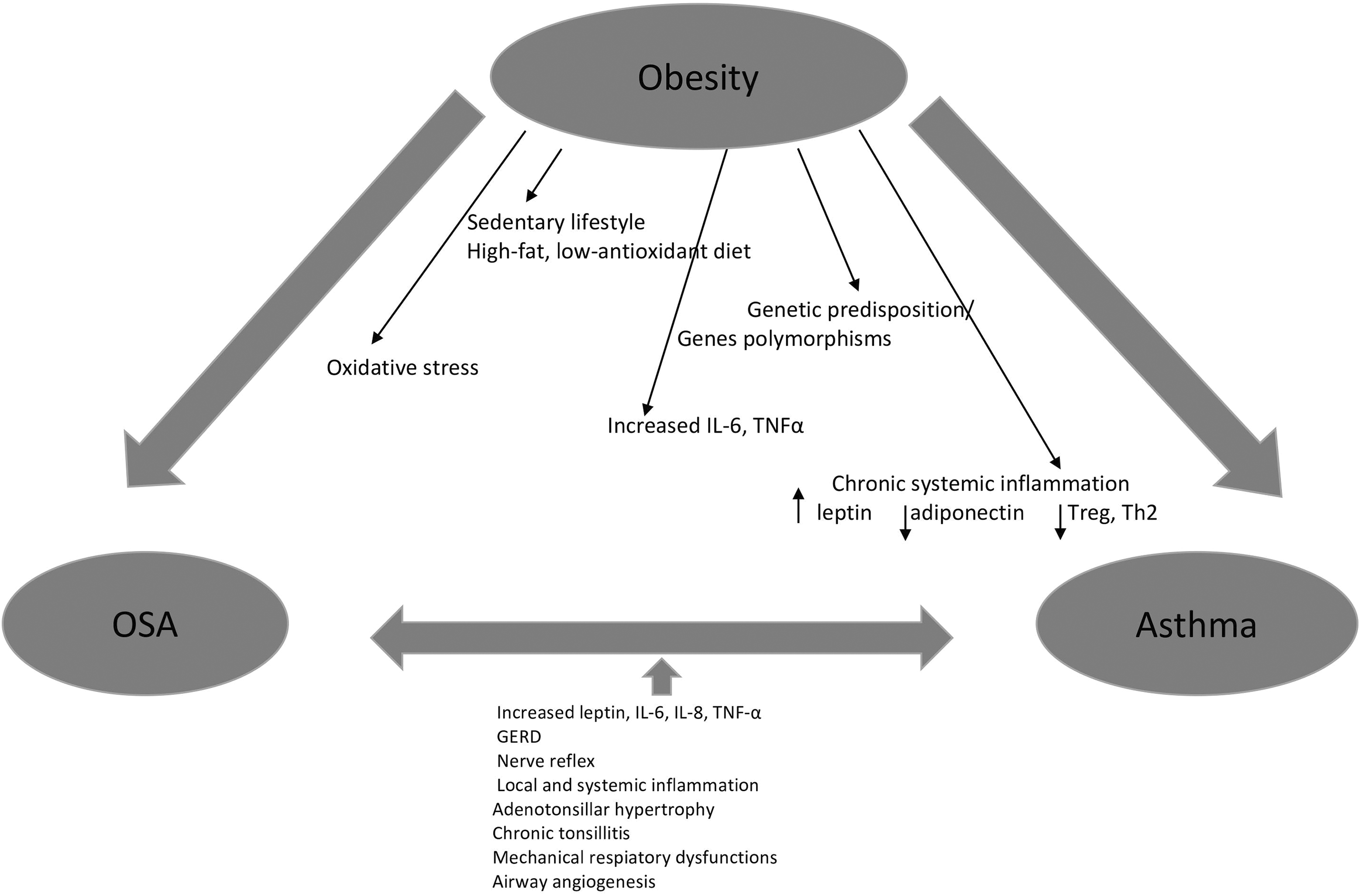
It is now believed that obese children are more prone to develop asthma (Figure 2). 28 –30 Obesity promotes bronchial hyperactivity, airway obstruction, and reduced pulmonary volumes in various mechanisms. Additionally, a correlation between OSA, commonly accompanied by obesity, and asthma is now widely discussed in large-scale studies. 4,31,32
“OSA, Asthma and Obesity” Triad.
The potential links between asthma and obesity comprise eating habits (high-fat and low-antioxidant diet), sedentary lifestyle, and genetic predispositions. 28 It was found that diet rich in saturated fat increases the serum level of circulating factors (IL-6, TNFα, and leptin) that are crucial in inducing asthma. 28 Consequently, such diet activates nuclear factor-κB (NF-κB)–dependent proinflammatory pathways and creates excessive oxidative stress. 28 It was suggested that low consumption of antioxidants, especially carotenoids, vitamin E, and vitamin C, may lead to lower pulmonary function in children. 33,34 Moreover, improper omega-6 (n-6) polyunsaturated fatty acid (PUFA)–n-3 ratio increases the production of leukotrienes. It is known that n-6: n-3 PUFA ratio shifted toward excessive n-6 PUFA is commonly observed in obese children. 28 It was suggested that low vitamin D intake may also promote asthma development via disturbed function of both suppressor T cells and respiratory smooth muscle cells. 35 –37 Moreover, large cohort studies revealed that physical activity leads to hyperventilation and bronchodilation; thus, sedentary lifestyle promotes asthma development. 38,39 Interestingly, it was found that certain polymorphisms in genes β2-adrenergic receptor gene, the TNFα gene, the lymphotoxin-α gene, vitamin D receptor gene, and protein kinase C-α may constitute a link between asthma and obesity. 40,41
It was suggested that obesity-induced systemic inflammation is mainly a result of excessive adipose tissue and insulin resistance and is commonly accompanied by dyslipidemia (low high-density lipoprotein [HDL] concentration and high triglyceride concentration). 42,43 Such systemic inflammation is characterized by increased level of proinflammatory adipocytokines (leptin) and reduced amount of anti-inflammatory adipocytokines (adiponectin and omentin) as well as by Th2 cell suppression and reduced amounts of T-regulatory cells. 42,43 Moreover, a study on a representative sample found that truncal obesity affects diaphragm motility, reduces lung volumes, and leads to pulmonary function deficits. 44
According to various studies, the correlation between asthma and OSA in pediatric population is bidirectional. 45,46 A large-scale study conducted by Chng et al established that children with asthma are more prone to have OSA than those without asthma. 45 Likewise, the authors found that young patients with OSA are more likely to develop asthma than their counterparts without OSA. 45 They also suggested that OSA may even be a predictor of asthma appearance and may also aggravate asthma severity by modifying oropharyngeal reflexes, reducing intrathoracic pressure, and promoting bronchoconstriction. 45 Moreover, it was observed that a mediating factor between asthma and OSA in children is adenotonsillar hypertrophy and chronic tonsillitis. 47 According to authors’ findings, the inflammation in the upper respiratory tract may predispose to the inflammation in the lower respiratory tract (and asthma), whereas the inflammation in the lower respiratory tract may result in adenotonsillar hypertrophy and subsequently lead to OSA. 47 The significant improvement in asthma severity was reported after adenotonsillectomy in children in very large sample studies. 47,48 Besides adenotonsillar hypertrophy, there are other presumed direct links between OSA and asthma including mechanical respiratory dysfunctions, nerve reflex, hypoxia, and inflammation. 32 A meta-analysis conducted by Sanchez et al revealed that the airflow in asthmatics is disturbed, especially during sleeping, because of the reduced functional residual capacity. 31 Consequently, that leads to increased airway resistance and airway collapse. 31 On the other hand, the authors suggested that the turbulent airflow in patients with OSA results in edema and inflammation in the upper respiratory tract and then trigger asthma. 31 It was also found that intermittent hypoxia observed in those with OSA induces oxidative stress and aggravates asthma. 31 On the other hand, reduced pulmonary function in asthmatics exacerbates hypoxia in patients with OSA. 31
It was suggested that another presumed pathogenic factor for asthma development in patients with OSA is leptin. 4,49 Serum leptin concentrations in humans with OSA are significantly elevated and are higher than in patients with similar BMI but without OSA. 4 The experimental study on mice revealed that the role of leptin in the pathogenesis of asthma is mainly based on stimulating the release of proinflammatory cytokines such as IL-6 and TNF-α by adipocytes, inducing airway hyperresponsiveness, and increasing serum immunoglobulin E (IgE) levels. 50 Interestingly, leptin concentration in a group of 102 children with asthma remained increased after normalizing BMI, contradictory to nonasthmatic peers. 49 This observation supports the potential role of leptin in asthma pathogenesis.
Another OSA–asthma link is called “nerve reflex.” It is a bronchoconstriction caused by the stimulation of the oropharyngeal neural receptors in OSA. 4
The local and systemic inflammation in patients with OSA influence asthma, and the systemic inflammation observed in patients with asthma influence OSA. 4 It was suggested that the local inflammation in OSA is a result of the mechanical disturbances in airway and is characterized by increased level of IL-6, IL-8, TNF-α, and vascular endothelial growth factor (VEGF). 4,51 –53 Studies showed that the systemic inflammation in OSA is mainly caused by the coexisting obesity and recurrent episodes of hypoxia. 4 The fact that the respiratory muscles are highly sensitive to such inflammatory environment explains the improper respiratory functions. 4
The VEGF promotes bronchial inflammation, hyperresponsiveness, and vascular remodeling in patients with asthma. 4 According to recent studies, increased levels of VEGF are observed both in patients with asthma and in patients with OSA. 54,55
Finally, GERD that is commonly observed in patients with OSA may mediate and induce asthma attacks. Vagal stimulation of esophageal mucosa by gastric acid results in bronchospasm. 56,57
Adenotonsillectomy Perioperative Complications
It is possible that obesity in children correlates with acute perioperative complications of tonsils/adenoids removal surgery. 58 A large cohort study revealed that children with obesity were more prone to develop immediate hemorrhage after tonsillectomy/adenotonsillectomy. 58 The risk of postoperative bleeding was about 2.3 times higher in obese patients in this sample. In contrast, no association between immediate hemorrhage after the surgery and chronic tonsillitis, peritonsillar abscess, adenotonsillar hypertrophy, OSA, and gender was found. 58 Gleich et al described that childhood obesity is an irrespective predictor of perioperative complications of tonsillectomy. The most frequent complications were airway obstruction and intraoperative severe hypoxemia. 59 Other perioperative problems in OW/obese children like higher frequency of laryngoscopy attempts, difficult mask ventilation, and intraoperative desaturation were also described by these authors. 59 Additionally, the study found that postoperative outcomes in obese children were significantly worse than in nonobese peers. 59 Obese patients were also more prone to have perioperative respiratory complications such as acute or chronic respiratory failure/insufficiency. 59 Such problems are commonly reported by anesthesiologists at anesthesia induction and during the postanesthesia care unit in large cohort randomized studies. 60 –62 Obese patients were usually forced to stay in the hospital longer after the surgery than nonobese ones. 63 They also underwent more episodes of postoperative hospitalizations in comparison to lean peers. 63 It was established that OW/obesity was an independent prognostic factor for longer postoperative length of hospitalization in a large cohort of pediatric population. 63 Obese children undergoing adenotonsillectomy were also more prone to have postoperative OSA. 60
Post-tonsillectomy Obesity
Several studies on large cohorts of children undergoing adenotonsillectomy found the tendency of gaining weight after the operation. 64 –66 In a large group of pediatric patients, the increase in weight was higher than expected and was observed both in OW and in lean patients. 67,68 The potential mechanisms of weight gain after tonsil removal included (1) reduced postoperative OSA-induced hyperactivity (reduced hyperactivity results in decreased calories burning), (2) reduced calorie burnout during the night because of improved breathing and air passage, and (3) overeating after removal of odynophagia/dysphagia induced by tonsils remaining chronically inflamed. 69,70 Weight gain after the adenotonsillectomy may also be a result of increased serum concentration of insulin-like growth factor I (IGF-I) and IGF-binding protein 3 in patients with OSA. 71,72
Otitis Media With Effusion
Otitis media with effusion (OME) is a condition of fluid accumulation in the middle ear without symptoms of acute inflammation such as otorrhea, otalgia, or fever. It is a common disease and important cause of hearing loss in children. 73 The OME may result in speech, development, growth, and general health disorders. 73 Approximately 90% of children undergo OME in the preschool age, with the highest prevalence between 6 months and 4 years of age. 74 It is suggested that there is a link between obesity and OME.
Kim et al examined numerous groups of children aged 5.2 ± 3.2 years with OME. The authors observed that the prevalence of OME cases in obese group was significantly higher than in underweight, normal, or OW groups. 75 The positive correlation between recurrent OME and both high BMI and total serum cholesterol level was also described. Moreover, the authors established that obese children underwent tympanostomy tube (TT) placement significantly more frequently than nonobese children. No correlation between the severity of OME and obesity/OW was found. 75 These outcomes confirmed the previously described results of the study on a group of 155 children conducted by the same authors. 76
Moreover, according to the current knowledge, there is also a correlation between obesity and both endocrinology and immunity. Briefly, adipose tissue interferes with endocrine system and immunity. A meta-analysis conducted by Cottam et al hypothesized that obesity predisposes to OME via inducing changes in the levels of various inflammatory cytokines, especially IL-6. 77 It was found that serum IL-6 levels were higher in obese patients than in lean ones. 77 Interestingly, the presence of IL-6 in the middle ear (ME) fluid was identified in the majority of patients with chronic OME. Moreover, amount of IL-6 correlated positively with TNF-α concentration. 78 In chinchilla model, the elevated level of IL-6 in the middle ear upregulated mucin secretion by the middle ear epithelium. 79 It may explain the IL-6-mediated correlation between obesity-induced inflammation and OME.
Obesity may predispose to OME also in a mechanical way. 80 According to Al-Saab et al, depositions of the adipose tissue around eustachian tube (ET) and its opening led to obstruction and closing of this structure. 80 Permanent occlusion of ET generated negative pressure in the middle ear and subsequently resulted in fluid production and OME. 80 It was suggested that laryngopharyngeal reflux (LPR), commonly observed in obese, induces OME via gastric efflux that gets into ME through nasopharynx and ET. 80 Authors of this study evaluated pepsinogen, the enzyme produced by gastric cells, in the ME effusions in children with OME. They identified the presence of pepsinogen in 84% of cases. Consequently, the authors emphasized the significant role of gastric reflux in developing OME. 80 It was also hypothesized that gastric acid that reaches ME causes dysfunction of the mucociliary clearance in the ME cavity and in ET. A controlled study conducted by Abtahi et al revealed that the frequency of OME and acute OM in youths with GERD was significantly higher than in healthy controls. 81 Positive correlation between LPR/GERD and OME was also found by other researchers in a controlled study on pediatric sample. 82
Furthermore, a large population-based study reported that diet rich in high amounts of fat significantly increased the risk of OME in children. 83 Such diet promoted OME via inducing ET dysfunction and upper respiratory tract infections. 83
Acute Otitis Media
Acute otitis media (AOM) is considered to be the second most common cause of family physician visits in pediatric population. 84 Approximately 60% to 85% of children have AOM during the first year of life. Additionally, this disease is the commonest reason for prescribing antibiotics in children.
According to recent studies, factors linking obesity/OW and AOM in children are similar to those described in OME. Kuhle et al examined 282 elementary schoolchildren reporting that obese and OW individuals had higher incidence of OM. 85 These children were also more prone to undergo recurrent episodes of OM than the lean ones. Socioeconomic factors such as allergy, a history of breast-feeding, and chronic tonsil/adenoid disorders were excluded as confounders in the correlation between OM and obesity.
The analysis of a large population of American school-aged children (42.1 million of patients) revealed that the frequency of AOM was significantly higher in obese children than in lean ones. 86 Obese children were more prone to undergo AOM at least annually in comparison to nonobese children. No such correlation was found for OW ones. 86
Interestingly, various studies found different correlation between otitis media (OM) and obesity, suggesting that OM predisposes to obesity in children. 87,88 It was suggested that high exposure to OM may modify the taste sensation on the anterior part of the tongue by damaging the chorda tympani nerve function. 87 As a result, children with recurrent OM have less preference to consume vegetables and fruits and are more prone to eat sweets and high-fat products. 87 Other authors consistently claimed that a history of severe OM episodes in childhood predisposes to decreased consumption of vegetables, increased sweet intake, and subsequently to OW. 88
Nelson et al. conducted a large cohort study on a representative group of toddlers trying to assess whether the toddler’s size at the age of 2 months predisposed to recurrent OM or if it predicted TT insertion by the age of 2 years. 89 The toddler’s size was defined using weight-for-length (WFL) measurement. The infants’ size was classified as obese (WFL above 95th percentile) or OW (WFL between 95th and 85th percentile). The authors concluded that high level of WFL during the first 2 months of life did not predict developing OM later in life. However, the follow-up of these children at the age of 2 years presented significant positive association between obesity/OW status and a history of TT placement. 89 According to the results, obese individuals underwent TT placement more often than lean ones. 89 Similar correlation was found for obesity and a history of recurrent OM. 89 It was suggested that the association between high WFL and the risk of TT placement might be a result of concomitant adenoid hypertrophy observed in obese patients. 89
Sensorineural Hearing Loss
Sudden sensorineural hearing loss (SNHL) is a rapidly and suddenly developing hearing disorder that evolves within 72 hours. This condition is described as an audiometric SNHL over 3 adjacent pure-tone frequencies of 30 dB or more. In majority of cases, SNHL affects only 1 ear. Mostly, the exact cause of this disease remains unknown. The prevalence of SNHL incidence increases after the age of 65 years and is low in pediatric population.
Lalwani et al presented for the first time the association between obesity and unilateral SNHL in a large population of children. 90 Authors found that obese children had higher hearing thresholds across all frequencies. Moreover, they had approximately 2-time increase in the odds of unilateral low-frequency SNHL. 90
In adults, it was established that hearing loss might be affected by obesity in dependent and independent ways. 91,92 Obesity-induced secretion of proinflammatory cytokines may directly lead to cochlear damage. 90 Low concentration of adiponectin might also predispose to hearing loss. A meta-analysis conducted by Reilly et al presented that low levels of adiponectin were commonly observed in obese children. 93 Hypoadiponectinemia-induced hearing dysfunction is presumably a result of improper expression of C-reactive protein, reduced TNF-α-induced NF-κB activation through a 3’-5’-cyclic adenosine monophosphate-dependent pathway, and suppressed IkappaB kinase (IκB) phosphorylation. 94 Disturbed hypoadiponectinemia-mediated AMPK-dependent endothelial vasorelaxation and angiogenesis may also result in hearing deficiency. 95,96 Indirect reasons of obesity-induced hearing loss are cardiovascular diseases and T2DM, conditions commonly observed in OW youths. 90 Systemic diseases such as metabolic syndrome, T2DM, and cardiovascular diseases leading to SNHL in adults may also predispose to SNHL in pediatric population. Nevertheless, the straight cause of SNHL in obese children has not been elucidated yet.
Lymphoid Tissues: Adenoid, Palatine Tonsils, and Lingual Tonsils
A recent study on obese pediatric population aged between 3-18 years revealed that these patients had significantly higher incidence of both adenoid and tonsillar hypertrophy in comparison to nonobese subjects. 2 The analysis of Narang et al. consistently reported that the frequency of adenotonsillar hypertrophy is significantly higher in obese children than in lean ones. 12 It is suggested that the linking factor between obesity and lymphoid tissues size is endocrine-mediated somatic growth that predisposes to larger tonsils, fat pads, soft palate, and tongue. 12
Another research compared palatine tonsil dimension (volume, weight, width, height, and thickness) in obese and nonobese children with SDB. 97 The results described that in the first group, tonsils were significantly more enlarged than in the latter one. Authors suggested that enlarged tonsils in obese children might have a bigger impact on the upper airway obstruction than in their normal-weight counterparts. 97 Nevertheless, the results require confirmation on larger sample studies. It was also observed that the prevalence of lingual tonsils hypertrophy was significantly higher in obese children than in nonobese ones. In obese group, the frequency of lingual tonsils hypertrophy measured by sagittal fast spin-echo inversion recovery imaging was greater in those with a history of tonsillectomy. 98
Interestingly, Megale et al’s analysis of a relatively small group of children with GERD revealed that approximately 25% of studied children had recurrent tonsillitis (RT). 99 The antireflux treatment combined with antiallergic drug led to removal of RT in almost 91% of patients. 99 However, antireflux therapy alone was able to cure only 18.18% of children. 99 These results require further analysis on the large-scale studies.
Arens et al examined lymphoid tissue in a group of children with OSA and its correlation with BMI. 100 Lymphoid structures including adenoids, palatine tonsils, and retropharyngeal nodes were assessed in this study. Authors did not find positive correlation between lymphatic tissues size and high BMI. However, sizes of tongues, mandibles, and parapharyngeal fat pad were significantly higher in obese that in nonobese children. 100
It is well known that improper serum lipids level in childhood might cause severe long-lasting metabolic and cardiovascular disorders. According to that, Zong et al revealed that serum level of HDL-C in individuals with SDB was inversely associated with adenotonsillar hypertrophy score. 101 Briefly, HDL-C concentration was lower in children with more enlarged adenoids and tonsils. After adenotonsillectomy, the amount of HDL-C increased less in obese patients than in nonobese patients. 101 These observations require further investigation on larger cohorts.
Allergic Rhinitis
Allergic rhinitis (AR) is a common disorder in pediatric population. The estimated prevalence of this noninfectious rhinitis reached 1.2 million children worldwide and is still rising. 102 AR is allergen-induced, IgE-mediated response of nasal mucosa. It is characterized by nasal itching, nasal obstruction, and rhinorrhea. Allergic rhinitis may be classified as intermittent or persistent in accordance with symptom frequency. 102
In adults, it was suggested that obesity predisposes to AR in an inflammatory way by modifying adipocytokines profile, leptin, and adiponectin and by stimulating the synthesis of proinflammatory cytokines and acute-phase proteins. 103
Saadeh et al examined a large French pediatric population finding that high BMI (defined as obesity or OW) correlated positively with AR incidence. 104 Increased frequency of AR was also observed in a large cohort of obese Chinese children. In contrast, no such association for asthma, drug, and food allergy was identified in this group. 105 Other authors consistently described positive connection between childhood obesity and AR incidence in numerous cohorts. 106 Kim et al studied the correlation between AR in a large group of children and various diet components. They established that high-fat and low-carbohydrate diet predisposed to AR. No significantly similar association was observed for atopic dermatitis and asthma. 107 Clear explanation of the mechanism combining AR and high-fat consumption has not been established so far. Nevertheless, it was suggested that some types of fatty acids affect the immune system. 108 Linoleic acid, one of the fatty acids, converts to prostaglandin E2 (PGE2) through arachidonic acid formation, 108 whereas PGE2 induces allergic reaction via stimulating production of IgE. 108 Inconsistently, study based on a large pediatric population conducted by Kusunoki et al revealed that the prevalence of AR was significantly lower in obese school-aged children, especially in boys, compared to lean individuals. 109 The suggested reason of such negative association between obesity and AR is based on immunomodulatory effects of obesity. 5 Namely, a high level of leptin that is observed in obese people inhibits Th2 (T helper cell 2) response and increases Th1 (T helper cell 1) response. 5 As AR is claimed to be a disease with the predominance of Th2-mediatied mechanisms, the obesity-induced domination of Th1 response might explain this negative association between obesity and AR. The difference between genders observed by Kusunoki et al might have been caused by various influences of female and male sex hormones on Th1/Th2 balance. 109 Another study on a large group of children found no positive correlation between OW/obesity and rhinitis (both allergic and nonallergic). 110 The authors revealed that youths, both girls and boys, with central obesity had lower frequency of AR than those with normal waist circumference. 110 No such correlation was observed for general obesity defined as high BMI. 30
Consistently, Sidell et al’s analysis of a large group of American school-aged children did not reveal positive association between obesity and increased risk of AR in contrast to AOM. 86 No association between high BMI and AR in youths was reported in an international, randomized large cohort study. 111
Rhinosinusitis
Rhinosinusitis (RS) is an inflammatory disease of nose and paranasal sinuses with a high prevalence in children. 112 Rhinosinusitis is divided into 2 main groups, acute RS (ARS) and chronic RS (CRS), depending on the symptoms duration. The ARS is characterized by sudden beginning of 2 or more specific RS symptoms including nasal obstruction, nasal secretion, hyposmia, sensation of pain/pressure in the midface, and coughing that last less than 12 weeks. The CRS is a condition of RS persisting for over 12 weeks with main complaints such as postnasal drip, chronic cold, obstruction of the nasal cavity, and rhinorrhea. The main difference between ARS and CRS is based on the period of clinical symptoms. 112
In adults, it was suggested that obesity predisposes to both ARS and CRS in an inflammatory way by modifying adipocytokine profile, leptin and adiponectin, and stimulating the synthesis of proinflammatory cytokines and acute-phase proteins. 103 A cross-sectional, large-scale study on a group of Japanese adults revealed significant, positive association between high BMI and the frequency of paranasal sinuses disease (PSD). 113 The authors established that obesity and PSD were not actually mediated by inflammation but rather by airway structural problems related to obesity or obesity-related lifestyles. They suggested that increased blood glucose levels in obese could predispose to PSD by inducing improper immune function or improper ciliary motility. 113 Nevertheless, the certain mechanisms linking these disorders have not been established yet.
Unfortunately, data evaluating association between obesity and PSD in pediatric population is sparse, poorly understood, and conflicting. Little is known about the correlation between OW/obesity and RS/sinusitis in children. The exact immunologic, physiologic, genetic, mechanic, and environmental mechanisms combining PSD and childhood obesity are still not clarified. 114 The majority of research analyzing the connection between OW/obesity and nasal/sinonasal disorders focus on AR and not on RS.
Nevertheless, the study on a large group of pediatric population conducted by de Sousa et al revealed a positive correlation between sinusitis and obesity in children aged 5 to 19 years. 115 The authors suggested that the risk factors for sinusitis in obese children were GERD and increased level of proinflammatory cytokines. On the other hand, Sidell et al’s analysis of a large sample of American school-aged children did not reveal positive association between obesity and increased risk of CRS. 86
In addition to that, Megale et al assessed a group of pediatric population with GERD. 99 The detailed analysis revealed that the initial symptom of GERD in almost 70% of patients was chronic nasal obstruction. Approximately 56% presented nasal secretion and about 47% presented nasal itching as initial GERD symptoms. Interestingly, 41.17% of patients with nasal disorders experienced full removal of rhinologic symptoms after antireflux therapy. 99
The association between RS and GERD in pediatric population has already been discussed by various authors. 116,117 Many studies found that antireflux treatment for GERD led to removal or improvement in RS symptoms. However, little is known about the exact correlation between high weight and RS in children.
Due to the fact that chronic RS might be caused by GERD, and that GERD is commonly observed in obese children, more studies assessing the potential association between RS and obesity are needed.
Discussion
Obesity in pediatric population is a crucial problem worldwide. It is a systemic disease with potentially life-threatening consequences. The prevalence of this disorder in youths is dramatically increasing all over the world. Obesity leads to many physical and social problems. Children with abnormally high BMI are more prone to have T2DM, cardiovascular diseases, fatty liver disease, OSA, and other complications. According to the current knowledge, various otorhinolaryngological illnesses are more frequently observed in this group of patients. Studies suggest that there is a correlation between childhood obesity and OME, AOM, adenotonsillar hypertrophy, AR, RS, SNHL, OSA, and asthma. Nevertheless, the results of these researches remain inconsistent. Many authors revealed that obesity predisposed to various ENT abnormalities, whereas others did not find such correlation. Most of the studies on the association between childhood obesity and ENT diseases revealed that obesity predisposes to OME, recurrent episodes of AOM, OSA, asthma, adenotonsillar hypertrophy, peri- and post-operative complications of adenotonsillectomy and to AR. It was also found that LPR/GERD predisposes to various ENT inflammatory diseases, especially OM. Unfortunately, little is known about obesity-induced RS, adenotonsillitis, and sudden SNHL so far.
The exact pathophysiologic mechanisms linking ENT diseases and obesity are still not fully understood. It is believed that adipose tissue, as an endocrine organ, modifies immunity, produces many proinflammatory factors, and thus induces other diseases. Excessive adipose tissue located in the head and neck region and upper airways also promotes otorhinolaryngological disorders.
The main limitation of this review is the relatively small number of studied researches. This is a result of the small amount of studies reported in the literature concerning the relationship between childhood obesity and otorhinolarynglogical diseases. Nevertheless, we tried to analyses all available, significant, and appropriate studies on this matter.
In conclusion, obesity predisposes to OME, AOM, recurrent OM, OSA, SNHL, and post-/perioperative complications of adenotonsillectomy. Obesity in children significantly correlates with OSA and asthma.
Childhood obesity, in the vast majority of cases, is a result of improper eating habits; thus, modifying diet and normalizing body mass could lead to reduction in many serious diseases. Besides being involved in many serious chronic systemic diseases and a number of ENT diseases, obesity also carries a considerable burden of mental dysfunctions. According to that, this review is an interdisciplinary research and is directed toward doctors of various specialties, psychologists, dieticians as well as toward parents, caregivers, and teachers. This knowledge may result in avoiding many serious diseases and may improve management of these diseases if they develop.
Because of the fact that the prevalence of childhood obesity is significantly rising and ENT diseases are leading diseases in pediatric population, more studies assessing the exact correlation between these disorders should be conducted.
Key Messages
The prevalence of obesity in children is rising. Obesity may predispose to otorhinolaryngological illnesses by interfering with the immune system and in a mechanic way. Obesity affects the immune system: increases serum IL-6, TNF, CRP, and leptin levels and reduces adiponectin amount. Obesity in children correlates significantly with OSA and asthma and forms “OSA, obesity, and asthma” triad. Obesity predisposes to OME, AOM, recurrent OM, OSA, SNHL, adenotonsillar hypertrophy, and post-/perioperative complications after adenotonsillectomy. The exact pathophysiologic mechanisms linking ENT diseases and obesity are not fully understood.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.