
Abstract
Background:
Ventilation tube (VT) insertion is the most common treatment for otitis media with effusion (OME). However, OME recurrence and persistent tympanic membrane (TM) perforation after VT removal are encountered in a certain percentage of such children.
Methods:
This study was performed to determine the outcomes of children who underwent long-term VT insertion. A total of 326 ears from 192 patients were analyzed. The associations among the patient age, sex, history of OME, history of repeated acute otitis media, placement duration, whether the VT had been removed intentionally or spontaneously, and the outcome (persistent TM perforation or OME recurrence) were analyzed. The outcomes of multiple VT tube insertions were also reviewed. We also analyzed whether or not local or general anesthesia was associated with the early spontaneous extrusion of the VT.
Result:
The OME recurrence and TM perforation rates were 29% (96/326 sides) and 17% (57/326 sides), respectively, for first insertions. In addition, 96 (29%) sides underwent ≥2 insertions. The shorter the duration for which the VT was retained in the middle ear, the more significant the rate of increase in OME recurrence. The OME recurrence was observed more often when VT was spontaneously removed than when intentionally removed. The rate of persistent TM perforation was significantly associated with male sex. Persistent TM perforation was not observed in patients who underwent 4 or 5 insertions. The anesthesia method did not significantly influence the timing of spontaneous extrusion of VT.
Conclusion:
The retention period of VT should be at least 2 years, and VT removal at the age of 7 might be a viable strategy. Multiple VT insertions are recommended for patients with recurrent OME. Ventilation tube under local anesthesia is an effective option for tolerable children.
Keywords
Introduction
Otitis media with effusion (OME) is one of the most frequently observed conditions, affecting 80% of the pediatric population at least once before school. It is the most common cause of hearing loss in school-aged children. 1,2 Patients with OME that persists for more than 3 months with resistance to conservative therapy are frequently treated by ventilation tube (VT) insertion. However, OME recurrence and persistent TM perforation after VT removal are encountered in a certain percentage of such children. 3 -7 The optimal timing for VT removal thus remains controversial. 8
In most cases, the VT spontaneously extrudes 6 to 18 months after surgery. Complete healing of the TM occurs through the squamous layer’s migration, together with the fibrous and mucosal layers. 9,10 However, failure of TM closure and persistent TM perforation are widely acknowledged complications associated with long-term VT use. 11 Additional surgery for myringoplasty is required to close the TM perforation.
The optimal timing for removing the VT is a topic of debate. If clinicians shorten the VT retention duration too much in order to avoid TM perforation, the insertion period may not be adequate, and OME may relapse. 5 Two years has been considered the standard duration for VT insertion, but we often encounter relapse of OME in cases where the VT was removed over 2 years after insertion. Therefore, deciding on the appropriate timing of VT removal remains difficult.
Repeat VT insertion is occasionally needed. The outcomes of a single insertion and a mixture of multiple insertions have been reported, but the individual outcomes depending on the number of insertions have rarely been reported. 1,3,6
Furthermore, no study has yet compared the effects of deliberate removal with those of spontaneous removal. Whether or not the quality of VT insertion under local anesthesia is as tolerable as that under general anesthesia is of some concern, especially when attempting to deliver informed consent to parents. For children younger than 2 years old, a VT can be inserted at the outpatient clinic under local anesthesia. However, for older children (older than 4 years), VT insertion under local anesthesia may be more difficult, so general anesthesia is used. The accuracy of insertion tends to be better under general anesthesia as children may otherwise have difficulty remaining calm during insertion. The main point of concern is whether or not insertion under local anesthesia is good enough for VT stability, as the surgeon needs to perform the insertion quickly and without great deliberation. Of note, most previous studies collected data from patients with different VTs, 1,3,6 thus reducing the quality of their analyses.
Given the abovementioned concerns, the present study explored the rate of OME recurrence, permanent perforation, and normalization of the middle ear according to the age, sex, history of OME, history of repeated acute otitis media (AOM), placement duration, and whether VT was removed intentionally or spontaneously. We reviewed the individual outcomes depending on the number of VT insertions. We also analyzed whether or not local or general anesthesia was associated with early spontaneous extrusion of VT. A long-term VT (Koken B-type, #1542; silicone, inner diameter: 1.6 mm, diameter of the inner flange: 4 mm, diameter of the outer flange: 3 mm, length: 2.0 mm; Koken Co, Figure 1) was used for all patients.
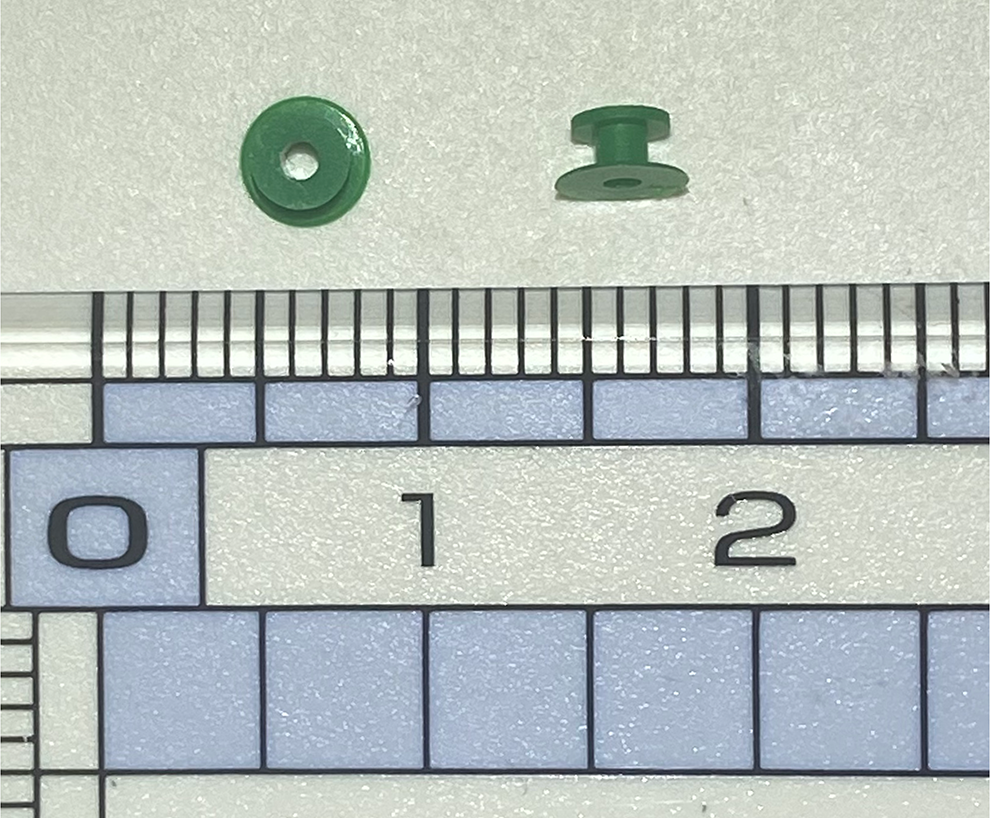
The size of the Koken B-type tube. The minimum scale on the ruler is 1 mm.
Materials and Methods
Patients
The current study evaluated children with persistent OME who underwent the Koken B-type VT insertion between October 2011 and March 2016 and whose outcomes after the first VT removal were observed. The criteria for VT insertion were as follows: (1) OME resistant to conservative therapy for over 3 months or (2) repeated AOM. Patients with congenital diseases related to maxillofacial anatomical changes, such as Down syndrome and cleft palate, were excluded from the study. All procedures were performed at Tohoku Rosai Hospital. No patients had a history of VT before being included in this study.
This study was approved by the institutional review board of Tohoku Rosai Hospital (no.: 18-19). The protocols used in this study were approved by the hospital’s protection of human subjects committee.
Surgical Technique
Depending on the patient’s age and coexisting adenotonsillar hypertrophy, surgery was performed under either general or local anesthesia. The VT was inserted in the anteroinferior quadrant under a microscope. In cases treated under local anesthesia, children were held by a parent who was sitting on the ear, nose, and throat (ENT) examination chair, and the children’s heads were held against the parent’s chest by a nurse.
Follow-Up
Patients were followed up a week later and then every 3 months thereafter. When not spontaneously removed, VTs were generally removed 2 years after insertion or when intractable otorrhea occurred. When patients did not visit our hospital regularly, the timing of VT removal was delayed. The VTs were reinserted in patients who presented with recurrent OME. When TM perforation persisted, patients were followed up until they regained Eustachian tube function, and myringoplasty was subsequently performed.
Statistical Analyses
The relationship between clinical factors (age, sex, history of OME or repeated AOM, duration of retention, and whether VT was removed spontaneously or intentionally) and outcomes (OME recurrence or persistent TM perforation) was analyzed using multivariate logistic regression analyses with the statistical software program Stata/MP, version 14.0. For continuous predictors (age and tube retention period), the OR represents the increase in odds of the outcome with every single-unit (month) increase in the input variable. A survival curve was constructed according to the Kaplan-Meier method and compared using the log-rank test. For the Kaplan-Meier analyses, the event was defined as spontaneous VT extrusion, and intentional removal was treated as censored. Pearson χ2 test was used to determine the difference between the outcomes between 2 groups divided by the cutoff value. Statistical significance was set at P < .05.
Results
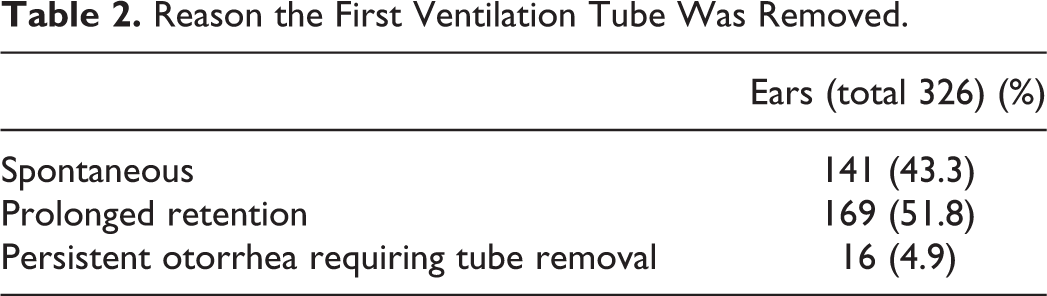
A total of 192 (326 sides) patients were followed up at least until the outcomes of the first VT removal were determined. The patient characteristics are summarized in Table 1. The average follow-up period of the total patients was 32 months. The outcomes of VT insertions (1-5 insertions) are shown in Figure 2. Figure 3 shows the outcomes of ears at each time point after the first VT insertion. The average first VT retention time was 27 months (range, 1-64 months). Table 2 summarizes the cause of VT removal. Persistent otorrhea was defined as a period of secretion lasting over 2 weeks observed by an otolaryngologist during follow-up. The overall OME recurrence and persistent TM perforation rates with first VT were 29% (96/326 sides) and 17% (57/326 sides), respectively.
Summary of the Clinical Features of the Patients.
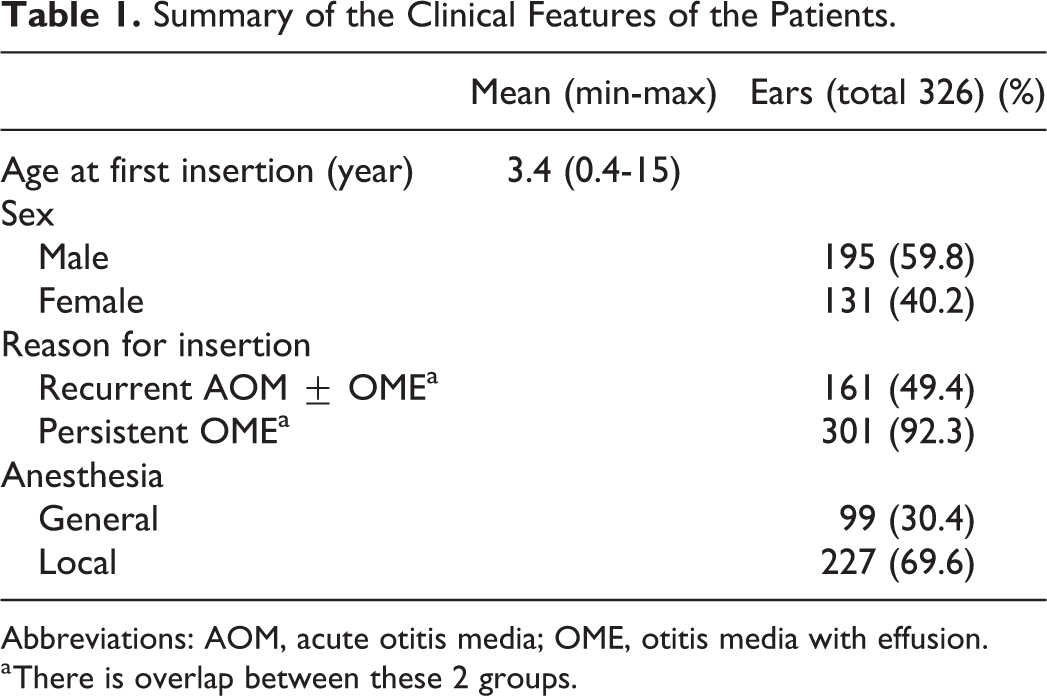
Abbreviations: AOM, acute otitis media; OME, otitis media with effusion.
a There is overlap between these 2 groups.
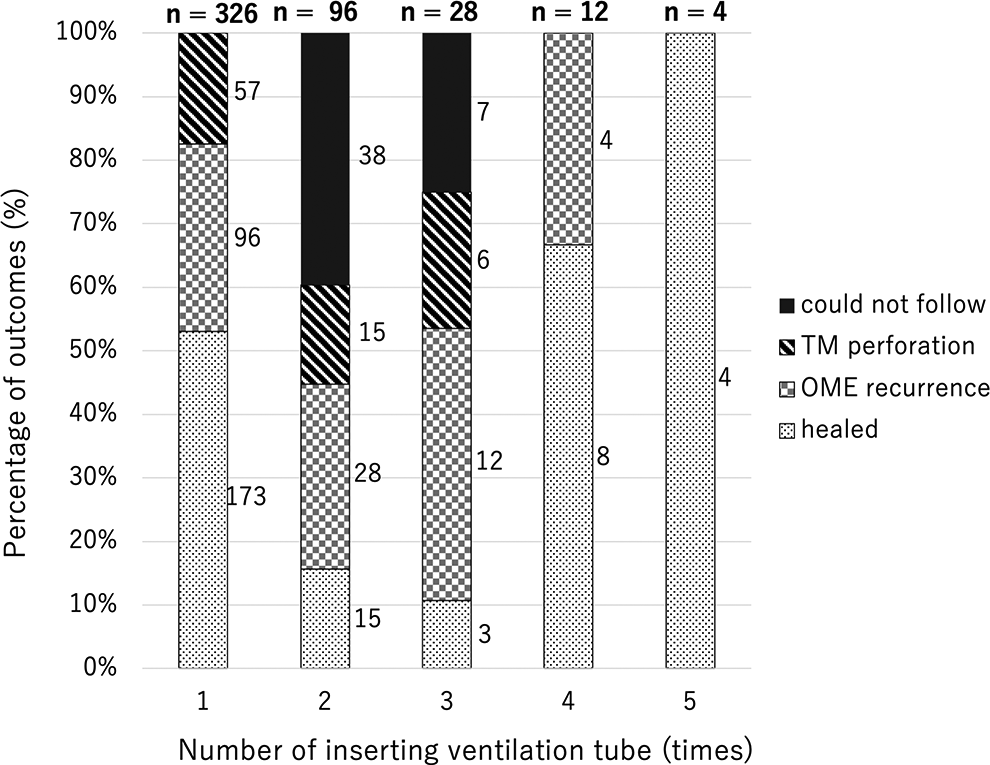
Outcomes of 1 to 5 times of ventilation tube insertion. Data were expressed as rates (%). OME indicates otitis media with effusion; TM, tympanic membrane.
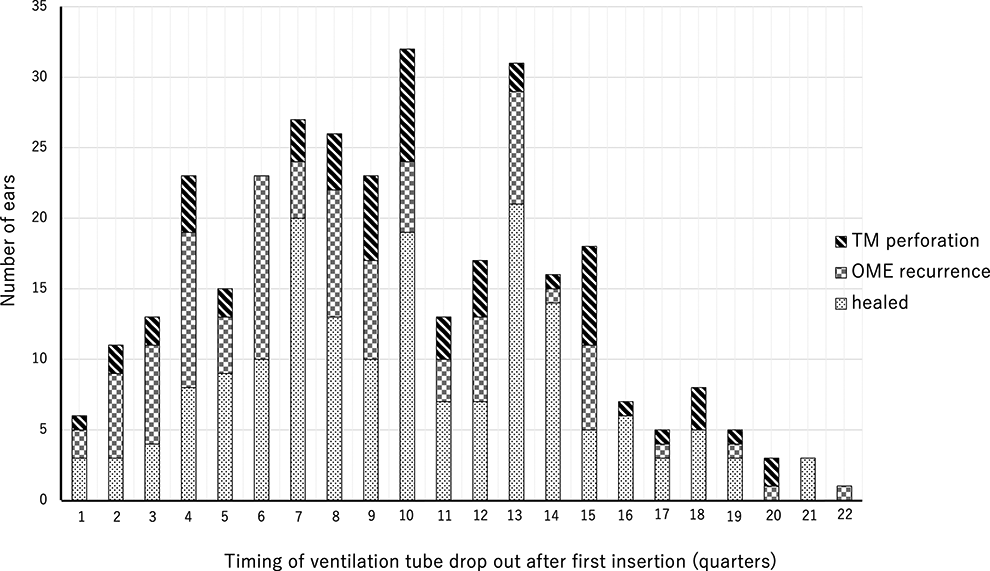
Outcome of the first insertion of a ventilation tube is based on the retention period. One quarter is 3 months. OME indicates otitis media with effusion; TM, tympanic membrane.
Reason the First Ventilation Tube Was Removed.
Analyses of Factors Associated With OME Recurrence and TM Perforation After the First VT Removal
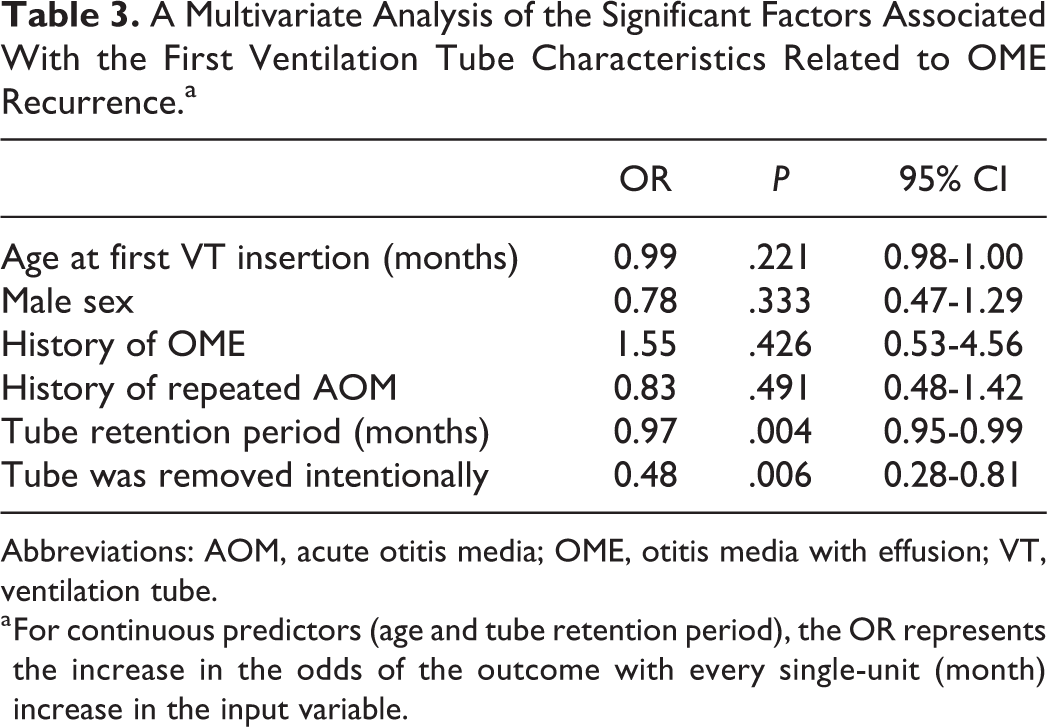
The clinical factors on OME recurrence after removal of the first VT are presented in Table 3. The shorter the duration of VT retention in the middle ear space, the more significant the rate of OME recurrence. The mean first tube retention time for patients with OME recurrence was 22.7 months, compared to the 29.0 months reported for those without recurrence. The Youden index showed that the cutoff point was 25 months (area under the receiver operating characteristic curve: 0.639). The VT removal ≥25 months after insertion had a significantly lower OME recurrence rate than removal within 25 months (P < .0001). The VT intentionally removed by surgeons was associated with a lower rate of recurrence of OME than spontaneous removal. Histories of OME and AOM were not associated with OME recurrence.
A Multivariate Analysis of the Significant Factors Associated With the First Ventilation Tube Characteristics Related to OME Recurrence.a
Abbreviations: AOM, acute otitis media; OME, otitis media with effusion; VT, ventilation tube.
a For continuous predictors (age and tube retention period), the OR represents the increase in the odds of the outcome with every single-unit (month) increase in the input variable.
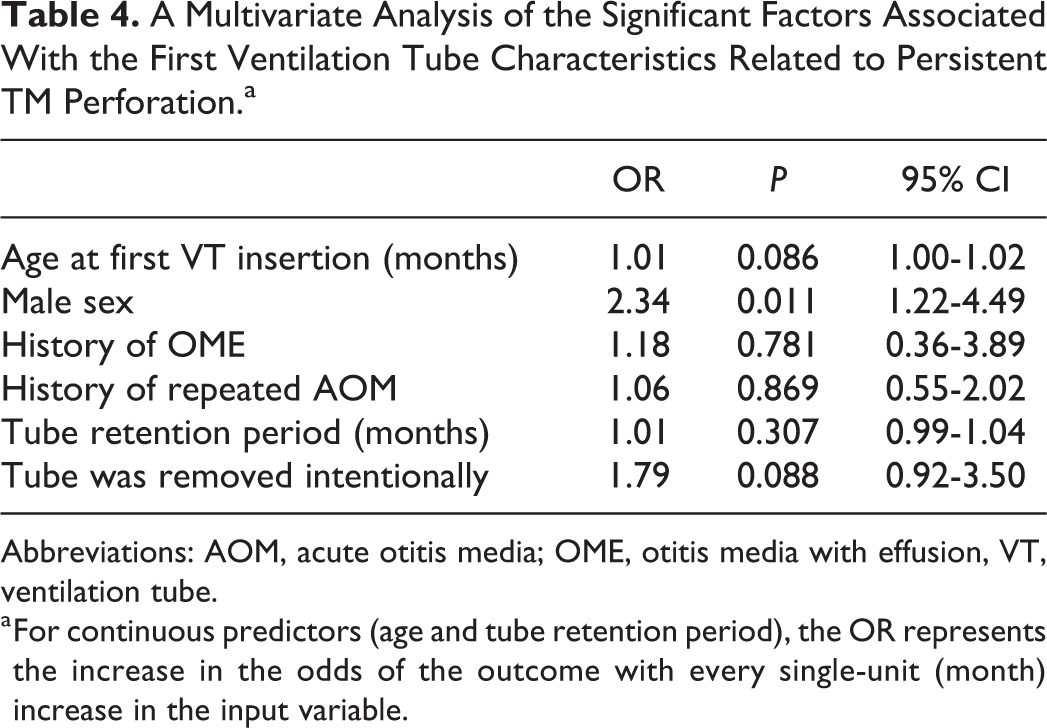
The clinical factors associated with persistent TM perforation after the first VT removal are provided in Table 4. The persistent TM perforation rate was significantly higher in males than in females. Patients with persistent TM perforation had an average tube retention time of 29.7 months, compared with the 26.6 months retention time of those without such perforation. However, the retention time was not significantly associated with TM perforation. The histories of OME and AOM were not associated with TM perforation.
A Multivariate Analysis of the Significant Factors Associated With the First Ventilation Tube Characteristics Related to Persistent TM Perforation.a
Abbreviations: AOM, acute otitis media; OME, otitis media with effusion, VT, ventilation tube.
a For continuous predictors (age and tube retention period), the OR represents the increase in the odds of the outcome with every single-unit (month) increase in the input variable.
Multiple VT Insertions
The average second VT retention period was 20 months (between 1 and 63 months). We were unable to follow 38 ears after the second VT insertion and 7 ears after the third VT insertion due to referral to another hospital or an ENT clinic and self-interruption of treatment. Persistent TM perforation was not observed in the groups that had 4 or 5 VT insertions.
The Survival Rate of VT by Anesthesia Type
The Kaplan-Meier curve for the survival of the first VT insertion by local or general anesthesia is shown in Figure 4. No significant difference was observed in the time before spontaneous VT extrusion depending on the type of anesthesia (P = .691).
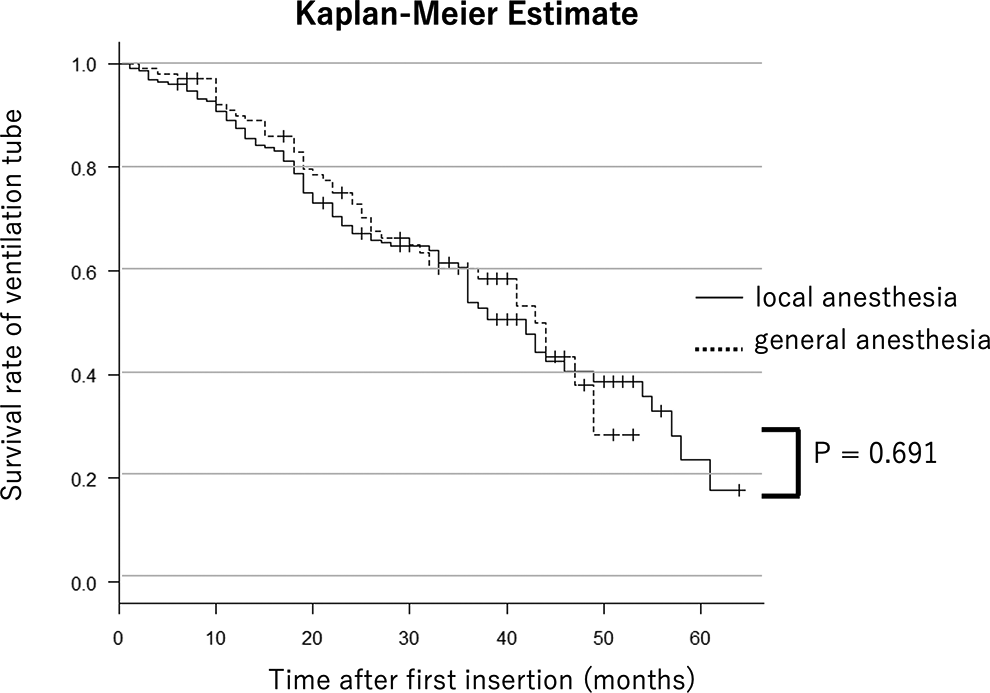
Kaplan-Meier curve for the first ventilation tube insertion’s outcome.
Discussion
We showed that a short VT retention period and spontaneous removal of VT were associated with OME recurrence. Male sex was associated with persistent TM perforation after VT removal. Interestingly, the duration of VT insertion and the risk of persistent TM perforation were not significantly associated. The risk of persistent TM perforation after multiple insertions was not higher than that after single insertion. In addition, we showed that the VT tube survival according to the time course was not significantly different between local and general anesthesia.
We used a single kind of long-term VT (Koken B-type VT) for all patients. The Koken B-type VT is one of Japan’s most frequently used tubes and is classified as a long-term VT. According to the 2015 clinical practice guidelines for diagnosing and managing OME in children in Japan, short-term tubes should be selected for the first VT placement, and long-term tubes should be selected when performing surgery in pediatric patients with recurrent OME that seems intractable. 8 The short-term tubes are spontaneously removed at 8 to 16 months after insertion. The reason for selecting short-term tubes for the first insertion is that an estimated 50% to 80% of the patients can be successfully cured without perforation. In our series, patients whose VTs were removed between 8 and 16 months (3-6 quarters in Figure 3) had a high percentage of OME recurrence. Patients with intractable otitis media and recurrent otitis media are often referred to our institution from other clinics and hospitals. Thus, our institution uses only Koken B-type VT. A study comparing several different kinds of VT showed that the group with VT insertion for ≥3 years had a 15% (26/172) chance of perforation, and the group with insertion for <3 years had a 3% (3/101) chance of perforation. 3 Another group showed that VT duration was not associated with TM perforation, but the type of VT (long-term VT) was associated with perforation. 6 These 2 studies analyzed patients treated with several different kinds of VT and did not eliminate confounding. Based on the findings from these studies, it is difficult to estimate the effect of the VT retention period and types of VT on TM perforation, although it is intuitively reasonable to assume that these factors are associated with TM perforation to some degree. In contrast, our data were obtained from patients treated with a single kind of VT, thus eliminating the effect of the VT on the outcome so that we can focus on the crucial clinical factors. The relatively high perforation rate of 17% may be because the Koken B-type VT used in our series is a long-term tube.
The OME recurrence was observed in 29% (96/326) of the ears after single VT insertion. The rate of OME recurrence is comparable to that in previous studies. A study of a mixture of several types of VT showed that 14.4% of patients required at least 1 additional insertion. 7 Another study with a single type of VT tube (Goode T silicone tube; inner diameter: 1.14 mm, length: 12 mm) showed that 25% of ears had recurrent OME. 5 The factors associated with OME recurrence were the period of VT insertion and spontaneous removal of VT. The cutoff point calculated with a Youden index of 25 months was consistent with the commonly accepted insertion period of 2 years. 12 Considering this calculated cutoff point of 25 months, we recommend a VT retention period of at least 2 years. Our analysis showed that that intentional removal was better than spontaneous removal with regard to the OME recurrence risk. We have no clear-cut explanation for this result, as OME recurrence depends on the Eustachian tube function and not on the status of the TM itself. However, in cases of intentional removal, a relatively high but not significant incidence of TM perforation (Table 4) might be the reason for the low OME recurrence (Table 3). When the Eustachian tube is underdeveloped, then OME can occur. However, when a TM perforation occurs, then OME does not develop due to the fact that effusion in the middle ear drains out through the TM perforation.
The overall rate of persistent TM perforation in our patients receiving the first VT insertion was 17%. This is in concordance with previous studies, which reported rates ranging from 4.8% to 28%. 1,3,5 -7,13 In 1998, Nichols et al 13 retrospectively found that the TM perforation rate was significantly higher in pediatric patients with VT retained for more than 36 months than in the groups with VT retained for less than 36 months (P = .02). A study with intentionally planned VT removal timing identified that the rate of permanent TM perforation significantly increases at 18 months after tube insertion (P = .008). 5 In our study, there was no significant difference in the TM perforation rate based on the tube retention time. However, there was a tendency for an older age at VT insertion to be associated with TM perforation, albeit without statistical significance. There have been few studies on the association between an older age and TM perforation. El-Bitar et al12 reported that the occurrence of complications (granulation tissue, persistent otorrhea, and permanent TM perforation) due to tube retention was higher in children aged 7 years and older than in younger children. However, they did not perform a multivariate analysis to eliminate the effect of confounding factors, and they attributed the higher complication rate in the older group to the prolonged retention period. Vercillo et al also reported that older children tended to have an increased risk of persistent TM perforation. However, older children receive long-term tubes more frequently than younger children. 6 These authors did not perform a multivariate analysis either, so it is not reasonable to conclude that older patients are associated with complications based on these previous findings. In our study, even after eliminating the effect of confounding factors, there was a tendency for an older age at VT insertion to be associated with TM perforation. Further studies are needed to clarify this phenomenon.
Given the results of the present study, the optimal timing for VT removal in patients without otorrhea might be after at least 2 years’ retention. The possibility of OME recurrence decreases after 25 months; however, the possibility of permanent TM perforation does not increase with a longer retention period. The timing may need to be decided based on a patient’s age at removal. The Eustachian tube function typically develops around 7 years old, and the risk of relapsing OME decreases around this age. It is generally considered that as soon as patients’ Eustachian tube function is deemed adequate, the VT should be removed, as VTs are associated with various complications, including granulation tissue formation, cholesteatoma formation, tube extrusion into the middle ear space, and persistent perforation. 3,14 However, evaluating the Eustachian tube function of children accurately is not always possible, and the outcome after VT removal cannot be predicted perfectly. Since a longer retention is not associated with permanent TM perforation, one potential strategy is to remove a VT at around 7 years old when the retention period exceeds 2 years.
Children older than 7 years who need VT might have other conditions, such as allergy and atopic disease. The middle ear is part of the upper respiratory tract—allergic rhinitis and bronchial asthma—therefore likely play a role in intractable OME. 15,16 Unfortunately, we did not review the allergy status of the children.
The rate of persistent TM perforation was significantly higher in male patients than in female patients, in contrast to the findings in previous studies that reported no significant differences between sexes. 5,13 The reason for this association is unclear, but a possible explanation is different hormonal levels between sexes and their effects on wound healing. Estrogen affects wound healing positively, while androgens regulate cutaneous wound healing negatively. 17
In our study, 96 (29%) and 28 (8.6%) patients required 1 and ≥2 additional VT insertions, respectively. In contrast, Padia et al7 reported that 19.0% and 4.6% of patients required at least 1 and ≥2 additional insertions, respectively. The type of VT used for the patients was not mentioned in their study. Choi et al 18 reported that 36.5% received multiple insertions among 126 ears in children younger than 12 years who had received insertion of a Paparella type 1 VT (short-term VT; silicone, inner diameter: 1.14 mm, diameter of the inner flange: 2.4 mm, diameter of the outer flange: 2.1 mm, length: 2.2 mm). Persistent TM perforation was not observed in patients who had received VT insertion 4 or 5 times in our study (Figure 2), suggesting that there is no ostensible need to worry about TM perforation due to multiple VT insertions. We did not analyze the factors associated with the recurrence of OME or persistent TM perforation in cases with multiple VT insertions because of the small sample size. However, previous studies have described the factors associated with multiple VT. Patients with recurrent OME generally require multiple VT. Therefore, the factors associated with multiple VT may also be associated with recurrent OME. A previous study showed that male sex, asthma or reactive airways, gastrointestinal disease, and prematurity were associated with multiple VT insertions. 19 Another study showed that attending large daycares, being breastfed for <3 months, atelectatic TM, and smoking parents were associated with multiple VT insertions. 20 Therefore, for children with potential risk factors for multiple VT insertions, that is, those with prolonged Eustachian tube dysfunction, the standard retention period of a VT might need to be longer than 2 years. The factors associated with persistent TM perforation in multiple VT insertions have not been reported.
In the present study, 16 (5%) patients in the first VT insertion group required tube removal for persistent otorrhea. A meta-analysis study showed that 3.8% of patients with VT had chronic otorrhea. 11 In particular, the RR of acquiring otorrhea requiring tube removal increased by 7.7 times when long-term tubes were used compared to short-term tubes (P < .001). 11 As such, a relatively low incidence of persistent otorrhea with long-term tubes, such as the Koken B-type VT, is tolerable.
The accuracy of VT insertion under local anesthesia is a concern for outpatient clinic otolaryngologists. Our results indicated that the anesthesia method did not significantly influence the rate of VT spontaneous extrusion. Therefore, we believe that our results will contribute to the selection of appropriate treatment methods. The VT insertion under local anesthesia has several benefits over that with general anesthesia, including a low cost, time-saving nature, and lack of side effects related to general anesthesia. However, older children are not the good candidates for local anesthesia, as they have difficulty standing still. Furthermore, the psychological effects on children who remember being subjected to forceful VT insertion should be considered. The type of anesthesia should thus be chosen depending on each patient’s background.
Several limitations associated with the present study warrant mention. First, we did not evaluate continuous conductive hearing loss before VT insertion because this study also included a preschool pediatric population. Second, certain patients were unable to be followed until the outcome of VT was revealed due to their referral to another hospital or ENT clinic and the patient’s self-interruption of treatment. The actual outcome might be, therefore, have been better than shown in this study, as patients in whom OME recurred and who had TM perforation were more likely to be re-referred to our hospital than cured patients. Third, our sample size was small, especially in cases of multiple insertions. Thus, we did not analyze the factors associated with the recurrence of OME or persistent TM perforation in cases with multiple VT insertions. Finally, we did not review other factors associated with the development of recurrent OME, such as the allergy and atopic disease status.
The main findings in this study are (1) a longer retention period of VT is associated with decreased OME recurrence, but not with permanent TM perforation; (2) the risk of persistent TM perforation after multiple insertions was not higher than after a single insertion; and (3) the VT tube survival according to the time course was not significantly different between local and general anesthesia. These findings led to the development of the following strategy: (1) The retention period of the VT should be at least 2 years, and removal at 7 years old might be viable; (2) multiple VT insertions are recommended for patients with recurrent OME; and (3) VT under local anesthesia is an effective option for children able to tolerate it.
Conclusions
A certain period of VT retention is necessary to avoid OME recurrence. The retention period of VT should be at least 2 years, and VT removal at 7 years old might be a viable strategy. Multiple VT insertions were not associated with persistent TM perforation and should, therefore, be recommended for patients with recurrent OME. Furthermore, there is no apparent need to worry about TM perforation due to multiple VT insertions. Insertion of VT under local anesthesia has no disadvantages over insertion via general anesthesia in terms of the VT survival period. Ventilation tube under local anesthesia is, therefore, an effective option for tolerable children.
Footnotes
Authors’ Note
All procedures performed in this study were in accordance with the ethical standards of the institutional research committee and conformed to the 1964 Helsinki Declaration and its later amendments. This was a retrospective chart review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI (grant number JP 19K08948).